
記住我
Obesity is an important risk factor for severe COVID-19 and, possibly, for breakthrough SARS-CoV-2 infections in fully vaccinated people. Novel findings highlight how SARS-CoV-2 infects adipose tissue and promotes subclinical inflammation. Thus, also based on knowledge about endocrine dysfunction facilitating SARS-CoV-2 infection, a vicious cycle involving obesity, impaired metabolic health and COVID-19 might exist.
Refers to Martínez-Colón, G. J. et al. SARS-CoV-2 infection drives an inflammatory response in human adipose tissue through infection of adipocytes and macrophages. Sci Transl Med. https://doi.org/10.1126/scitranslmed.abm9151 (2022).
The cardiometabolic diseases obesity, type 2 diabetes mellitus (T2DM) and cardiovascular disease are associated with severe COVID-19 and, in most studies, these relationships have been found to be independent of each other1. However, analyses from the large COVID-19 Host Genetics Initiative, which applied a Mendelian randomization approach, indicated that only increased body-mass index (an estimate of increased adipose tissue mass) is causally involved in the pathogenesis of COVID-19 (ref.2). Owing to the limitations of Mendelian randomization analyses, the involvement of the other cardiometabolic diseases in the pathogenesis of COVID-19 cannot be excluded. These data highlight the great importance of increased adipose tissue mass for severe COVID-19.
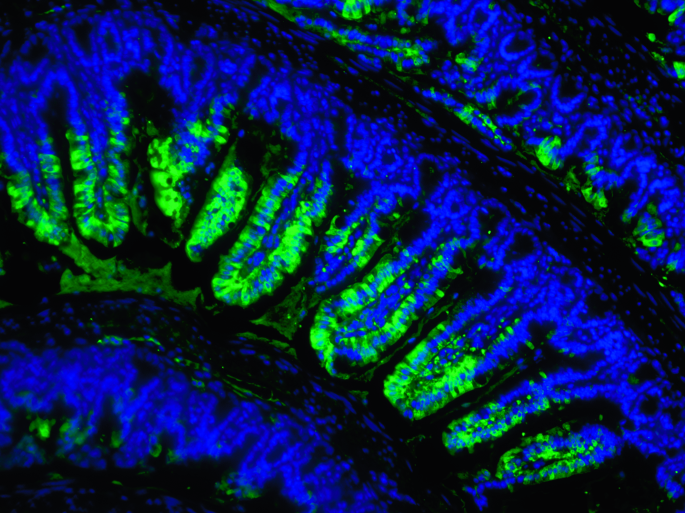
To understand the mechanisms involved in this relationship, Martínez-Colón and colleagues investigated the targets of SARS-CoV-2 within adipose tissue. Furthermore, they studied how infection might drive subclinical inflammation and functional alterations at the single-cell level3 by analysing adipose tissue from patients with COVID-19 who had died. They detected SARS-CoV-2 RNA in several adipose depots and, by using RNA in situ hybridization, they also found SARS-CoV-2 in the cytoplasm of adipocytes and an adjacent mononuclear inflammatory infiltrate. Using mature adipocytes and preadipocytes isolated from adipose tissue of patients who underwent bariatric or cardiothoracic surgery, Martínez-Colón and colleagues showed that adipocytes are permissive of SARS-CoV-2 infection.
When investigating the role of ACE2 (the entry receptor for SARS-CoV-2), unexpectedly, ACE2 seemed not to be necessary for SARS-CoV-2 infection of adipocytes. Furthermore, the authors showed that adipose tissue macrophages are abortively infected by SARS-CoV-2 and that SARS-CoV-2 infection of stromal vascular cells derived from adipose tissue promotes inflammation. Interestingly, the authors found evidence that SARS-CoV-2 entry into macrophages might also not be dependent on ACE2 expression. Altogether, the new data by Martínez-Colón and colleagues suggest that adipose tissue could serve as an important target and reservoir for SARS-CoV-2 and that the related local inflammation and possible systemic inflammation might promote severe COVID-19 in people with obesity3.
A role of adipose tissue in mediating severe outcomes of SARS-CoV-2 infection has also been proposed by other researchers. For example, a 2021 study found viral RNA in the adipose tissue of SARS-CoV-2-infected Syrian hamsters, together with reduced secretion of the anti-inflammatory and cardiometabolically protective hormone adiponectin compared with non-infected animals4. In addition, this study found that SARS-CoV-2 could directly infect human and mouse adipocytes. On the basis of these data and their findings that insulin resistance is the main cause for hyperglycaemia in patients with severe COVID-19, the authors concluded that SARS-CoV-2 might induce adipose tissue dysfunction, resulting in insulin resistance and adverse outcomes in acute COVID-19 (ref.4). In support of this conclusion, a 2022 study found that SARS-CoV-2 could infect adipocytes but not preadipocytes5. Importantly, this infection was particularly pronounced in lipid-laden cells and the authors found SARS-CoV-2 RNA in adipose tissue of people with active SARS-CoV-2 infection and COVID-19 who had obesity and overweight, but not those who were lean. Furthermore, the authors found that ACE2 expression was strongly induced upon adipocyte differentiation, and that inhibition of lipolysis in adipocytes strongly reduced viral replication. These data suggest that SARS-CoV-2 infection of adipocytes is dependent on a sufficient availability of lipids within the cells5.
“a vicious cycle involving obesity, impaired metabolic health and COVID-19 might exist”
Besides local conditions in adipose tissue, SARS-CoV-2 infection of adipose tissue might also depend on the humoral milieu. In this respect, a 2021 study found evidence suggesting that insulin-resistant hyperinsulinaemia could be involved in the infection of adipose tissue by SARS-CoV-2 (ref.6). In experiments with HEK293T cells, the authors showed that the SARS-CoV-2 spike protein physically interacts with cell-surface glucose-regulated protein 78 (GRP78), which was proposed to increase SARS-CoV-2 infectivity. In addition, they not only found GRP78 to be highly expressed in adipose tissue during ageing, obesity and T2DM, but also that hyperinsulinaemia upregulates this GRP78 expression6.
What, therefore, is the big picture about adiposity and severe COVID-19? There is ample evidence that adipose tissue is an important target for SARS-CoV-2 (refs.3,4,5,6). Interestingly, it might not be adipose tissue per se, but rather specifically lipid-laden adipocytes that enable the virus to infect adipose tissue and to replicate5. In addition, in humans, higher levels of ACE2 expression were observed in visceral adipose tissue as compared with subcutaneous adipose tissue, and ACE2 expression was found to increase with age7. Furthermore, insulin-resistant hyperinsulinaemia could be an important factor in enabling SARS-CoV-2 to infect adipose tissue6. In addition, hyperglycaemia might promote this process. In this respect, increased levels of glucose were found to facilitate viral replication and cytokine production in monocytes, and glycolysis was found to sustain SARS-CoV-2-induced monocyte response and viral replication8. Such dysregulated metabolic conditions characterized by hyperglycaemia, hyperinsulinaemia and subclinical inflammation are commonly observed in people with visceral obesity and reduced gluteofemoral adipose tissue mass, and particularly in people with non-alcoholic fatty liver disease9. SARS-CoV-2 is thought to infect hepatocytes, resulting in hepatic dysfunction. Furthermore, the steatotic liver, if infected by the virus, could contribute to hyperglycaemia and hyperinsulinaemia and could also contribute to organ dysfunction in COVID-19 via dysregulated production of lipids, cytokines and hepatokines9. These processes — involving inflammation and dysfunction of adipose tissue, liver, pancreas and other organs — might not only affect acute COVID-19, but also breakthrough SARS-CoV-2 infections in fully vaccinated people. This hypothesis is supported by an increased risk of immunosenescence in patients with obesity and/or T2DM, and indications of reduced SARS-CoV-2 vaccine effectiveness in patients with overweight and diabetes mellitus as compared with people without overweight and/or diabetes mellitus10.
“there is ample evidence that adipose tissue is an important target for SARS-CoV-2”
In conclusion, there is accumulating data that SARS-CoV-2 infection of adipose tissue could increase the risk of severe COVID-19 by replication of the virus within adipocytes and induction of local and systemic inflammation. Thereby, a vicious cycle (Fig. 1) might be put in motion that involves obesity, impaired metabolic health and severe COVID-19.
Fig. 1: Vicious cycle involving SARS-CoV-2 infection of adipose tissue.
SARS-CoV-2 infection of adipocytes and macrophages promotes virus replication and local and systemic inflammation. Adipose tissue inflammation contributes to systemic hyperglycaemia and hyperinsulinaemia, both of which facilitate SARS-CoV-2 infection.
留言 (0)