Following a prospective, randomised and single-centre research design, the current study included a total of 60 patients who underwent RC. The study was conducted at Beni-Suef University Hospital between April 2020 and January 2022. The ethical committee of the Faculty of Medicine, Beni-Suef University (FM-BSU), Egypt, approved the conduct of the study (Identifier: FM-BSU REC/08032020). The current study was registered at Clinical Trials.gov on 23/3/2020 (registration number: NCT04318158). All the participants confirmed their voluntary participation in current study by signing in the written informed consent form. The principles of the Declaration of Helsinki were followed for this study. Sixty patients of ASA grades I and II, from both sexes, aged between 50–70 years of age with a body mass index (BMI) of < 40 kg/m2 undergoing RC surgery were included in the study. Patients with ischaemic heart diseases, heart block, congestive heart failure, valvular heart disease, cerebrovascular disease, impaired kidney function, history of chronic liver diseases, coagulation disorders, infection near the site of needle insertion, history of allergic reactions to any of the study medications, previous abdominal surgery, and any neurological or neuromuscular disorder or history of seizures were excluded. The participants were randomly divided into three categories, each containing a total of 20 participants. Group B had patients who received a single shot US-guided TAP block on each side with 20 ml of 0.25% bupivacaine (Sunnypivacaine®, Sunny Pharmaceutical) + 2 ml normal saline; group BF had patients who received a single shot US-guided TAP block on each side with 20 ml of 0.25% bupivacaine + 1 µg/kg fentanyl dissolved in 2 ml normal saline (Fentanyl Hameln®, Sunny Pharmaceutical); and group BD had patients who received a single shot US-guided TAP block on each side with 20 ml of 0.25% bupivacaine + 1 µg/kg dexmedetomidine dissolved in 2 ml normal saline (Precedex®, Hospira Inc). Randomisation was achieved by using computer-generated random numbers, which were then placed in separate opaque envelopes and kept by a data administrator.
Anaesthetic Technique
All the patients under study underwent routine preoperative check-ups, haematological and biochemical analyses followed by cardiac evaluation. The study protocol was explained to all the participants including visual analogue scale (VAS) on the day of preoperative evaluation. Standard monitoring was established when patients were transferred to the operating room. The patient received midazolam 0.05 mg/kg IV 3 min prior to induction and ondansetron 4 mg IV. Anaesthesia was induced by 2–2.5 mg/kg propofol, 2 μg/kg fentanyl & 0.5 mg/kg atracurium for muscle relaxation. The patient was ventilated using a face mask with 100% oxygen at a rate of 4 L/min and isoflurane 1.2%. After 180 s, the patient was intubated using an appropriately sized cuffed oral tube. Anaesthesia maintenance was performed by isoflurane 1.2% in 100% O2 and intravenous fentanyl infusion at a rate of 1–2 μg/kg/hr. Muscle relaxation was continued by atracurium 0.1 mg/kg every 20 min. Mechanical ventilation was performed for all participants to maintain end-tidal carbon dioxide levels between 35–40 mmHg. Intravenous fluid requirements were assessed and provided to patients perioperatively, and normothermia was maintained throughout the surgical procedure. Blood loss was assessed from time to time using visual estimation technique ( blood loss measured in suction canisters and estimated in blood-soaked sponges and drapes) and compensated for.
Ultrasound-guided TAP procedure
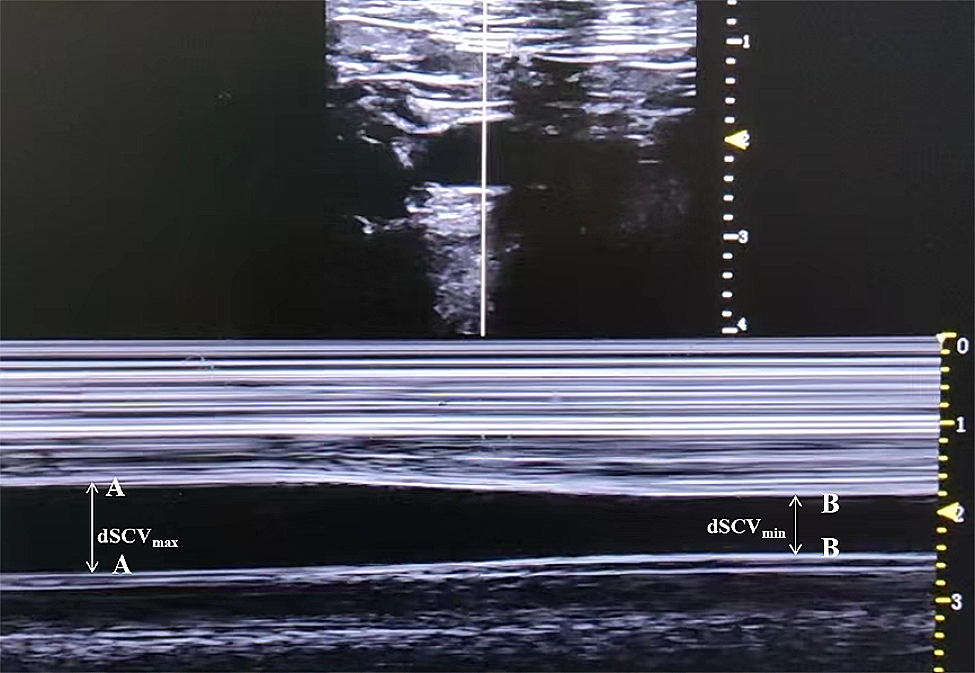
A TAP block was carried out, under US guidance, using the lateral approach after the completion of the surgical procedure and before extubation. The ultrasound used in the study was PHILIPS HD5 whereas the scanning probe was a linear array transducer L12-3 (3–12 MHz). In supine position, the lumbar triangle of Petit (formed anteriorly by external oblique muscle, posteriorly by lattisimus dorsi muscle, and inferiorly by iliac crest) was detected. After complete sterilisation, a linear US probe was transversely placed on the abdominal wall between the costal margin and iliac crest. The findings from above downward indicate the presence of skin, subcutaneous tissue and fat, external oblique, internal oblique, and transversus abdominis muscles. Both peritoneum and bowel loops were visualised deeper in the muscles. Once a TAP was identified between the internal oblique and transversus muscles, a 22-G 80 mm needle (Pajunk SonoPlex® STIM; Geisingen, Germany) was inserted in the plane using USG probe. Upon reaching the plane, 2 ml of saline was injected after negative aspiration of the blood to confirm the correct position of the needle. As categorised earlier, three groups received their respective doses as given herewith; group B had patients who received a single shot US-guided TAP block with 20 ml of 0.25% bupivacaine + 2 ml normal saline; group BF had patients who received a single shot US-guided TAP block with 20 ml of 0.25% bupivacaine + 1 µg/kg fentanyl dissolved in 2 ml normal saline; and group BD had patients who received a single shot US-guided TAP block with 20 ml of 0.25% bupivacaine + 1 µg/kg dexmedetomidine dissolved in 2 ml normal saline. Transverse abdominis plane was visualised by expanding with the injection. Thereafter, same procedure was repeated on the other side.
Recovery and postoperative management
At the end of the blockade procedure, any residual neuromuscular block was antagonised with neostigmine 0.04 mg/kg and atropine 0.02 mg/kg IV after which extubation was performed. When patients were found to be fully awake and vitally stable, they were transferred to the post-anaesthesia care unit (PACU) and kept under observation for 30 min prior to shifting to the surgical intensive care unit for 24 h.
Parameter recording
The duration of analgesia after surgery (i.e., time from TAP blockade to the first analgesic request in postoperative period) and the degree of pain (evaluated using VAS) were assessed. An anaesthetist explained the participants on how their pain will be assessed using a VAS scale in the range of 0 (no pain) to 10 (worst pain) [17]. Postoperative VAS score for pain was recorded immediately postoperatively and then at 2, 4, 6, 8, 12, 18, and 24 h at rest and movement. A score ≤ 3 was considered to be acceptable for pain relief. Supplementary rescue analgesia was administered in the form of nalbuphine IV 0.15 mg/kg (at VAS ≥ 4). Total analgesic consumption, in the first 24 h after the blockade, was recorded. The incidence and severity of postoperative complications such as hypotension, bradycardia, respiratory depression, sedation, nausea, and vomiting, during the first 24 h of postoperative period were also recorded. A categorical scoring system (0 = none, 1 = nausea, 2 = retching, and 3 = vomiting) was used to evaluate nausea and vomiting [18]. Sedation scores were evaluated using a sedation scale (0 = awake, 1 = drowsy, 2 = asleep but arousable, 3 = deeply asleep). Patients were considered sedated, if they had a sedation score of > 0 at any time, during the first 24 h after surgery [19]. Patient satisfaction (area of satisfaction was pain relief) was also assessed in the form of 1 = poor, 2 = moderate, 3 = good, and 4 = perfect [20]. The primary outcome was the time to the first rescue (TOFS) analgesia after TAP blockade. The secondary outcomes were the total dosage of rescue analgesia in the first 24 h after blockade, pain intensity after surgery at rest and movement during the first 24 h using VAS score, and adverse events, if any.
Sample size calculation
The sample size was assessed by comparing the time of the first analgesic request between patients treated with bupivacaine and dexmedetomidine (BD group), bupivacaine with fentanyl (BF group), and bupivacaine (B group) in ultrasound-guided TAP block in patients, who received RC. According to previous literature [17, 21], the mean ± SD of time to 1st analgesic request among BD participants was 9.8 ± 2.9 h, while in BF participants, it was 5.4 ± 1.5 h and in B group, it was 4.0 ± 0.7 h. So, the minimum sample size was calculated to be 16 patients in each group. In order to find the reduction in VAS score of 0.82 units, 20 samples per group is required with an expected drop rate of 5%. In another study conducted upon dexmedetomidine, the sample size of 20 was used. This sample size is sufficient to determine the real difference of 1 h with 80% power at α = 0.05, using One Way analysis of variance test. G*Power software version 3.1.2 for MS Windows (Franz Faul, Kiel University, Germany) was used to assess the sample size. Therefore, we recruited 20 patients per group to account for dropout.
Statistical analysis
The findings are described as mean ± standard deviation (± SD), median and range, or frequency (number of cases) and percentage. A Kolmogorov–Smirnov test was used to assess the normality of the numerical data. Group comparisons were carried out using a Kruskal–Wallis test with test as post hoc multiple 2-group comparisons after applying a Bonferroni adjustment for multiple comparisons for numerical data. A chi-square (c2) test was used for categorical data. An exact test was used instead when the expected frequency was < 5. Two-sided p values under 0.05 were defined as statistically significant. Data analyses were carried out in SPSS version 22.


留言 (0)