
記住我








A single-center cross-sectional cohort study was conducted between February 2018 and April 2019. The authors selected an idiopathic Normal Pressure Hydrocephalus (iNPH) population for this study, such as a homogeneous consecutive cohort without intracranial hypertension. Participants had to be I) older than 18 years and II) with suspected iNPH diagnosis after a multidisciplinary evaluation (PRO-Hydro) based on clinical and radiological findings [16]. Patients with ON diseases, the presence of a central nervous system mass, other primary causes of possible altered ICP and those who declined participation in the present study, were excluded. Eligible patients underwent a specific 3-Tesla brain MRI, using a protocol described below, and an immediate subsequent ONSD sonographic assessment. The study was conducted in accordance with the declaration of Helsinki and the principles of Good Clinical Practice. The study protocol was approved by the local ethics committee (Cod. CE 17115). All patients gave their written informed consent to participate. We used Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies as reporting guidelines [17].
BiasThe same MRI and US equipment were used to limit a systematic error in ONSD measurements, and the two measurements were obtained in rapid sequence to minimize ICP orthostatic changes. Same neuroradiologist and neurosonologists performed all measurements. Patients with iNPH require a complex process of differential diagnosis, therefore the population that can be recruited for the duration of the study, albeit in a reference center, is small.
Demographic and clinical variablesThe age and gender of patients were recorded for each enrollment. iNPH was suspected according to criteria established by Relkin et al. [18].
MRI variablesA 3-Tesla whole-body scanner MRI (Magnetom Skyra, Siemens Healthcare, Erlangen, Germany) used a 32-channel phased-array head coil. The neuroradiologist selected the best sequence available within the specific protocol, using a sagittal T1-weighted rapid three-dimensional gradient echo technique (Repetition Time, 2300 ms; Echo Time, 2.98 ms; flip angle, 9°; thickness, 1 mm; 160 slices; field of view, 256 × 248 mm; matrix, 256 × 248: 1 mm × 1 mm) which showed contrasts between endo-orbital fat and sheath providing optimal morphological imaging for ONSD evaluation. The measurements were performed on reconstructions carried out parallel and orthogonal to the ON. The assessments were performed twice, blindly, on the same images, at 2 weeks from each other.
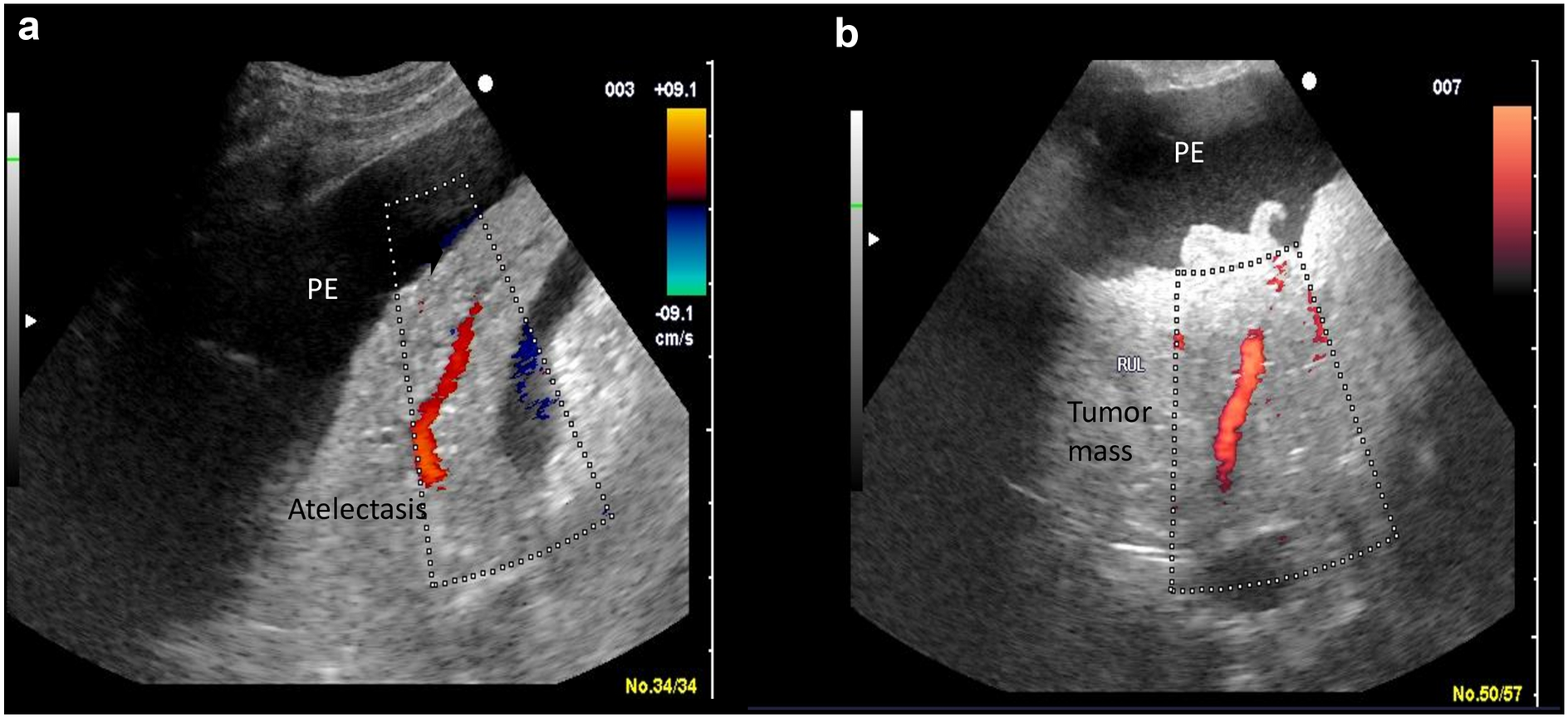
Ultrasound variablesUS settings and ONSD evaluation were performed according to the CLOSED protocol, a bundle which includes safety measures and technical procedures already reported in a previous paper [13]. US was performed disjunctively in B-mode and color-Doppler mode, using a MyLab™Twice US system (Esaote, Italy) equipped with a 11–3 MHz linear transducer (Fig. 1).
Fig.1
Three ultrasound images of the eyeball and optic nerve with sheath, enriched by the parameters/landmarks highlighted in CLOSED protocol. a B-mode image in gray-scale: dashed white arrow points to the optic disc, in yellow window 4.3 mm ONSD measurement, in red window acoustic power output = 20%; b same image but with color-mode: white arrow points to the lens, in yellow window 3.9 mm ONSD measurement, in red window PRF 940 Hz (almost 1 Kh), yellow arrow points to central retinal artery; c same image but with color-mode plus Doppler wave (at the bottom): in red window Gain 50%, yellow arrow points to ophthalmic artery, in the enlarged panel the typical nock of the ophthalmic artery flow
Data variablesONSD was measured 3 mm behind the optic disc on MRI and US imaging. All measurements were performed bilaterally and on the two planes (transverse and sagittal), named right and left transverse diameter (TDR and TDL, respectively) and right and left sagittal diameter (SDR and SDL, respectively). All the investigators were blinded to the other measurements. One experienced neuroradiologist (FT) performed ONSD measurements two times on MRI, to determine the intra-agreement. Sonographic ONSD assessments were performed by one expert neurosonologist (RA) supported by a further expert physician proficient in neurosonology (GB).
Statistical analysisDemographical variables were compared between US subgroups (US B-mode group vs. US color-Doppler mode group): Mann–Whitney U test and Chi-square test were used to compare age and sex, respectively.
The evaluation of intra-reliability of ONSD assessment using MRI was performed calculating Bland–Altman plots [19]: the agreement between the two-consecutive assessment of the same neuroradiologist (intra-observer) were quantified by plotting the difference between measurements against their mean and by constructing limits of agreement. Mean and the standard deviations of the differences between two measurements were used for statistical limits; they represent the maximum deviation expected for the 95% of the differences between the two measurements. In addition, the Lin’s Concordance Correlation Coefficient (CCC) [20] with 95% confidence intervals (CI) was computed to quantify the strength of intra-observer agreement: this coefficient provided indications on a standardized relationship scale about precision (how close the data are about the line of best fit) and accuracy (how far the line of best fit is from the 45-degree line through the origin, which represents perfect agreement). Lin’s CCC values < 0.20 were considered as “poor” while values > 0.80 were considered as “excellent”, values between > 0.20 and < 0.80 were considered “moderate”.
The two different US methods (B-mode group and color-Doppler mode) were described using median and interquartile (IQR) range; differences in distribution were graphically displayed by box-plot and compared using Mann–Whitney U test. Then, differences between each of the two US methods and MRI were described by box-plot and evaluated by calculating average differences and their standard deviations.
Statistical analysis was performed using Stata statistical software version 14 (Stata Corp LLC, College Station, 101 TX, USA).
留言 (0)