
記住我

Ambulatory blood pressure measurement (ABPM) has been shown to be the most cost-effective option to confirm a diagnosis of hypertension [1]. The reproducibility of average blood pressure (BP) taken by 24-h ABPM has been previously shown to be superior to the reproducibility of clinic BP [2–4]. However, the majority of studies examining ABPM reproducibility have been performed with time intervals of 12 weeks or less, or in individuals with long-term hypertension or a history of cardiovascular disease.
There are fewer studies comparing techniques for long-term monitoring and clinic BP remains a first-line tool despite well known risks from white-coat or masked hypertension [5–7]. Long-term monitoring using ABPM could facilitate improved BP control, but the degree of variability between sequential ABPM in normotensive and stable hypertensive individuals otherwise free from overt cardiovascular disease is poorly characterized.
A retrospective analysis of individual patient data (IPD) from randomized controlled trial (RCTs) provides an opportunity to investigate ABPM measurement variability. Here, we present analyses of measurement variability from three studies, which investigated possible benefits of dietary modification on ambulatory BP and arterial stiffness in individuals who were normotensive or with well controlled hypertension [8–10]. The concurrent measurement of pulse wave velocity (PWV) in these individuals presented an ideal opportunity to directly compare the reproducibility of PWV against that of ABPM, as superior reproducibility may support the alternate use of PWV as a long-term monitoring tool for cardiovascular health.
Even in a healthy population, reproducibility of BP measurements will be affected by blood pressure variability (BPV). Some degree of BPV is a normative property, but a high variability has been shown to be associated with an increased risk of cardiovascular outcomes, independent of the mean systolic pressure [11–13]. Determinants of increased BPV may include general cardiovascular risk factors such as increasing age, arterial stiffness and adverse lipid profiles [14,15] amongst others. Elucidation of factors associated with BPV in this cohort may provide clues to modifiable risk factors for high BPV in cohorts at a higher risk of cardiovascular morbidities.
Therefore, the primary aim of the present study was to calculate reproducibility associated with sequential ABPM in this relatively healthy population of normotensive and well controlled hypertensive individuals. Secondary aims were to estimate BPV and its potential determinants and to compare the reproducibility of arterial stiffness to that of ABPM for evaluation of its use as a surrogate technique for long-term measurement of vascular health.
MATERIALS AND METHODS Individuals and inclusion criteriaWe analysed IPD from three RCTs investigating the impact of dietary modifications on cardiovascular outcomes. Firstly, the Fruit & Veg study (ISRCTN50011192) tested whether a potassium-rich diet was beneficial for treatment-naive prehypertensive individuals (n = 48) [8]. Secondly, the MARINA study (ISRCTN666664610, n = 312) examined if increasing intake of long-chain n-3 polyunsaturated fatty acids favourably affected endothelial function and arterial stiffness [9]. Finally, the CRESSIDA study (ISRCTN9282106, n = 162) considered how following UK dietary guidelines, instead of a traditional British diet, might affect vascular function [10]. All study and trial procedures were performed at Guy's and St. Thomas’ NHS Foundation Trust. Each study was approved by a local research ethics committee.
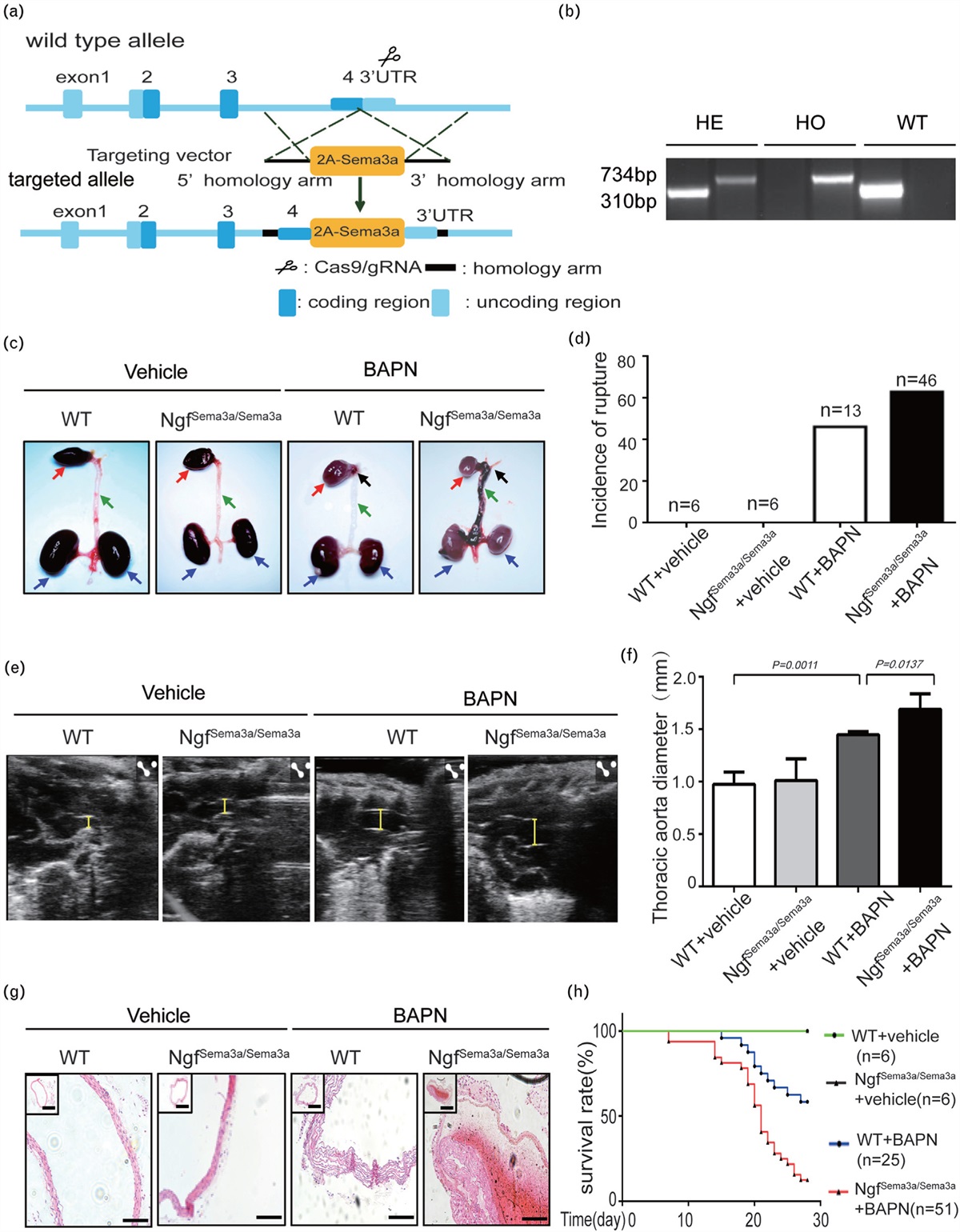
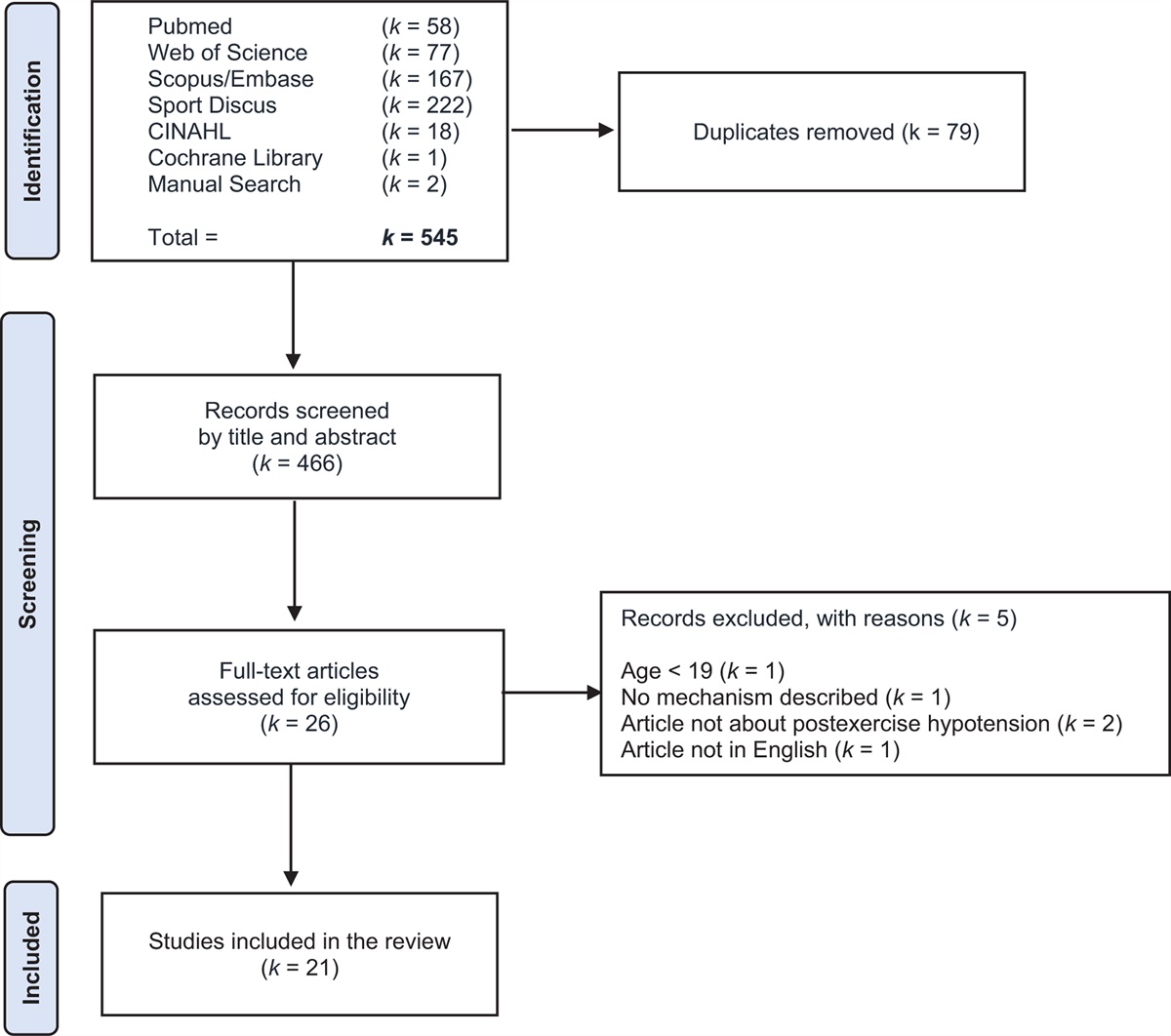
Data were eligible for inclusion and analysis if they fulfilled the following criteria: individuals must have had at least two ABPM and two PWV measurements, individual arms of each study did not show a significant change in BP measurements from baseline (statistical method detailed below) and no change in antihypertensive medications during the study. The second criterion ensured that any discrepancy between repeat measurements were secondary to measurement technique and physiological variability, rather than changes in an individual's true average BP (defined as a hypothetical estimate without measurement error and physiological variation [16]) resulting from dietary or other interventions. From the 522 available individual cases, 501 were retained in this analysis, as summarized in Fig. 1.
 FIGURE 1:
FIGURE 1: Consort diagram of the flow of individuals through the study. PWV, pulse wave velocity.
MeasurementsABPM measurements were performed with the A&D TM-2430 device (ScanMed, Moreton-in-Marsh, Gloucestershire, UK) in all studies. CRESSIDA and the Fruit & Veg study took five measurements of ABPM, whilst MARINA recorded three. The first baseline measurement for CRESSIDA was followed by a second baseline measurement approximately 3 weeks later, and then further measurements at 4, 8 and 12 weeks after the second baseline measurement. In Fruit & Veg, the first two measurements were approximately 6 weeks apart, and then subsequent measurements were every 11 weeks. MARINA measured ABPM at baseline, then 6 months and 12 months later. A full schedule of events can be found in Table S1, https://links.lww.com/HJH/C73 (in Supplemental Digital Content). ABPM devices were programmed to take measurements every 30 min from 0700 to 2200 h and hourly between 2200 and 0700 h, but daytime and night-time periods were defined by each participant according to a sleep diary.
PWV was measured by applanation tonometry of the carotid and femoral arteries using the SphygmoCor device (Atcor Medical, Sydney, Australia) after at least 15 min of rest. Further details of study procedures and study outcomes can be found in the published articles [8–10].
Nocturnal dippingNocturnal dip category was estimated for each ABPM session firstly according to a simple dichotomous outcome of dipper (night-time SBP fall ≥ 10% of daytime SBP) or nondipper (night-time SBP fall < 10% daytime SBP). Dipping status was then further defined according to the four classic dipping patterns (dipper: nocturnal SBP fall >10% of daytime SBP), reduced dipping (nocturnal BP fall 1–10% of daytime SBP), reverse dipping (increase in nocturnal SBP) and extreme dipping (nocturnal SBP fall >20% of daytime SBP) [17].
Data analysisTo verify whether individual arms of studies were eligible to be included in this analysis, repeated-measures analysis of variance (ANOVA) was used to assess if there were significant differences in BP across each study timeframe. If ANOVA demonstrated significance less than 0.05, posthoc pairwise comparisons were performed using the Bonferroni method between the initial and last ABPM measurement. Study arms were eligible to be included if the overall ANOVA significance was more than 0.05, or if P value was less than 0.05 but with no significant difference between the first and last measurement (see Table S2, https://links.lww.com/HJH/C73, Supplemental Digital Content, which details the sequential BPs for each study arm, and the significance of any differences). As such, all arms of the studies were considered eligible to be included in this analysis.
Correlations were tested with Pearson's correlation coefficient unless stated otherwise. Comparison of individual characteristics at baseline and study endpoint were compared with paired t-tests. Logarithmic transformation was used to calculate the within-individual coefficient of variation (CoV) and corresponding 95% confidence interval (CI) as described by Bland and Altman [18,19] for daytime, night-time and 24-h BP and heart rate (HR), and PWV. CoV was compared between normotensive and hypertensive individuals. Normotension was defined as baseline daytime SBP (SBPday) less than 135 mmHg, whereas hypertension was defined as baseline SBPday at least 135 mmHg.
Each individual had two to five measurements of SBPday, night-time SBP (SBPnight), daytime DBP (DBPday) and night-time DBP (DBPnight). The mean and standard deviation (SD) of these measurements was calculated for each individual. This intra-individual SD was used as an estimate of BPV for each individual. Multivariable linear regression models were used to analyse associations between patient characteristics and BPV, using an enter method.
Effect of regression to the mean (or adaptation to the ABPM device) was analysed using repeated-measures ANOVA in a subset of 199 individuals who had five ABPM measurements. Fleiss’ Kappa was calculated to determine agreement above chance in dipping categories.
Statistical tests were performed in SPSS version 25 (IBM, Chicago, USA), and significance defined as a P value less than 0.05. One author (L.K.) had access to all the data and takes responsibility for its integrity and the data analysis.
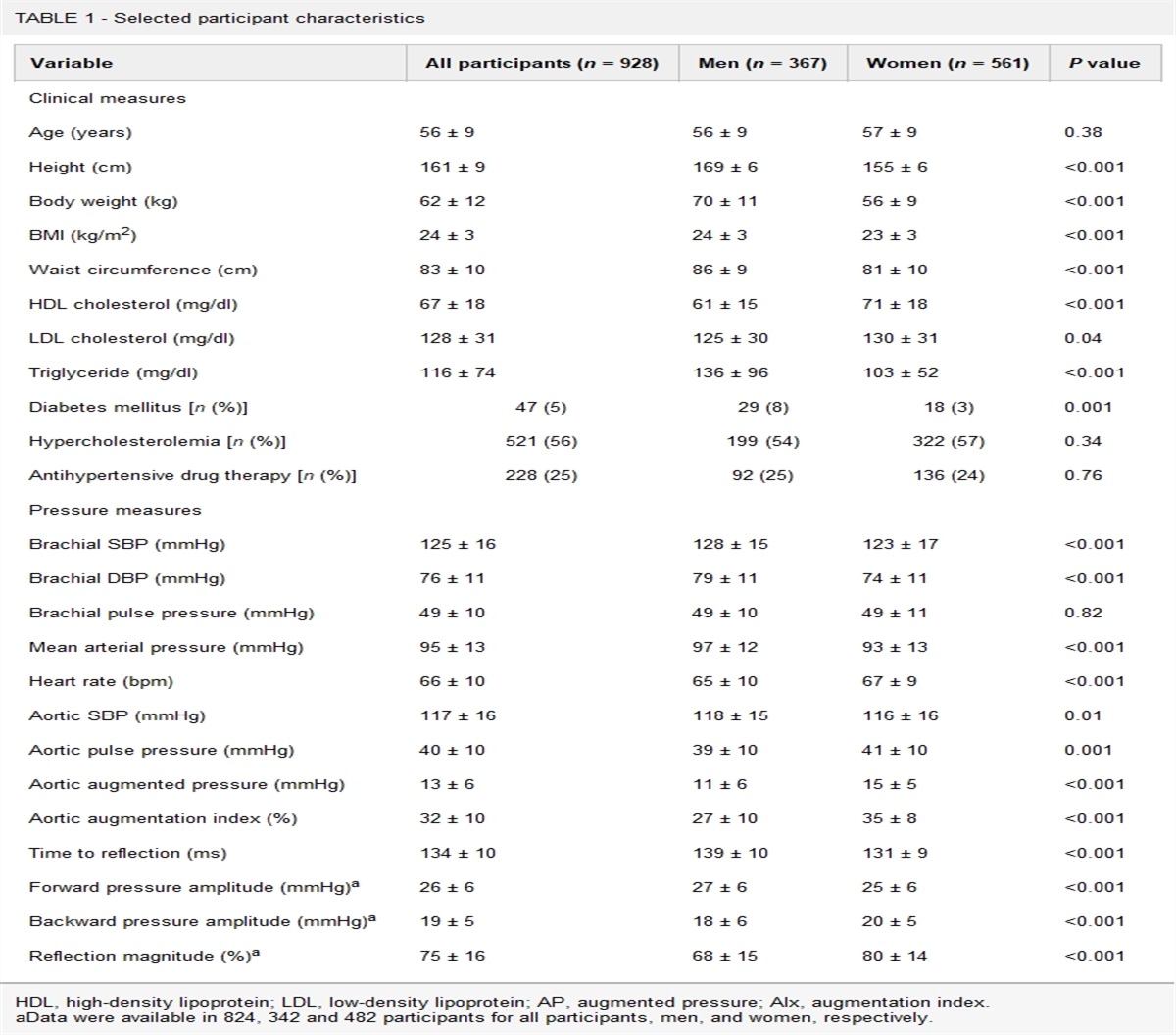
RESULTS Baseline characteristicsParticipant characteristics at baseline are summarized in Table 1 (n = 501). The cohort was predominantly female (61%), with mean (±SD) age 53.4 ± 8.0 years. Most individuals were of white ethnicity (80%). Mean clinic (seated) SBP and DBP were 124 ± 16 and 80 ± 10 mmHg, respectively. A small proportion of participants in the MARINA trial were on stable antihypertensive medication (4%). No individuals from CRESSIDA or Fruit & Veg were on antihypertensive therapy. Mean baseline PWV was 8.4 ± 1.6 m/s and mean baseline ambulatory SBP was 130 ± 13 mmHg during the day, 110 ± 14 mmHg at night and 125 ± 13 mmHg over 24 h. Mean baseline ambulatory DBP was 79 ± 8 mmHg for day, 65 ± 8 mmHg at night and 76 ± 7 mmHg over 24 h. Mean BMI at baseline was 26.0 ± 3.9 kg/m2. There was no significant change in mean BMI over the duration of the studies (P = 0.938).
TABLE 1 - Individual characteristics at baseline CRESSIDA (n = 159) Fruit & Veg (n = 48) MARINA (n = 294) All (n = 501) Age (years) 52.9 ± 8.0 45.2 ± 9.4 55.1 ± 6.6 53.4 ± 8.0 Female [n (%)] 96 (60) 25 (52) 184 (63) 305 (61) Ethnicity White [n (%)] 133 (84) 29 (60) 239 (81) 401 (80) Black [n (%)] 14 (9) 10 (21) 15 (5) 39 (8) Asian [n (%)] 10 (6) 9 (19) 27 (9) 46 (9) Other/mixed [n (%)] 2 (1) 0 13 (4) 15 (3) BMI (kg/m2) 26.0 ± 3.8 28.4 ± 3.8 25.5 ± 3.9 26.0 ± 3.9 Antihypertensive use [n (%)] 0 0 11 (4) 11 (2) PWV (m/s) 7.5 ± 1.2 7.9 ± 1.0 8.9 ± 1.7 8.4 ± 1.6 Clinic seated measurements: SBP (mmHg) 120 ± 16 129 ± 12 126 ± 16 124 ± 16 DBP (mmHg) 79 ± 10 87 ± 8 80 ± 10 80 ± 10 HR (bpm) 66 ± 9 73 ± 9 68 ± 9 68 ± 9 Ambulatory measurements: SBPday (mmHg) 126 ± 13 139 ± 14 131 ± 13 130 ± 13 SBPnight (mmHg) 107 ± 14 116 ± 14 110 ± 13 110 ± 14 24-h SBP (mmHg) 122 ± 12 135 ± 13 126 ± 12 125 ± 13 DBPday (mmHg) 77 ± 8 88 ± 7 79 ± 7 79 ± 8 DBPnight (mmHg) 64 ± 9 71 ± 8 65 ± 7 65 ± 8 24-h DBP (mmHg) 74 ± 7 85 ± 7 76 ± 7 76 ± 7 HRday (bpm) 72 ± 9 76 ± 7 76 ± 8 75 ± 8 HRnight (bpm) 62 ± 9 65 ± 9 64 ± 8 63 ± 9 24-h HR (bpm) 70 ± 8 74 ± 7 73 ± 7 72 ± 8Values represent means ± standard deviation, or number [percentage].HR, heart rate; PWV, pulse wave velocity.
Baseline SBPday and SBPnight were significantly correlated with age (r = 0.15, P = 0.001 and r = 0.14, P = 0.001 respectively), but DBPday and DBPnight were not (r = 0.02, P = 0.70 and r = 0.85, P = 0.06). Baseline BMI was significantly correlated with all baseline pressure measurements (r = 0.26, P < 0.001 for SBPday, r = 0.29, P < 0.001 for SBPnight, r = 0.16, P < 0.001 for DBPday and r = 0.23, P < 0.001 for DBPnight).
Associations between blood pressure variability and mean pressuresSignificant associations were observed between mean ambulatory BP values and the variability of those measurements (Fig. 2). For SBP, both day and night measurements demonstrated a significant association between mean values and the SD of those measurements (SBPdayr = 0.21, P < 0.001; SBPnightr = 0.27, P < 0.001) (Fig. 2a and c). When the relationship was investigated using the ratio of variability and mean SBP (individual CoV), the strength of the relationship was no longer significant for day measurements (r = 0.03, P = 0.449) and reduced for night (r = 0.15, P = 0.001; Fig. 2b and d).
 FIGURE 2:
FIGURE 2: Associations between individual ambulatory mean pressures and SD or coefficient of variation. (a) Daytime systolic SD. (b) Daytime systolic CoV. (c) Night-time systolic SD. (d) Night-time systolic CoV. (e) Daytime diastolic SD. (f) Daytime diastolic CoV. (g) Night-time diastolic SD. (h) Night-time diastolic CoV. CoV, coefficient of variation; SD, standard deviation.
For ambulatory DBP measurements, a significant positive relationship was observed between mean values and the SD of those measurements (DBPdayr = 0.17, P < 0.001 and DBPnightr = 0.29, P < 0.001; Fig. 2e and g). Conducting the analyses with CoV removed the significant association for both DBPday and DBPnight (r = 0.02, P = 0.696 and r = 0.10, P = 0.496, respectively; Fig. 2f and h).
Within-individual coefficient of variation for repeated ambulatory blood pressure measurementsMeasures of within-individual CoV for each study and for the entire cohort are summarized in Table 2. Qualitative analysis shows that measures of CoV for each BP measurement are similar for each study. In the entire cohort, the CoV for daytime measurements is significantly lower than that compared with night-time measurements: 5.4% (95% CI 5.2–5.6) for SBPday compared with 7.0% (95% CI 6.7–7.3) for SBPnight, and 6.1% (95% CI 5.9–6.4) for DBPday compared with 8.4% (95% CI 8.0–8.7) for DBPnight. CoV is significantly lower for 24-h ABPM measurements: 4.8% (95% CI 4.6–5.0) for SBP, and 5.3% (95% CI 5.1–5.5) for DBP.
TABLE 2 - Measures of reproducibility in ambulatory blood pressure and pulse wave velocity CRESSIDA Fruit & Veg MARINA ALL n CoV, % (95% CI) n CoV, % (95% CI) n CoV, % (95% CI) n CoV, % (95% CI) All individuals 159 48 294 501 SBPday 5.0 (4.8–5.4) 5.4 (4.9–6.0) 5.6 (5.3–5.9) 5.4 (5.2–5.6) SBPnight 6.7 (6.3–7.0) 7.5 (6.7–8.4) 7.1 (6.7–7.5) 7.0 (6.7–7.3) 24-h SBP 4.7 (4.4–4.9) 4.9 (4.4–5.5) 4.8 (4.5–5.1) 4.8 (4.6–5.0) DBPday 5.1 (4.8–5.4) 6.3 (5.7–7.0) 6.6 (6.2–7.0) 6.1 (5.9–6.4) DBPnight 9.0 (8.5–9.5) 8.1 (7.2–8.9) 8.0 (7.5–8.5) 8.4 (8.0–8.7) 24-h DBP 4.8 (4.5–5.0) 5.7 (5.1–6.4) 5.5 (5.1–5.8) 5.3 (5.1–5.5) HRday 6.0 (5.7–6.4) 6.5 (5.8–7.2) 6.4 (6.0–6.8) 6.3 (6.1–6.5) HRnight 7.2 (6.8–7.7) 7.8 (7.0–8.7) 8.3 (7.8–8.8) 7.9 (7.6–8.2) 24-h HR 5.8 (5.5–6.1) 6.0 (5.3–6.6) 5.9 (5.6–6.3) 5.9 (5.7–6.1) PWV 7.6 (6.7–8.4) 10.4 (9.3–11.5) 12.1 (11.1–13.1) 10.7 (9.0–10.9) Normotensive individuals 121 17 186 324 SBPday 5.3 (4.9–5.6) 6.0 (5.0–7.0) 5.6 (5.2–6.0) 5.5 (5.2–5.8) SBPnight 6.7 (6.2–7.1) 7.2 (5.9–8.5) 7.0 (6.5–7.5) 6.9 (6.6–7.2) 24-h SBP 4.8 (4.5–5.1) 4.8 (3.9–5.6) 4.7 (4.3–5.1) 4.7 (4.5–5.0) DBPday 5.3 (5.0–5.7) 7.7 (6.4–9.1) 6.4 (5.9–6.8) 6.1 (5.8–6.4) DBPnight 9.2 (8.6–9.8) 7.7 (6.3–9.1) 8.3 (7.7–8.9) 8.6 (8.2–9.0) 24-h DBP 5.0 (4.6–5.3) 6.5 (5.3–7.6) 5.3 (4.9–5.7) 5.3 (5.0–5.5) HRday 6.1 (5.7–6.5) 6.5 (5.4–7.6) 6.3 (5.9–6.8) 6.3 (6.0–6.6) HRnight 7.4 (6.9–7.8) 7.0 (5.7–8.3) 8.7 (8.0–9.4) 8.1 (7.7–8.5) 24-h HR 6.0 (5.6–6.3) 5.4 (4.4–6.4) 5.8 (5.4–6.3) 5.9 (5.6–6.1) PWV 7.1 (6.2–8.0) 11.0 (9.1–13.0) 11.7 (10.5–13.0) 10.2 (9.4–10.9) Hypertensive individuals 38 31 108 177 SBPday 4.4 (3.9–4.9) 5.1 (4.4–5.7) 5.6 (5.1–6.2) 5.3 (4.9–5.6) SBPnight 6.6 (5.8–7.4) 7.8 (6.7–8.8) 7.3 (6.5–8.0) 7.2 (6.7–7.7) 24-h SBP 4.1 (3.6–4.6) 5.0 (4.4–5.7) 5.1 (4.6–5.6) 4.9 (4.5–5.2) DBPday 4.4 (3.9–4.9) 5.5 (4.8–6.2) 6.9 (6.2–7.6) 6.2 (5.8–6.6) DBPnight 8.2 (7.3–9.2) 8.3 (7.2–9.4) 7.6 (6.8–8.3) 7.8 (7.3–8.4) 24-h DBP 4.1 (3.6–4.6) 5.3 (4.6–6.0) 5.6 (5.1–6.2) 5.3 (4.9–5.6) HRday 5.6 (5.0–6.3) 6.5 (5.7–7.3) 6.6 (5.9–7.2) 6.4 (6.0–6.8) HRnight 6.9 (6.1–7.7) 8.3 (7.2–9.3) 7.6 (6.8–8.4) 7.6 (7.1–8.1) 24-h HR 5.3 (4.7–5.9) 6.2 (5.4–7.1) 6.1 (5.5–6.7) 5.9 (5.6–6.3) PWV 9.0 (6.9–11.1) 10.0 (8.7–11.4) 12.7 (10.9–14.5) 11.5 (10.5–12.6)Normotension defined as baseline ambulatory SBPday <135 mmHg. Hypertension defined as baseline ambulatory SBPday ≥135 mmHg.CI, confidence interval; CoV, within-individual coefficient of variation; HR, heart rate; PWV, pulse wave velocity.
Reproducibility of ambulatory measurements was compared between individuals defined as normotensive on their baseline visit compared with those defined as hypertensive (Table 2 and Fig. 3). The mean baseline SBP for the normotensive group was 122 ± 8 mmHg compared with 144 ± 9 mmHg for the hypertensive group. When considering all normotensives versus all hypertensive individuals, there was no clear evidence of any difference in the reproducibility of SBPday, SBPnight, DBPday or DBPnight. However, both the CRESSIDA and Fruit & Veg studies showed significantly less variability in hypertensive individuals than normotensive individuals for measurements of DBPday: 4.4% (95% CI 3.9–4.9) in hypertensive individuals compared with 5.3% (95% CI 5.0–5.7) in normotensive individuals in CRESSIDA, and 5.5% (95% CI 4.8–6.2) in hypertensive individuals compared with 7.7% (95% CI 6.4–9.1) in normotensive individuals in Fruit & Veg.
 FIGURE 3:
FIGURE 3: Comparison of within-individual coefficient of variation between individuals defined as normotensive at study baseline (SBP <135 mmHg) versus individuals defined as hypertensive at study baseline (SBPday ≥135 mmHg). Error bars represent 95% confidence intervals. CoV, within-individual coefficient of variation; PWV, pulse wave velocity.
Association of individual risk factors to individual blood pressure variabilityAverage estimates of individual BPV, as assessed by the SD, were as follows: SBPday SD 6.1 ± 3.3 mmHg, SBPnight SD 6.6 ± 3.8 mmHg, DBPday SD 4.1 ± 2.3 mmHg and DBPnight SD 4.4 ± 2.5 mmHg. BPV was not correlated with age for SBPday SD, SBPnight SD, DBPday SD, DBPnight SD (all P > 0.05). BMI at baseline was significantly correlated with SBPday SD (r = 0.09, P = 0.04), SBPnight SD (r = 0.20, P < 0.001) and DBPnight SD (r = 0.19, P < 0.001), and had a borderline significant correlation with DBPday SD (r = 0.09, P = 0.054).
Table 3 summarizes multivariable linear regression investigating the associations between BPV to individual demographics and mean BP. No significant associations were demonstrated for age, sex or PWV with SD for SBPday, SBPnight, DBPday or DBPnight. SBPday SD was independently associated with nonwhite ethnicity, use of antihypertensive medication and mean SBPday. SBPnight SD was independently associated with baseline BMI and mean SBPnight. DBPday SD was only associated with mean DBPday. DBPnight SD was independently associated with baseline BMI and mean DBPnight. Further analyses were performed examining the effect of mean sleep duration on night-time variability, in a subset of 207 individuals in whom these data were available (the CRESSIDA and Fruit & Veg participants). Mean sleep duration was not independently associated with SBPnight SD (P = 0.482) or DBPnight SD (P = 0.160), as shown in Supplemental Digital Content, Table S3, https://links.lww.com/HJH/C73, which details the full linear regression models.
TABLE 3 - Multivariable linear regression showing associations between variability of ambulatory blood pressures to mean blood pressure and demographic risk factors
留言 (0)