
記住我

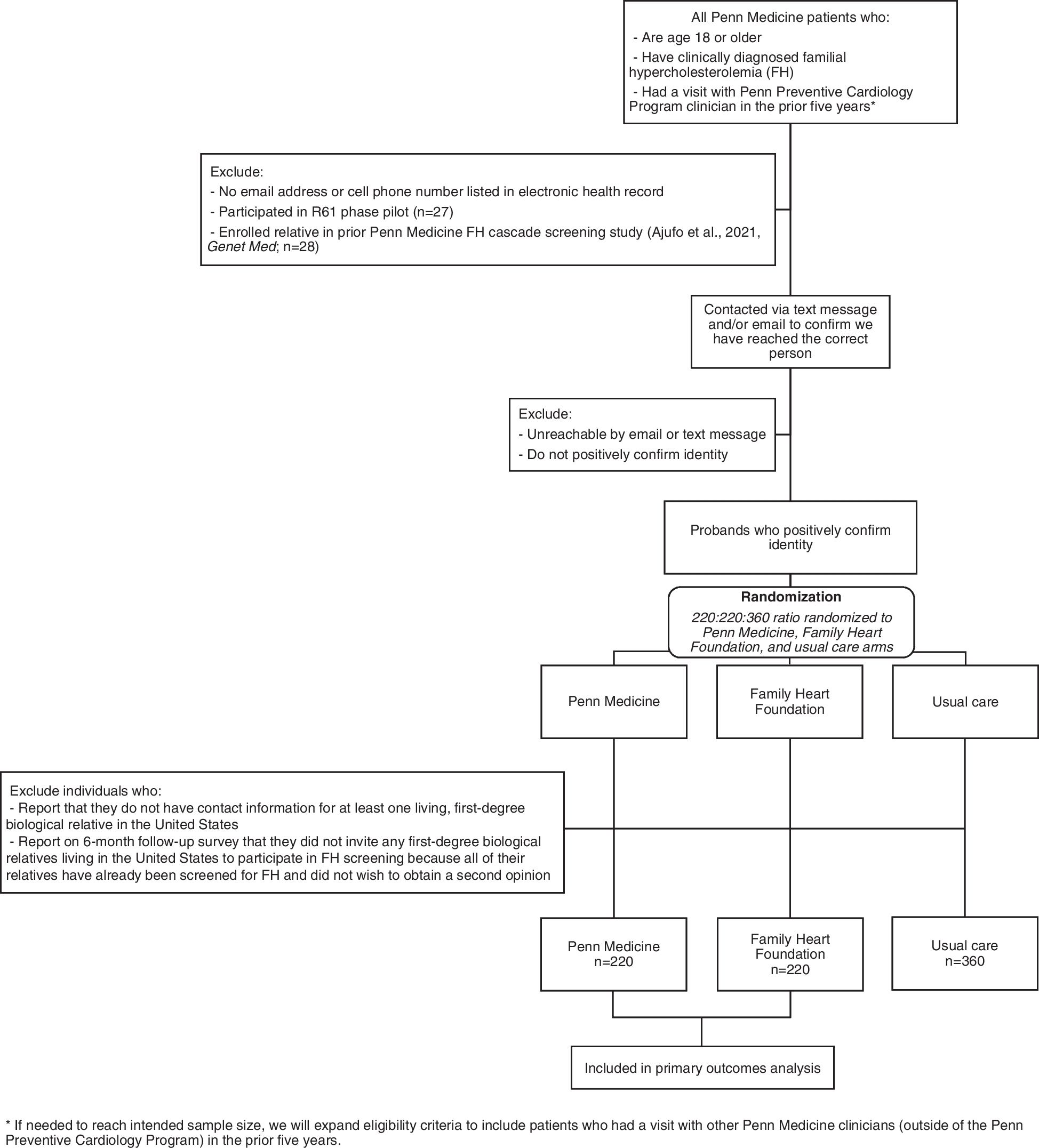




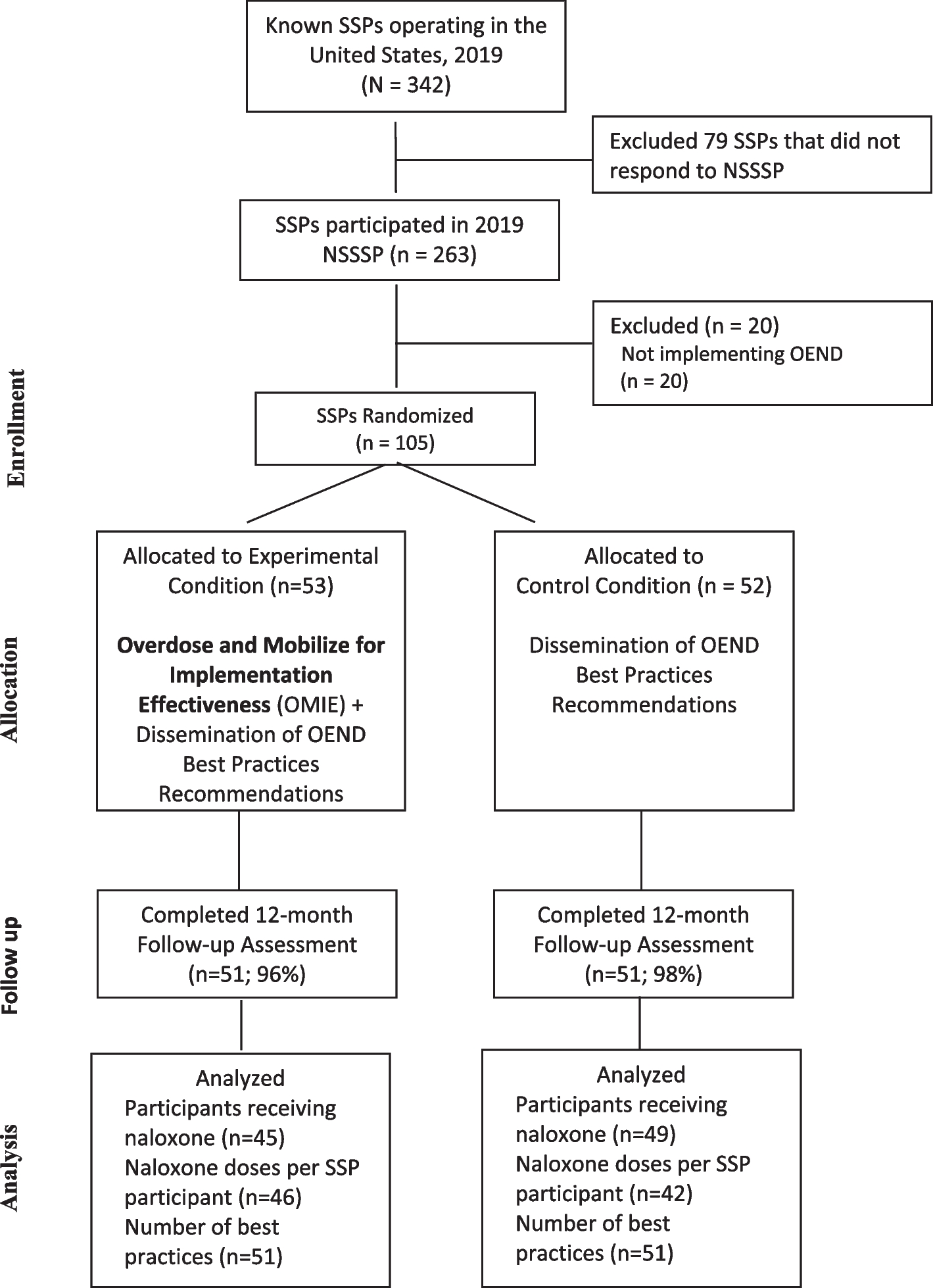
After deduplication of identified records, we screened 17,240 titles and abstracts, the majority of which were excluded (n = 17,185). The yield rate is slightly lower than previous estimates likely due to the breadth of stakeholders, summary formats, and outcomes of interest [38, 39]. We reviewed 54 full-text articles and identified 22 articles for inclusion which all underwent backwards citation screening (Fig. 3). The search strategy output and reasons for inclusion/exclusion files are available on OSF [19]. Of note, many studies had multiple phases or participant groups. We included the study if we could clearly separate the methods and results for the phase and/or group. Where possible, we extracted information only from the eligible phase/group.
Fig. 3 Characteristics of included studies
Characteristics of included studiesOur final sample included 22 full-text articles representing 20 unique studies. This included 16 qualitative studies, 4 RCTs, and 1 mixed-methods RCT and qualitative study (Tables 1 and 2) involving 908 total participants from a variety of different stakeholder groups (Table 1). Many studies involved a multidisciplinary mix of participants such as researchers, health professionals, and policymakers [40, 41, 43,44,45, 47,48,49,50, 54,55,56, 59,60,61], although some had homogenous groups of clinicians [51, 52, 57] or decision-makers [42, 46, 53]. The majority of types of evidence syntheses were systematic reviews, but one study related specifically to network meta-analyses (NMA), one to diagnostic test accuracy (DTA) reviews, and one to updating reviews. Seven studies involved an international mix of participants [42, 48, 53, 54, 58, 60, 61], five were from Canada [43, 46, 47, 51, 52], three from the USA [44, 45, 49, 55, 56], two from Croatia [41, 59], two from England [40, 57], and one from Kenya [50]. Most were funded by national agencies [41,42,43, 45,46,47, 49, 51, 52, 55, 56, 59] such as the Canadian Institutes of Health Research [43, 47, 51, 52] or the Agency for Healthcare Research and Quality [45, 46, 49, 55, 56].
Table 1 Included qualitative studiesTable 2 Included randomised controlled trialsThe TiDiER checklist was used to gather intervention data detailed in Tables 1, 2, and 3. The majority of included qualitative studies conducted either focus groups [41, 43, 49, 51, 52] or one-on-one semi-structured interviews [40, 42, 44,45,46,47, 50, 53,54,55,56,57,58, 62] (Table 1). RCTs were conducted either with an online survey [59, 60] or through in-person workshops (Tables 2 and 3) [50, 61]. There were a wide variety of summary formats tested including de novo summary prototypes [43, 46, 47, 49,50,51,52,53, 57], Grading of Recommendations, Assessment, Development and Evaluations (GRADE) Summary of Findings (SoF) evidence tables [42, 48, 50, 54, 58], MAGICapp [55, 56], Tableau [55,
留言 (0)