Management for the segmental tubular bone defect often require appropriate treatment, prior literatures presented selectable strategy to reconstruct [16,17,18,19], most of their research shown satisfactory results and expectable abroad clinical application. In the condition of infection milieu, the illizarov bone transport and MIMT were acknowledged as the ideal management [4].
Although both the two techniques associate with uncertain bone union rates and long treatment time, surgeons often selected induced membrane technique as a priority owing to the in aesthetic appearance and inconvenience of illizarov external fixator [20], compared with traditional cylindrical bone transport fixator, the monoplane external fixator might means better tolerance for the patients during the lengthy bone tractive time, however, the deformity still appearance in the result of this substitute strategy [21], in addition, the technique was not suitable to reconstruct periarticular bone loss because of limited space to fix pins, and trans articular fixation may lead to stiffness and contracture of joint [4].
The MIMT with internal fixator seems to be solve the problems of illizarov bone transport, this alternative technique is also a feasible means to deal with infective bone defect of tubular bone and segmental bone defect adjacent joints [22], the main advantage is the immediately unrestricted range of motion practice after surgery which reduce the risk of myophagism, deep venous thrombosis and joint functional insufficiency [23], patients could achieve early functional exercise because the internal fixation and the autograft both contribute to establish a biomechanical stability. During first stage, the self-induced membrane is actually created by immune system, this characteristic combined with the loaded antibiotics will synergistically accomplish anti-infection in the process of bone reconstruction [3]. In the stage 2 of MIMT, segmental bone defect often requires huge volume of autologous and allogeneic bone which means enormous injury and may lead to chronic pain, fracture, hematoma and infection in the donor site [24].
In this study, we attempted to apply a novel means to improve the treatment in the second stage of MIMT, and, observed the stability of internal fixation and recovery of limb function, as a permanent implant, the postoperative imagine exam shown well osseointegration that no progressive relative movement between the implant and bone [25], through these indicators to infer the application prospect of 3D-printed porous tantalum. Previous study have already reported the 3D-printed titanium or tantalum prosthesis, with promising outcomes for the bone reconstruction, Li et al. [26] used a personalized 3D tantalum implant to reconstruct an approximately 12 × 8 × 6 cm bone defect after tumor removal, as an essential weight bearing skeleton of limb, there was no internal fixation failure and implant loosen present during the next 12 months. In the cases of bone necrosis and collapse, Mu et al. [27] applied customized talar prosthesis for arthroplasty after completely resection of talar, all cases achieved satisfactory results regarding pain relief and function recovery, a literature reviewed clinical result from revision surgery to oncologic reconstruction, indicated the good osseointegration, stably fixation and well biocompatibility of 3D-printed titanium or tantalum prosthesis [28].
The scaffold we designed was constructed with two parts, a porous prosthesis that made of tantalum was connected with a titanium locking plate, we choose porous tantalum instead of traditional titanium attributed to the better biomechanical and biological function of this metal, the material research conducted by Fan et al. [13] considered that cellular structure tantalum scaffold are superior to resist compression and deformation than titanium in similar construction. In an animal test, Ping et al. [29] concluded the tantalum with specific pore diameter and porosity has the biological ability to induce osteogenesis and osteointegration, prior study suggested the optimum porous diameter range was between 100 and 500 μm [30], additional research acknowledged the diameter of the pore in the porous structure greater than 300 μm promoted the formation of new bone and microcirculation [31]. Inheriting the above research, Li et al. [32] proceed a vitro experiment demonstrated that the porous diameter between 300 and 400 μm were more favorable to proliferation and osteogenic differentiation of the bone marrow stromal cells (BMSC). Therefore, in this study, we restricted the porous diameter and porosity, respectively, in 350 μm and 70%, to guarantee biomechanical stability and created a favorable osseointegration environment during the processes of bone repair.
Most of the infectious osteonecrosis in our study were located close to hip or knee joint and the minimum length of bone defect was 15 cm after debridement, all these cause great difficulty even for an experienced surgeon, the illizarov bone transport technique was the first excluded strategy as a result of considering the postoperative joint function [4], so MIMT was the ideal option. However, the bone graft in the stage 2 means abundant bone demand which may lead to multiple complication in the donor site [11]. Based on this consideration, we use the novel implant without bone graft in the stage 2, the length of the scaffolds could adjust according to specific length of bone defect in each case, another characteristic of the tantalum prosthesis is prominent structure allowed insert into the medullary cavity to partially enhance the connection with cancellous bone (Fig. 1). Furthermore, the whole implant was manufactured refer to the radiological exams, and the shape of the internal fixation was suitable to femoral anatomical characteristics. In open reduction surgery, this advantage indicates easier surgical procedure, less time and blood loss.
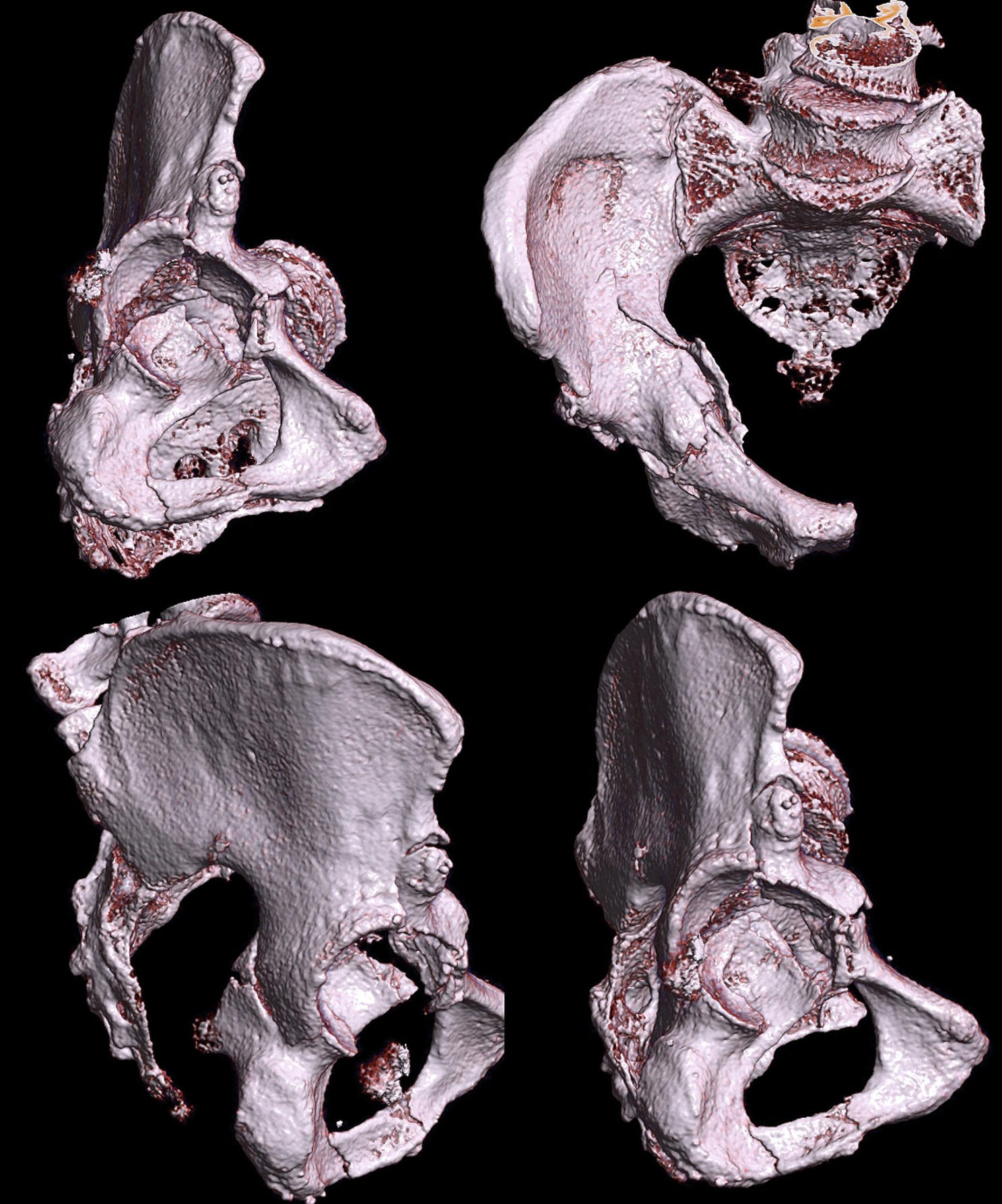
Although this study was preliminary clinical research, the result obviously shown encouragement outcomes, the limb deformity angle corrected from 5.5 (4.05, 5.75) degree preoperatively to 2.1 ± 0.76 degrees after surgery, without any changes by the last follow-up time, imagine test shown satisfactory osseointegration, Fig. 2 shown a special case with a length of femoral defect that approximately 20 cm. Moreover, both the remaining length of femur and morphology of the distal section posed great challenge for reconstruction, the illizarov and single MIMT technique was inappropriate to complete the re-establishment, and either traditional internal fixator could hardly enhance contact proportion with the cortex of femur [33], with the application of customized scaffolds and plate, the biomechanically stability was achieved and the prosthesis obtained enough contact proportion with the oblique fracture surface, which all benefit from the personalized shape of the implantation design [34]. However, the most meaningful limitation is the lack of comparison treatment group, and the selection bias may occur to influence the results of this research. Therefore, larger samples of this novel treatment and comparative studies with other means are required in the future.
This manuscript was not attempt to demonstrate that the 3D-printed porous tantalum scaffolds was omnipotent, in the treatment of weight-bearing long bone defection, each technology has advantage and drawbacks [4], the main purpose of our clinical research was trying to explore new path for bone reconstruction and offer more options for orthopedic surgeons.




留言 (0)