
記住我



Tumor histotype, standard morphological parameters, and grade of the 64 MUOs are reported in Table 1. Fifty-four (84.4%) cases showed clear-cut cytohistological features of carcinoma. Of these, 40 (74%) were classified as adenocarcinoma, 11 squamous (20.3%), and 3 neuroendocrine carcinomas (5.5%). Ten cases (15.6%) did not show clear-cut features of epithelial malignancy; 5 of these (50%) were classified as undifferentiated tumors and 5 as sarcomatoid tumors (50%).
Table 1 Histotype, architecture, cell features, and grade of 64 MUOOf the 54 cases defined at histology as carcinomas, the majority were either G3 (53.7%) or G2 (37%), while 9.3% were G1 (p < 0.01) compared to the undifferentiated and sarcomatoid tumors, which were consistently classified as G3.
Immunohistochemical workupMUOs with clear-cut carcinoma histologyAdenocarcinomas were the most represented (n = 40/64, 62.5%) and required relatively extensive immunohistochemical analysis to formulate the diagnosis of provisional CUP and then exclude the presence of a primary tumor by imaging to reach the diagnosis of confirmed CUP [2, 10]. Women and men were 27 (67.5%) and 13 (32.5%), respectively, with a trend of significance for higher women representation compared with the non-adenocarcinoma CUPs (p = 0.087).
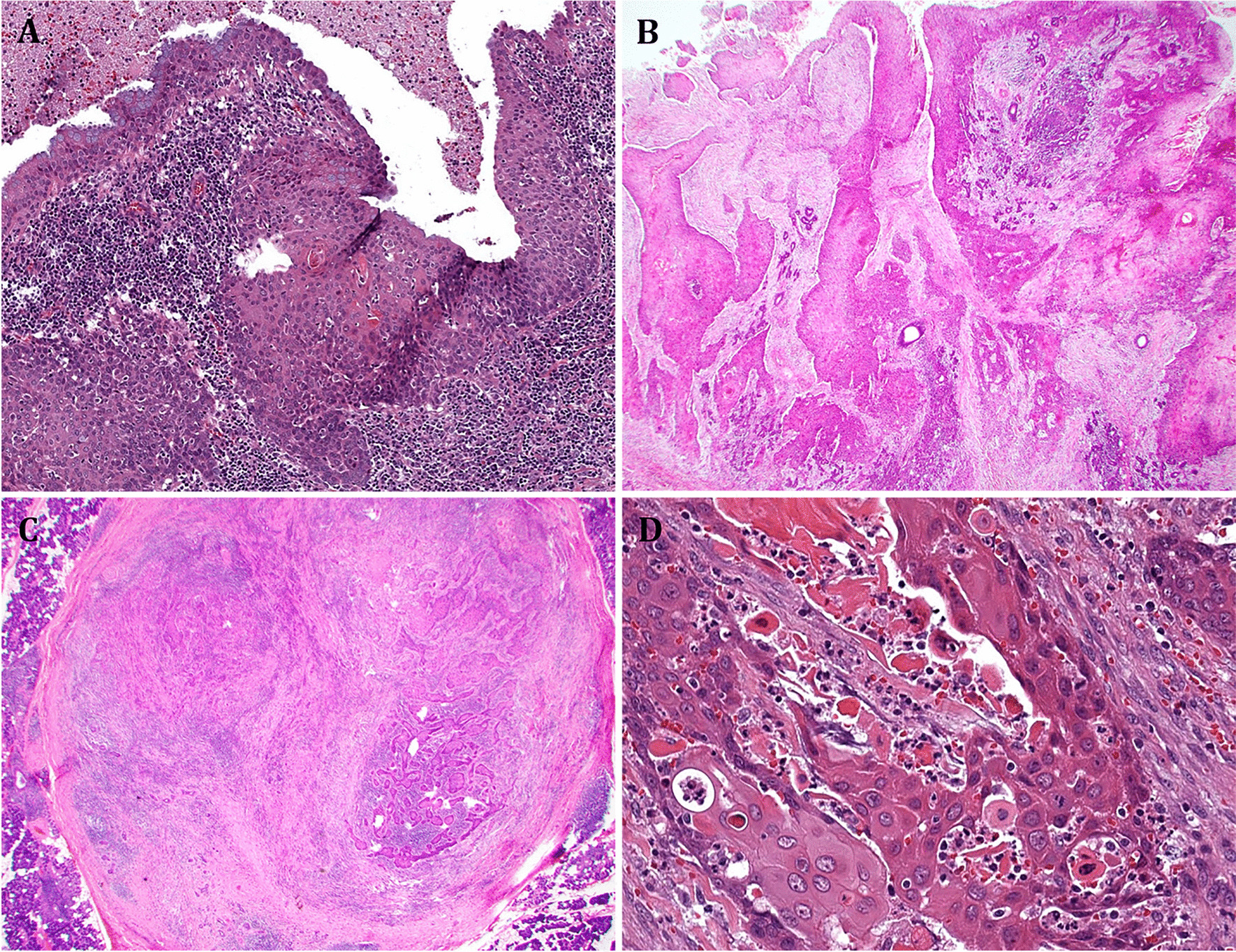
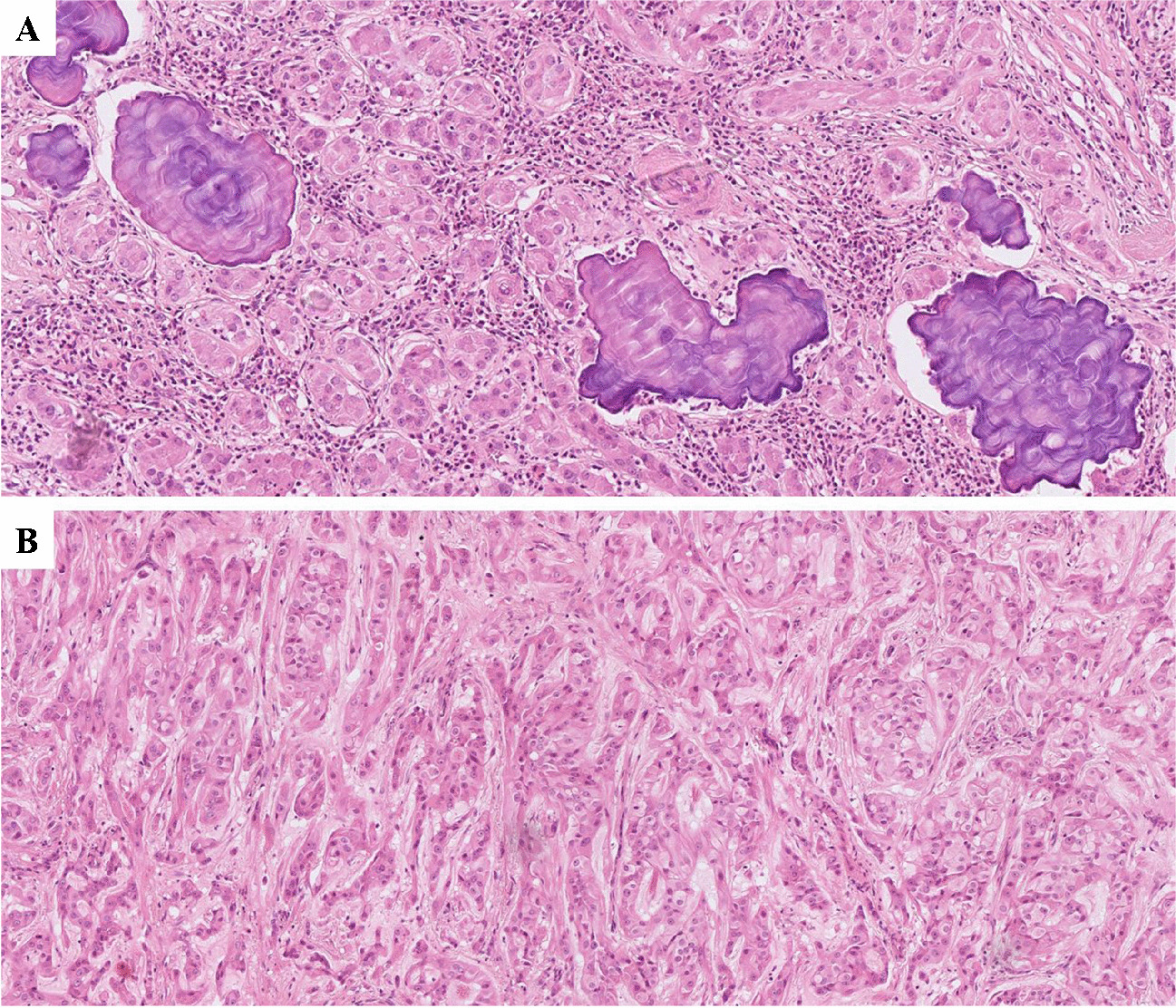
Histological revision identified 7/40 (17, 5%) early metastatic adenocarcinomas. Two lobular breast cancers (AGN40 and EM01/14.15, liver (Fig. 1A) and ovary (Fig. 1B) metastases, both resulted CK7 + /CK20 − and estrogen receptor (ER) score 3. Microfollicular structures were identified on deeper histological sections of a single metastasis in a latero-cervical lymph node, diagnosed at another institution as CUP, TTF1 + (CUP17/8.15) (Fig. 1C). Thyroglobulin expression further confirmed the thyroid origin. AGN336 patient was incidentally discovered with lung and liver localizations after a CT scan for SARS-CoV2 infection. The liver core biopsy was sent to our institution for consultation as “adenocarcinoma ER/TTF-1/GATA3/CDX2 negative, possible CUP.” Based on the morphology of well-differentiated glands in sclerotic stroma, a diagnosis of “intrahepatic cholangiocarcinoma” (Fig. 1D) with lung metastases was given, and the patient was treated accordingly. The tumor was CK7 + /CK20 − /ER − and DOG-1 score 1. AGN329 patient presented with a single localization within the ileo-psoas muscle; her biopsy was sent to our service for consultation as CUP, vimentin score 1 + , and calretinin − /SOX10 − /CD10 − . Based on morphology (Fig. 1E), we suspected a gynecologic origin, which was confirmed by ER, PAX8, and WT1 positivity. The patient had an endometrial biopsy diagnosed as G1 papillary endometrioid carcinoma of the uterus, and the case was reclassified as early metastatic carcinomas. AGN343 patient had a pseudomyxoma peritonei (CK7 − /CK20 score 3 + /CDX2 score 3/SABT2 score 1, and ER − /PAX8 − /WT1 −); she underwent right and transversal colectomy during debulking, but neither primary cancers nor polyps were identified. Pancreas and stomach were not affected by any lesion. The patient was treated as carrying a tumor of colorectal origin KRAS mutated (see Fig. 6, ONCOCARTA result). In AGN52, biopsy of a bone metastasis showed signet ring cells at histology (Fig. 1F). WT1 and CDX2 showed both score 1 expression, and TTF1 was negative. The histology-driven endoscopy detected a primary gastric adenocarcinoma.
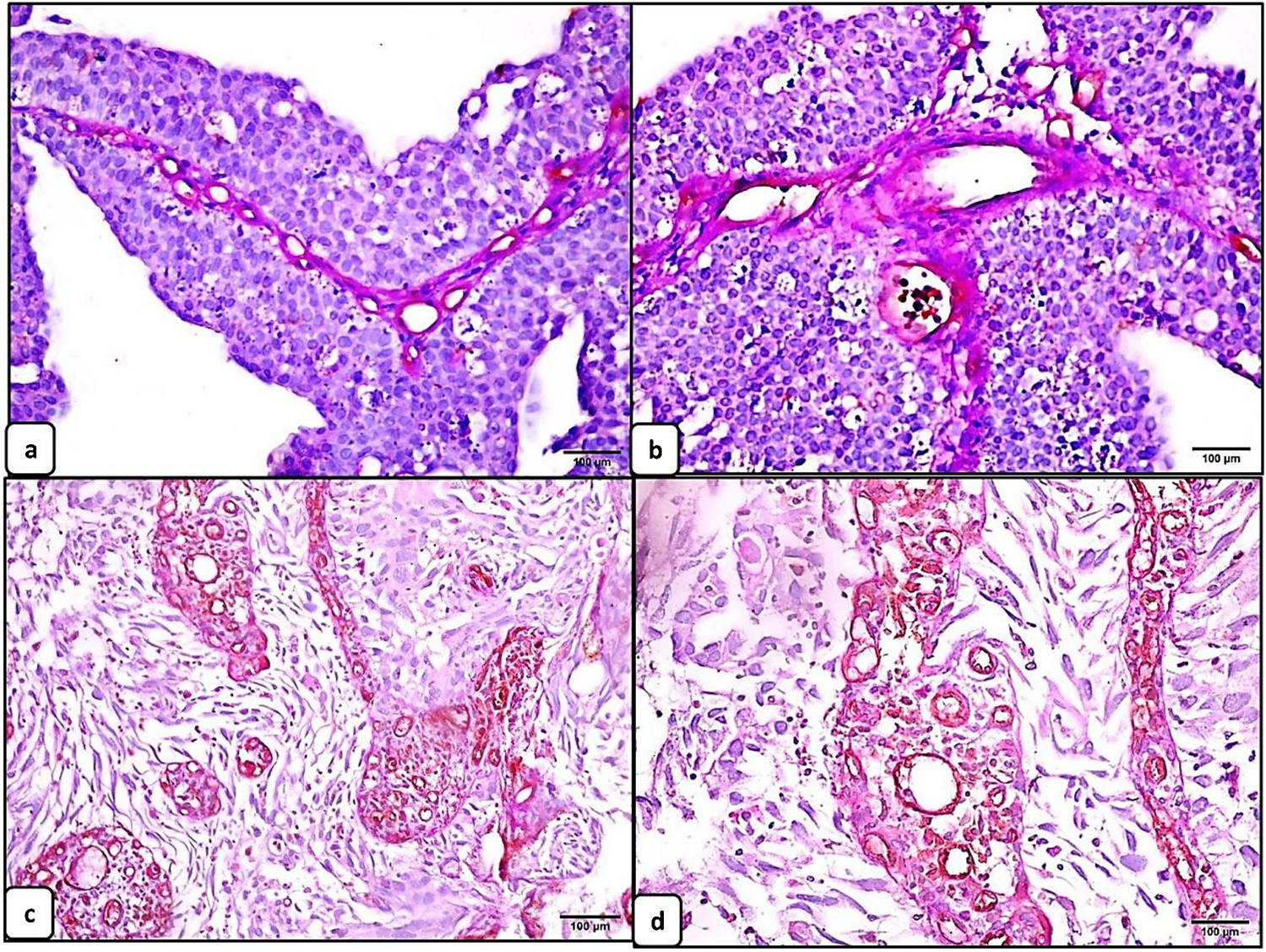
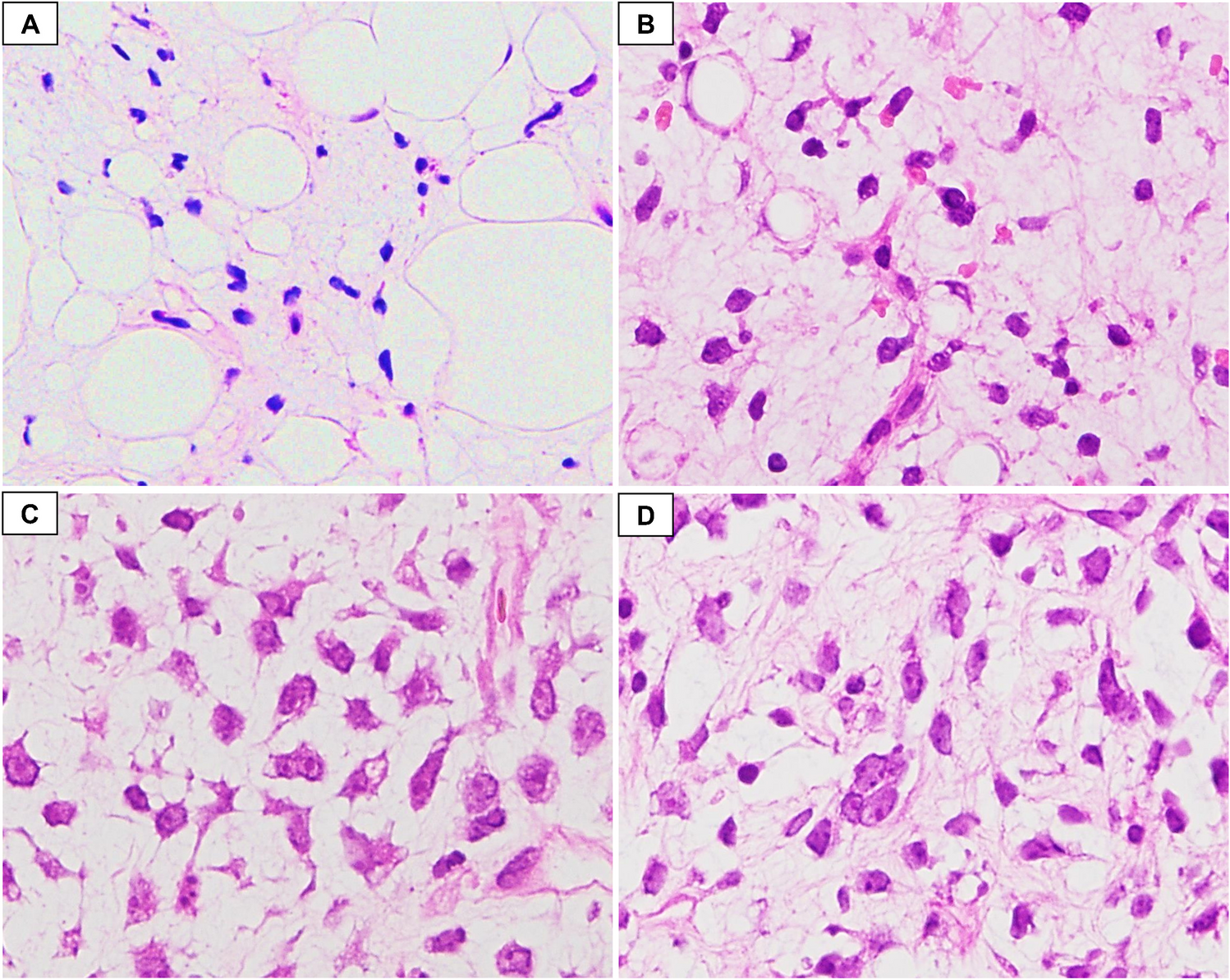
Fig. 1
Cytohistological patterns suggestive of tissue of origin. A AGN40 liver and B EM01/14.15 ovary biopsies of lobular breast cancer metastasis; C CUP17/8.15 latero-cervical lymph node biopsy of follicular thyroid carcinoma; D AGN336 liver biopsy of intrahepatic cholangiocarcinoma; E AGN329 ileo-psoas muscle biopsy of G1 papillary adenocarcinoma metastases; F AGN52 bone biopsy of signet ring cell gastric cancer metastasis
The remaining 33/40 adenocarcinomas were all tested using anti-CK7/CK20 antibodies. Thirty-eight other IHC markers, used in different combinations by pathologists, were recorded in this set. We selected the immunostaining score values of the 10 most recurrent tissue-specific markers to produce a heatmap (Fig. 2) and to evaluate their impact on ruling out CUP diagnosis. A “putative immunophenotype” of potential tissue of origin was suggested based on the results of tissue-specific markers. Except for CK7, the expression score was generally lower in confirmed CUPs than in non-CUP cases.
Fig. 2
Heat map of tissue-specific marker scores in MUO adenocarcinoma. Heat map depiction of immunohistochemical scores of the most representative tissue-specific markers used in the diagnostic workflow. Data are sorted based on the “putative” immunophenotype (IHC phenotype). Each row represents one case. Columns represent patient identification code (ID), site of biopsy, patient age, patient gender (female: F, male: M), tumor grade (grade 1, grade 2, grade 3), immunohistochemical scores of tissue-specific markers (IHC score): 0 = < 5% of neoplastic cells stained; 1 = 5–10% of neoplastic cells stained; 2 = 11–50%; 3 = > 50% of neoplastic cells stained; white fields: not performed; confirmed cancer of unknown primary (CUP)/early metastatic cancers (EM). (AGN913)*two biopsies of the same patients
In 10/33 cases (30, 3%) (3 women and 7 men), none of the markers was convincing for any “flavor” of tissue of origin (undefined immunophenotype), nor any instrumental examination ratified a primary tumor, directly leading to the definition of confirmed CUPs. One of these patients (AGN913) had biopsies of obturator and retrocaval lymph nodes 2 years apart that maintained the same “undefined profile” (CK7 + /CK20 − /ER − /TTF1 − /GCDFP15 score 1). AGN43 has been described previously [8]. During “warm autopsy,” samples of different anatomical sites of metastases were collected, and 16 different tissue-specific markers were performed, but none of them were useful to define the primary tumor.
In the remaining 23/33 (69.7%) adenocarcinomas, all tested for CK7/CK20, a putative immunophenotype was suggested setting the premises for further diagnostic exploration in related organs. Following imaging and/or endoscopy guided examinations, in 9/33 (27.2%) cases, an early metastatic tumor was found, while in the remaining 14/33 (42.4%), the primary was not found, leading to the diagnosis of confirmed CUP.
All CK7 + /CK20 − and CK7 + /CK20 + biopsies from women were tested for estrogen receptors (ER). CK7 + /CK20 − /ER + immunophenotype per se, independently from the ER IHC score, identified 2 out of the 6 early metastatic breast cancers. GATA3 was considered as a breast cancer marker in CK7 + /CK20 − /ER − female adenocarcinomas, and other 2 early metastatic breast cancers were identified. In both CK7 + /CK20 − /ER + (1 case) and CK7 + /CK20 + /ER + (2 cases) adenocarcinomas, PAX8/WT1 expression was performed to rule out gynecological cancers. All cases showing a putative gynecologic immunophenotype were diagnosed as confirmed CUP.
In CK7 + /CK20 − male and in CK7 + /CK20 − /ER − female adenocarcinomas, TTF1 and/or napsin A were the first option, to exclude the lung origin. If TTF1 and or napsin A were positive (4 cases), pathologists generally did not proceed with other markers. Positron emission tomography (PET) and computed tomography (CT) scan confirmed a possible primary lung cancer in 3 patients, and they were studied for treated consequently.
In CK7 + /CK20 + /ER − and in CK7 + /CK20 − cases, CDX2/DOG1 expression suggested a putative biliopancreatic immunophenotype. Two out of seven cases resulted to be early metastatic cholangiocarcinomas.
In squamous cell and neuroendocrine carcinomas, 24 and 12 different IHC markers were tested, respectively; none were useful to rule out CUP, but only to confirm the cell lineage differentiation of the tumor (Fig. 3A and B). Only the brain biopsy of AGN331 was p16 positive out of 4 squamous carcinomas tested, suggesting a possible HPV-related cancer of the upper respiratory or genital tract, which was not confirmed at further examinations.
Fig. 3
Heat map of tissue-specific marker scores in squamous and neuroendocrine carcinomas. Heat map depiction of immunohistochemical scores of the most representative tissue-specific markers and cell lineage markers used in A squamous carcinoma and B neuroendocrine carcinoma. Results are not sorted. Each row represents one case. Columns represent patient identification code (ID), site of biopsy, patient age, patient gender (female, male), tumor grade (grade 1, grade 2, grade 3), immunohistochemical scores of tissue-specific markers (IHC score): 0 = < 5% of neoplastic cells stained; 1 = 5–10% of neoplastic cells stained; 2 = 11–50%; 3 = > 50% of neoplastic cells stained; white fields: not performed; confirmed cancer of unknown primary (CUP)/early metastatic cancers (EM)
MUOs with unclear carcinoma histologyUndifferentiated tumors (2 women and 3 men) were investigated with an extensive panel of cytokeratins to confirm their epithelial nature and then with different tissue-specific and cell lineage markers (18 different markers). Excluding the laparoscopic omental biopsy of an undifferentiated tumor expressing Melan A, S100, chromogranin A, and synaptophysin, which led to the endoscopic identification of an intestinal melanoma with aberrant neuroendocrine differentiation, the other cases lacked any tissue-specific marker and were confirmed as CUPs (Fig. 4A). Sarcomatoid tumors were primarily studied with pan-cytokeratins to exclude not epithelial cancers. Fifteen other markers were used; none of them were useful to identify/suggest a tissue of origin (Fig. 4B).
Fig. 4
Heat map of tissue-specific marker scores in undifferentiated and sarcomatoid tumors. Heat map depiction of immunohistochemical scores of the most representative tissue-specific markers and cell lineage markers used in A undifferentiated and B sarcomatoid tumors. Results are not sorted. Each row represents one case. Columns represent patient identification code (ID), site of biopsy, patient age, patient gender (female, male), tumor grade (grade 1, grade 2, grade 3), immunohistochemical scores of tissue-specific markers (IHC score): 0 = < 5% of neoplastic cells stained; 1 = 5–10% of neoplastic cells stained; 2 = 11–50%; 3 = > 50% of neoplastic cells stained; white fields: not performed; confirmed cancer of unknown primary (CUP)/early metastatic cancers (EM)
Histology-driven algorithm for MUO diagnosisTaking into consideration the results described above, we designed a 4-step workup (Fig. 5).
Fig. 5
Workup of MUOs. A 4-step workup is shown. 1st step: differentiation of MUOs in clear-cut and not clear-cut carcinomas. 2nd step: definition of the histotype. 3rd step: selection of specific immunoistochemical (IHC) tissue markers based to the results of step 2. 4th step: selection of the diagnostic exploration in related organs or comprehensive imaging to confirm the diagnosis of CUP or early metastatic cancer (EM)
This algorithm considers “histology” as the guiding parameter of the diagnostic cascade of MUOs, with the intent to define those with clear-cut carcinoma characteristics. This first step followed the definition of the specific tumor histotype in the two sets of MUOs. In adenocarcinomas, cytohistological features per se solved MUOs origin in 7/17 cases, identifying 41% of early metastatic cancers. If no pathological characteristic of a specific organ has been recognized, in adenocarcinomas, the expression of CK7/CK20, along with the sex and site of metastases, headed to the selection of specific IHC markers to define an alleged source tissue immunophenotype, which in turn guided targeted diagnostic investigations. This pathway led to identify 9/17 (53%) early metastatic adenocarcinomas. In squamous and neuroendocrine carcinomas, the site of metastases and the patient gender were not considered to posit a tissue of origin, and each patient was studied with PET and CT. All were diagnosed as confirmed CUP. The epithelial nature of cancers without clear features of carcinoma was tested using many different pan-cytokeratins and other markers of cell differentiation, which identified one melanoma (5.8% of early metastatic cancers).
Comparison of clinical and pathological characteristics of confirmed CUP and early metastatic carcinomasOf the 64 MUOs, 47 (73.4%) were confirmed CUPs, and 17 (26.5%) were early metastatic cancers. Histotype (p = 0.045), grade (p = 0.04), and putative immunophenotype (p = 0.01) were significantly different between confirmed CUP and early metastatic cancers, as shown in Table 2.
Table 2 Clinical and pathological comparison of confirmed carcinoma of unknown primary (CUP) and early metastatic cancers (EM)CUP genetic analysis by ONCOCARTAThe oncoprint in Fig. 6 summarizes the genetic analysis by the ONCOCARTA gene panel that explores more than 230 somatic mutations across 19 actionable oncogenes frequently mutated in human cancers.
Fig. 6
Oncoprint. The graph reports the DNA mutations identified in the cohort of 37 CUPs analyzed by targeted sequencing. Gene names and relative frequency of mutations are reported in the double y-axis. The bar graph in the top of the oncoprint defined the number of variant/sample. Histology, phenotype, gender, tumor grade, and alive status are annotated at the bottom of the plot. ADK: adenocarcinoma, NEC: neuroendocrine carcinoma, NOS: not otherwise specific or undifferentiated tumors
The leftover of FFPE tissue after the IHC study was adequate for molecular analyses in 37/47 CUP cases (78.7%). Twelve out of the 37 cases (36%) showed at least one mutation; 10 of these were adenocarcinomas, 1 was SSC, and 1 was sarcomatoid carcinoma. The remaining 25 CUPs did not show any detectable alterations. KRAS and PI3KCA were the most frequently mutated genes and accounted for 75% of all the identified alterations. KRAS, BRAF, NRAS, and PIK3CA mutations were found with a mutually exclusive pattern. When subdividing by CUP histological type, the adenocarcinoma was the most frequently mutated (10/12 samples); in addition, only adenocarcinomas harbored KRAS mutations. The most mutated immunophenotypes of adenocarcinomas were the undefined (1 KRAS; 2 PIK3CA, and 1 BRAF) and the biliopancreatic (2 KRAS and 1 BRAF), followed by the gynecological immunophenotype (1 case with concomitant KRAS and PDGFRA missense mutation and 1 with PIK3CA mutation). The pseudomyxoma peritonei with intestinal immunophenotype (AGN343) showed KRAS mutation. One sarcomatoid carcinoma (AGN323) showed NRAS mutation. One SCC showed co-occurrence of a PIK3CA and a HRAS mutation. CUPs showing NE differentiation were wild type for the evaluated genes. No specific correlation was found between specific mutations and immunophenotype, sex, histological grade, or survival status.
Clinical impact of CUP histology and immunophenotypeIt is known that CUP patients with only lymph node metastases have a better OS [11]. Thus, we focused on confirmed CUP patients and assessed the site of first metastases, the site of progression, and their possible correlation with the histotype and, in the case of adenocarcinomas, with the putative immunophenotype (Tables 3 and 4).
Table 3 Evolution of CUP with lymph node localization at diagnosisTable 4 Evolution of CUP with any localization (with or without lymph node) at diagnosisSpecifically, squamous cell carcinoma histotype and the “gynecologic immunophenotype” within adenocarcinomas presented frequently with lymph nodes as the solely involved organs. None of the patients within the “bilio-pancreatic” and “lung immunophenotype” of adenocarcinomas presented with lymph node involvement only. Patients with “undefined immunophenotype” of adenocarcinomas, undifferentiated, and sarcomatoid carcinomas frequently progressed, independently from the anatomical site of cancer at diagnosis. Altogether, 20/47 (42.5%) confirmed CUP patients had only lymph node metastases at first diagnosis, while 27 (57.5%) had metastases elsewhere (visceral and/or bone and/or muscle and/or brain) with or without lymph node involvement (Table 3) (Supplementary Figs. 1A and B). The time to organ progression other than lymph nodes or death for the disease was 6.4 months longer in patients with lymph node metastases only, independently from the number of lymph node involved and the regional location. Finally, the patients with only lymph node metastases at first diagnosis had a significantly longer OS (< 0.001), independently again from the number of lymph node involved and the regional location (sub- or supra-diaphragmatic) (Fig. 7).
Fig. 7
Overall survival (OS) analysis. OS survival curve for CUP patients, stratified for the site of the lesion onset (lymph nodes only versus all other sites with or without lymph node involvement). CUP patients who had only lymph node metastases at first diagnosis had a significantly longer overall survival (< 0.001) than the patients who had metastases elsewhere (visceral and/or bone and/or muscle and/or brain) with or without lymph node involvement
留言 (0)