
記住我




Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system (CNS). While the majority of people with MS (pwMS) initially present with a relapsing course (RMS), most experience disease progression which can include permanent mobility impairment, cognitive symptoms, and decreased social functioning [1,2,3], resulting in negative personal and professional repercussions.
There has been a dramatic increase in available disease-modifying treatments (DMTs) for relapsing, secondary-progressive and primary-progressive forms of MS in the past decade [4]. Despite these breakthroughs in treatment, there are still several unmet clinical needs with existing therapies, including a lack of an effect on relapse-independent disease biology, as evidenced by gradual relapse-independent disease worsening, even in people with early RMS on highly effective therapies [5].
Current DMTs limit disease progression primarily by dampening immune cell activity in the peripheral blood or hindering the migration of activated immune cells from the periphery into the CNS [6]. While early initiation of DMT has shown to improve the mid- and long-term prognosis of pwMS [7,8,9,10], many pwMS who receive these medications still develop significant disability worsening over time [5, 11, 12].
One of the leading hypotheses for the inability of most current DMTs to meaningfully prevent disease worsening in MS is their limited capacity to cross the blood–brain barrier (BBB) and to reach and exert a meaningful effect on the cells that orchestrate inflammation in the CNS compartment. Thus, more effective means to prevent disability progression have become the focus of recent clinical trials using small molecules that can act in the peripheral blood, cross the BBB, and directly modulate the activity of immune cells in the CNS. Inhibitors of Bruton’s tyrosine kinase (BTKI), a cytoplasmic tyrosine kinase that is expressed widely by a variety of hematopoietic cells, but predominately by B cells and myeloid cells, including microglia [13,14,15] are currently being investigated widely in MS. BTKIs have been evaluated as therapeutic agents in a number of diseases, including hematological malignancies, where they have proven to be an effective treatment strategy with relatively few toxic effects [16]. Recently, phase II clinical trials of BTKIs in systemic autoimmune diseases, such as rheumatoid arthritis (RA) [17], systemic lupus erythematosus (SLE) [18], and chronic spontaneous urticaria (CSU), have provided evidence of target engagement and clinical efficacy, and have also demonstrated decreases in inflammatory blood biomarkers, supporting their efficacy. In the context of MS, one of the major advantages of BTKIs over currently available DMTs is that these small molecules have the potential to cross the BBB and to exert beneficial effects on CNS-compartmentalized inflammation [19].
Bruton’s Tyrosine Kinase in MS PathophysiologyIt is well established that aberrantly activated immune cells cross from the peripheral blood into the CNS, where they contribute to the formation of inflammatory lesions [6, 20]. Genetic studies of MS implicate cells of the adaptive immune system, such as T and B cells, but also cells of the innate immune system, such as monocytes, dendritic cells, and natural killer cells [21] as relevant to the pathogenesis of MS. Pathological studies have provided evidence of immune cell activation and infiltration into the CNS, resulting in demyelination and neuronal degeneration [22, 23].
While T cells represent the prototypical pro-inflammatory cell type that drives inflammation in MS and its animal models [6, 20, 24], there is a wealth of accumulating evidence highlighting essential contributions from both B cells and myeloid cells. For example, aggregates of B cells and activated microglia have been described in the meninges of people with progressive forms of MS [25, 26] and have been associated with higher levels of disability [27, 28]. B cells from pwMS have been shown to produce pro-inflammatory cytokines [29, 30] and express high levels of the co-stimulatory molecules that are required for T-cell activation [31]. Therapy with monoclonal antibodies against anti-CD20 (rituximab and ocrelizumab), which is highly expressed on B cells, has a profound effect on reducing acute MS relapses and delays disease progression [32,33,34,35] in relapsing forms of MS, and is the first and currently only proven therapy for primary progressive MS. These effects are likely due to the removal of a relatively small fraction of highly differentiated B cells [36]. Since non-specific B cell depletion can result in lasting immune suppression and an increased risk of infections, there is a need for more targeted treatment approaches [37, 38]. The pivotal role that microglia play in mediating relapse-independent disease progression in chronic active lesions has been shown in numerous studies [39, 40]. Such chronic, active lesions can now be visualized when appropriate imaging techniques are utilized [41,42,43,44,45]. Imaging measures representing chronic active lesions, which include paramagnetic rim lesions (PRLs) and slowly evolving/expanding lesions (SELs) are being included as an exploratory imaging outcome measure in many of the phase II and III BTKi trials in MS [ 44,45,46,47,48]. Evobrutnib decreased SEL volume over 48 weeks in a dose-dependent manner in the Phase II clinical trial [49]. In the phase II tolebrutinib trial, the median total SEL volume was lowest in the 60 mg arm at 16 weeks, and in a subset of patients (n = 32) that had susceptibility-weighted imaging performed, 50% had PRLs at baseline, and the total number of PRLs remained stable in all but 2 patients: one patient who had a PRL at baseline had no subsequent susceptibility-weighted imaging, and another patient had one PRL identified on all but the last scan [50••]. At this time, it is unclear what specific PRL endpoint will be evaluated in phase III clinical trials. However, an open-label study evaluating tolebrutinib (NCT04742400) will be evaluating PRLs as the primary outcome measure and has explicitly stated that “modulation of PRLs, and changes in size of, and T1 relaxation time within, PRLs will be evaluated, which suggests that these methods and others may be used in the phase III clinical trials when evaluating PRLs. To participate in this trial, patients can have stable or progressive MS but need to have at least one PRL to be eligible for this trial. Reduction or resolution of the PRL would imply dampening the local immune cell response and would suggest repair. PRLs and SELs will be an exploratory endpoint of high interest in the on-going phase III BTKi clinical trials.
BTKIs have emerged as attractive agents that modulate B cell responses instead of causing broad and sustained B cell depletion [15, 51•]. BTK phosphorylation is a critical step in B cell activation, maturation, and differentiation [52]. BTK inhibition in B cells can limit their activation status and reduce their ability to serve as antigen-presenting cells to T cells, resulting in attenuation of pro-inflammatory T cell responses in vitro and in vivo, as recently demonstrated in a phase I study of BIO-0556375 [51•]. Moreover, BTKIs preferentially reduce memory B cells, which are thought to be highly pathogenic in MS [15, 51•]. Recent in vitro studies have shown that BTK activity is increased in B cells from pwMS and that the BTKI evobrutinib can suppress the development of CXCR3 positive memory B cells into antibody-secreting cells [53]. In addition, BTKIs reduced expression of integrins and chemokine receptors, such as integrin alpha4beta1 (VLA-4) or C-X-C chemokine receptor 4 (CXCR4) on B-cells, which may reduce their propensity to cross from the blood into the CNS [54].
While there is little evidence for direct effects of BTKIs on T cells [16, 51•], inhibition of BTK reduces signaling through the Toll-like receptor and inflammasome-related signaling pathways in a variety of additional cell types, including monocytes, macrophages, and dendritic cells in vitro and in animal models [55,56,57]. In vitro studies have shown that inhibition of BTK hinders the differentiation of monocytes into pro-inflammatory macrophages [58]. Microglia are the prototypical resident immune cells of the CNS and, upon activation, produce a variety of inflammatory mediators, including chemokines and other cytokines [59]. BTK inhibition has been shown to reduce pro-inflammatory cytokine levels in activated microglia in vitro and in animal studies [60]. In a pre-clinical in-vivo model, BTK levels have shown to be increased after demyelination, and its inhibition promotes myelin repair, likely via a mechanism that involves microglia [61].
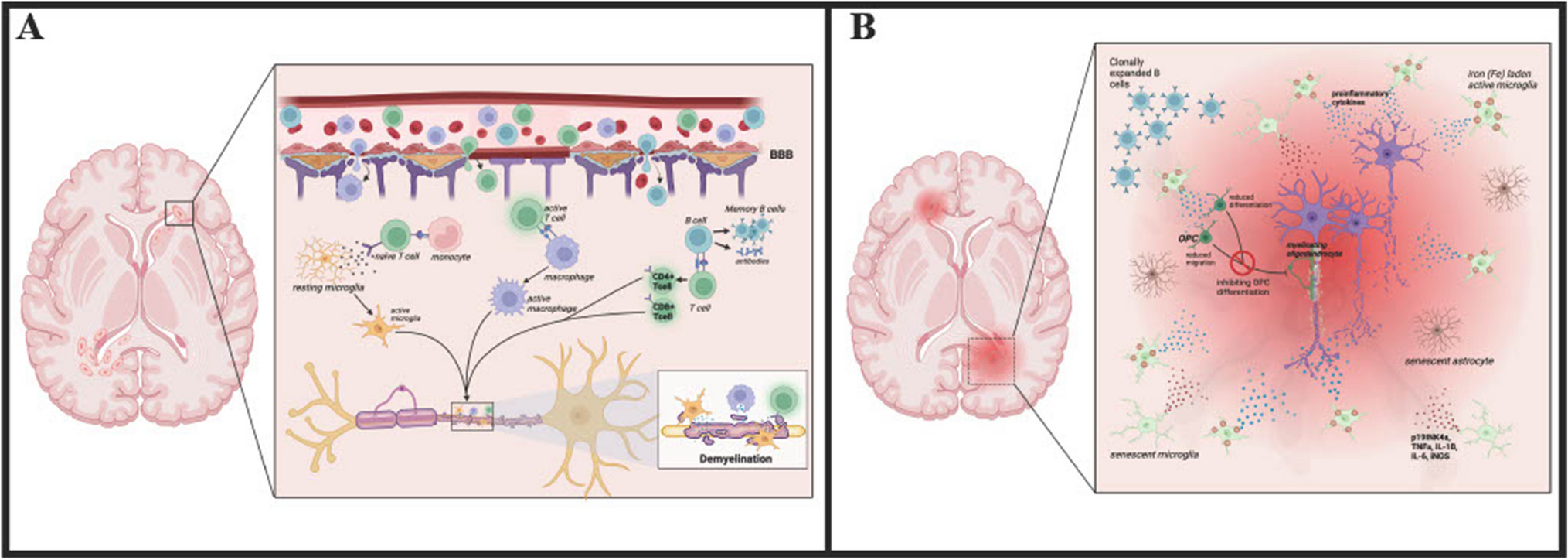
Studies in non-human primates, who were given oral tolebrutinib, fenebrutinib, or evobrutinib, showed that pharmacologically relevant doses of these BTKIs can be detected in cerebrospinal fluid (CSF) [19]. Since BTK-positive cells have been found to be increased in and around MS lesions [62], it is plausible that BTKIs will dampen both the peripheral and central immunopathology, which is a crucial driver of disability progression in MS. Thus, BTKIs carry great promise for the treatment of both relapsing and progressive forms of MS, where certain aspects of the pathology seem confined to the CNS compartment (Fig. 1).
Fig. 1
BTK inhibition can affect cells of the adaptive and innate immune system outside and within the CNS. Abbreviations: Bruton’s Tyrosine Kinase (BTK), B cell receptor (BCR), Fc-gamma receptor (FcyR), multiple sclerosis (MS). Created with BioRender.com
Clinical Trials in MS: EfficacyIn MS, a number of BTKIs are currently in clinical development and are being intensively studied in comprehensive clinical development programs. The BTKIs that are farthest along in clinical development for the treatment of MS are evobrutinib, tolebrutinib, fenebrutinib, remibrutinib, and orelabrutinib. Additional details of clinical trials that have completed or on-going of various BTKis in pwMS are summarized in Table 1.
Table 1 BTKIs being evaluated in phase II and phase III clinical trials in pwMS. Abbreviations: Relapsing MS (RMS), non-relapsing secondary progressive MS (NRSPMS), primary progressive MS (PPMS), annual relapse rate (ARR), Expanded Disability Status Scale (EDSS), not applicable (n/a), to be determined (tbd), gadolinium-enhancing (Gad +), adverse events (AEs), serious adverse events (SAEs), quaque die (QD), bis in die (BID). Information from clinicaltrials.govEvobrutinib is an oral, irreversible, selective BTKI that binds covalently to cysteine-481 through a warhead that increases selectivity over other kinases [63] with a half-life of approximately 2 h [64]. Evobrutinib demonstrated efficacy reaching its imaging endpoints in a randomized, placebo-controlled, double-blind phase II trial in RMS [63] Various doses of evobrutinib (25 mg daily, 75 mg daily, 75 mg twice daily) were evaluated against placebo as well as an open-label active control arm of dimethyl fumarate (DMF) [63] over 24 weeks. From weeks 24 to 48, there was a blinded extension where patients continued on the same dose that they were on up to week 24, with the exception of the placebo group that transitioned to evobrutnib 25 mg daily. The primary endpoint of reduction in gadolinium-enhancing (Gad +) lesions during weeks 12–24 was met by the evobrutinib 75 mg daily group vs placebo (p = 0.005) and there was a trend towards a reduction in the evobrutinib 75 mg twice daily group (p = 0.06). The mean total number of Gad + lesions was 3.85 ± 5.44 in the placebo group, 4.06 ± 8.02 in the evobrutinib 25-mg group, 1.69 ± 4.69 in the evobrutinib 75-mg once-daily group, 1.15 ± 3.70 in the evobrutinib 75-mg twice daily group, and 4.78 ± 22.05 in the DMF group. There was no significant effect seen on clinical outcomes, including annualized relapse rate (ARR) or disability progression, measured with the Expanded Disability Status Scale (EDSS). However, the study was relatively short and not powered to evaluate clinical endpoints. The unadjusted ARRs were numerically lower in the higher-dose evobrutinib subgroups: at week 24 was 0.37 in the placebo group, 0.57 in the evobrutinib 25-mg group, 0.13 in the evobrutinib 75-mg once-daily group, 0.08 in the evobrutinib 75-mg twice-daily group, and 0.20 in the DMF group.
Recently, the extension of this phase II clinical trial was reported up to 108 weeks [65]. Reassuringly, ARR remained low in patients treated with evobrutnib. Compared to those who initiated placebo or other doses of evobrutinib in the double-blind period followed by various doses of evobrutinib in the extension period: patients who initiated evobrutinib 75-mg twice-daily from the beginning of the study had lower ARR (0.11) at week 48 and at week 108 (0.12) and lower cumulative probability of a first relapse at week 48 (0.08) and at week 96 (0.20). In addition, serum neurofilament levels decreased in patients treated with evobrutinib 75 mg bid as early as 12 weeks and was sustained at week 24 [49]. Finally, the volume of slowly expanding lesions, which may represent chronic active lesions, was reduced over 48 weeks in a dose-dependent manner with evobrutinib, with the highest effect seen in those on 75 mg bid [49]. Two phase III trials evaluating evobrutinib in RMS vs teriflunomide as an active comparator are underway (NCT04338022 and NCT04338061), which will be informative for the field.
Tolebrutinib is an oral, irreversible, selective BTKI with evidence of high CNS penetrance in humans, which can be seen as early as 2 h after a single 120-mg dose [19] and covalently binds to cysteine-481 in the kinase domain and has a half-life of about 2 h [66]. Tolebrunitib was evaluated in a randomized, double-blind, placebo-controlled Phase IIb (NCT03996291) clinical trial where participants with RMS were randomized to four doses (5 mg, 15 mg, 30 mg, 60 mg) of tolebrutinib for 12 weeks in a cross-over study design with a 4-week placebo run-in and run-out period. This study design is noteworthy as it allowed for an efficient evaluation of 4 different doses of tolebrutnib over a relatively short time frame of 16 weeks. The primary endpoint was a reduction in new gadolinium-enhancing lesions.
After 12 weeks of treatment, tolebrutinib 60 mg resulted in an 85% relative reduction in new T1 Gad + lesions, and an 89% relative reduction in T2 lesions compared to what was observed during the placebo period. Patients who completed the phase IIb trial were eligible to enroll in the long-term extension study (LTS). Initially, in Part A of the LTS, patients continued on the same dose of tolebrutinib that they were on during the phase IIb core study. Thereafter, all patients were transitioned to tolebrutinib 60 mg daily in Part B of the LTS, when this dose was selected for the Phase III development program. Recently, 18-month follow-up results of the LTS were reported. The vast majority of patients who were eligible to participate in the LTS (n = 124 of n = 129 total) were still enrolled at 18 months. In patients who had been on at least 8 weeks of treatment with tolebrutinib 60 mg daily, the ARR remained low at 72 weeks at 0.17. and there was no meaningful change in the EDSS scores over this time period. Based on the favorable results of the phase IIb study, tolebrutinib is currently being evaluated in a comprehensive phase III clinical development program which includes four ongoing phase III trials to evaluate tolebrutinib in MS: RMS with teriflunomide as an active comparator (GEMINI I and II), as well as in non-active SPMS (HERCULES) vs. placebo and in PPMS vs. placebo (PERSEUS). The inclusion of non-active SPMS patients in HERCULES is of interest, as other contemporary studies evaluating progressive MS have not selected specifically for patients without overt inflammatory clinical disease activity.
Fenebrutinib is an oral, selective, reversible BTKI that has demonstrated efficacy in phase II clinical trials of patients with RA [17], SLE [18], and CSU [67]. Fenebrutinib forms hydrogen bonds with lysine-430, methionine-477, and aspartate-539 residues of the kinase domain [68] andhas a half-life of 4.2 to 9.9 h [69]. In RA, fenebrutinib demonstrated efficacy comparable to existing highly-effective disease-modifying anti-rheumatic drugs. Based on the pooled safety profile in other autoimmune disorders, three phase III trials have been launched in MS, including two trials in RMS with teriflunomide as an active comparator (FENhance/NCT04586023 and NCT04586010). Eligible participants (n = 736) will be randomized 1:1 to either fenebrutinib or teriflunomide. The primary outcome measure is the ARR over a minimum of 96 weeks. FENtrepid (NCT04544449) is currently the only phase III BTKI trial enrolling people with primary progressive MS (PPMS). Eligible participants (n = 946) will be randomized 1:1 to either daily oral fenebrutinib (or placebo) or intravenous (IV) ocrelizumab (or placebo). The primary outcome is the time to onset of composite 12-week confirmed disability progression.
Remibrutinib is an oral, selective, reversible BTKI that covalently binds to cysteine-481 [70] and has a half-life of approximately 1 to 2 h [71]. There are two identical ongoing phase III clinical trials in RMS with teriflunomide as an active comparator (NCT05147220 and NCT05156281 [72]). Eligible participants (n = 800) are randomized 1:1. The primary outcome measure is the ARR. The extension is an open-label, single-treatment arm study in which eligible participants receive remibrutinib for up to 5 years.
Orelabrutinib is another oral selective, irreversible BTKI that binds covalently to cysteine-481 [73] and has a half-life of about 4 h [74]. Orelabrutinib is currently being tested in RMS in a phase 2 study (NCT04711148). Eligible patients (n = 160) with RMS will be randomly assigned to 1 of 4 treatment groups: placebo, orelabrutinib (low dose), orelabrutinib (medium dose), and orelabrutinib (high dose) at a 1:1:1:1 ratio. The primary outcome measure is the cumulative number of new Gad + T1 MRI brain lesions. The extension is an open-label, single-treatment arm study for patients who have completed week 24. All patients will receive the low dose of orelabrutinib or any other dose as suggested by the core study.
Clinical Trials: SafetyThe main safety concerns with currently available DMTs for MS are related to prolonged depletion of lymphocyte populations [75], chronically low immunoglobulin levels [76], and complete or near-complete blockade of lymphocytes from entering the CNS [77], which have all been associated with increased infection risk. While first-generation BTKIs, such as ibrutinib, have shown to be associated with a number of serious AEs, including significant risk of infection [78], bleeding risk, and cardiovascular risk, the few cases of infections seen with BTKIs considered for the treatment of MS have been generally mild and transient [50••, 79••, 80]. This is thought to be due to different binding profiles and improved selectivity resulting in fewer “off-target” effects. For example, binding of ibrutinib to human epidermal growth factor receptor 2 (HER2) has been implicated in cardiotoxic AEs [78] and the inhibition kinases other than BTK has shown to decrease T cell activation and increase susceptibility to infections [81].
The available safety data for BTKIs currently being evaluated in MS are summarized in detail below.
In a phase II trial of evobrutinib in MS (NCT02975349 [79••]), where 213 out of 267 participants received the drug, the highest rate of adverse events (AEs) was observed in pwMS who had received the highest dose of the drug (75-mg twice daily). The most commonly observed AEs were nasopharyngitis and increases in levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lipase. Rare but serious AEs included pneumonia, lung neoplasm, and peripheral embolism, spontaneous abortion, and seizure [79••]. Data from 861 patients that had received evobrutinib in phase II clinical trials were pooled, including patients with RA (NCT03233230), SLE (NCT02975336), and MS (NCT02975349) [82]. The proportion of patients with AEs was similar for those who had received evobrutinib and those who had received placebo. AEs that occurred in > 5% of patients on evobrutinib were urinary tract infections (9.5%), nasopharyngitis (7.3%), and diarrhea (6.2%). Elevations in ALT and AST were transient [82] and asymptoamatic, and there was no observable change in IgG levels of subtypes in evobrutinib-treated patients vs. placebo across studies Although the lack of change in immunoglobulin levels is reassuring, the majority of studies included in this analysis were of a relatively short duration (12–52 weeks); therefore, the long-term effect of evobrutinib on IgG and subtype levels will be of interest to follow in the long-term extension study, and phase III trials.
In a phase II trial of tolebrutinib in MS (NCT03889639 [50••]) where 130 participants received the drug, the most common AE was headache (9%), followed by upper respiratory tract infection (5%), and nasopharyngitis (4%). Three study participants had elevated ALT levels, including 2 who had concentrations of more than three times the upper limit of normal [50••]. One serious AE, hospitalization for MS relapse, was reported in a pwMS who had received the highest dose 60 mg [50••]. Eighteen-month long-term safety data analysis showed that the most common AEs were COVID-19 infections (16%), headache (13%), nasopharyngitis (10%), upper respiratory tract infections (8%), and arthralgia (6%) [80]. Reassuringly, all observed COVID-19 cases were mild or moderate, and all patients recovered and remained in the LTS. Reassuringly, there was no emergence of new safety signals, even for participants who had switched to the highest dose (60 mg) [80].
In late June 2022, phase III tolebrutinib trials were placed on partial hold by the US Food and Drug Administration (FDA) [83]. The decision was based on several cases of drug-induced hepatotoxicity. Most of the affected patients had comorbidities known to predispose them to drug-induced liver injury, and elevations of liver enzymes were reversible after drug discontinuation. Thus, enrollment criteria were adjusted to exclude people with known risk factors for hepatotoxicity. For those study participants who had completed at least 60 days in the trial without complications, the risk of liver injury was deemed minimal, and they were allowed to continue the study.
The safety of fenebrutinib was evaluated in a pooled analysis of safety data from 299 patients with autoimmune conditions (RA (NCT02983227), SLE (NCT02908100 and NCT03407482), or CSU (NCT03693625 and NCT03137069) [84]) that had received the highest dose of fenebrutinib (200 mg BID) in the context of phase II clinical trials. Common AEs were nasopharyngitis (6%), nausea (6%), and headache (5%). Elevations in ALT were transient, returning to normal after treatment cessation. There was no observed imbalance in rates of infection vs. placebo, and no signal of major bleeding risk or cardiovascular risk, as was observed with an older-generation BTKI, ibrutinib. Finally, although there was a slight numeric decrease in immunoglobulin levels (IgG and IgM) over time, the change was minimal and remained above the lower limit of normal in the vast majority of cases. In addition, a decrease in IgG or IgM levels was not associated with infection risk. However, it is important to keep in mind that the follow-up time period in this pooled safety analysis was quite variable; therefore, monitoring immunoglobulin levels and their association with infectious risk over many years will be of importance in BTKIs being evaluated in MS. Safety data on remibrutinib and orelabrutinib in MS and other autoimmune diseases remain sparse and is anticipated to be reported in the context of ongoing clinical trials (NCT05147220, NCT05156281, NCT04711148).
At the current time, it is difficult to compare the relative safety of the BTKis being evaluated in MS clinical trials as the existing safety data are based on relatively small, phase II trials in pwMS, or extrapolated from clinical trials of other disease states that have wide variation in sample sizes and patient characteristics. As such, ongoing phase III clinical trials of the various BTKis in pwMS will be essential to better understand these agents' relative safety."
Currently, none of the BTKIs discussed in this review have been approved by the FDA for the treatment of MS. However, some of the BTKis discussed may be approved by regulatory agencies for other indications in the near future. In 2021, the FDA granted breakthrough therapy designation to orelabrutinib for the treatment of mantle cell lymphoma [74]. However, none of the BTKIs discussed here have been approved by the FDA for the treatment of MS. On-going Phase III clinical trials of the various BTKIs will be essential to confirm the safety profiles of these agents. As illustrated by the example of ibrutinib, a first-generation BTKI used in B cell malignancies that carries a risk of bleeding and cardiovascular toxicity, differences in off-target effects of BTKIs can result in serious AEs [85].
留言 (0)