Embryonal Rhabdomyosarcoma of the Uterine Cervix: A Clinicopathologic Study of 94 Cases Emphasizing Issues in Differential Diagnosis Staging, and Prognostic Factors
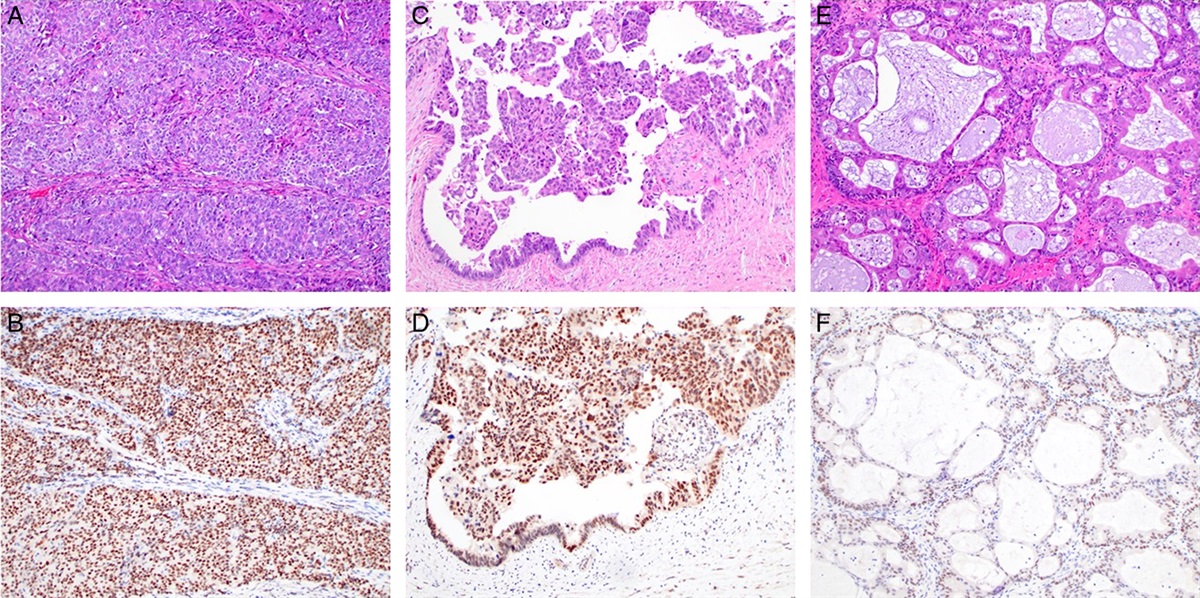
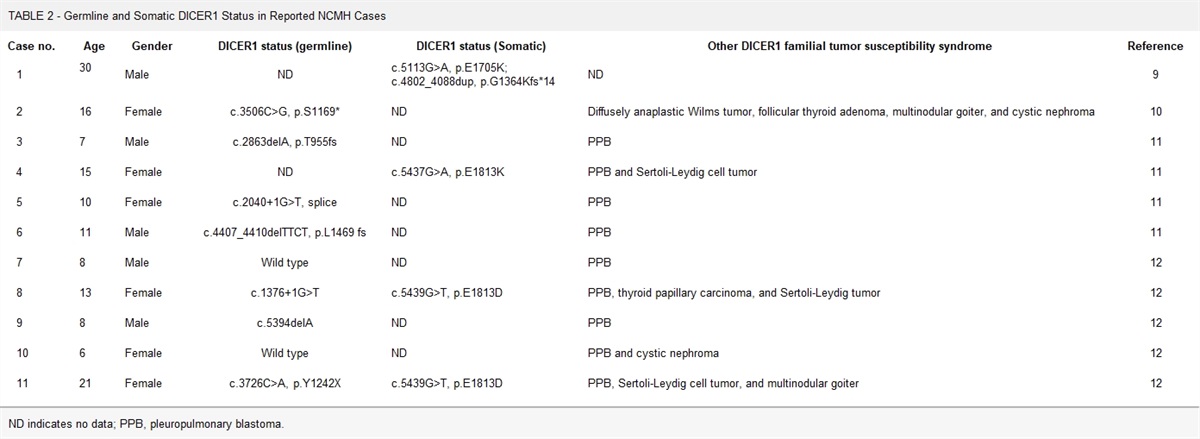
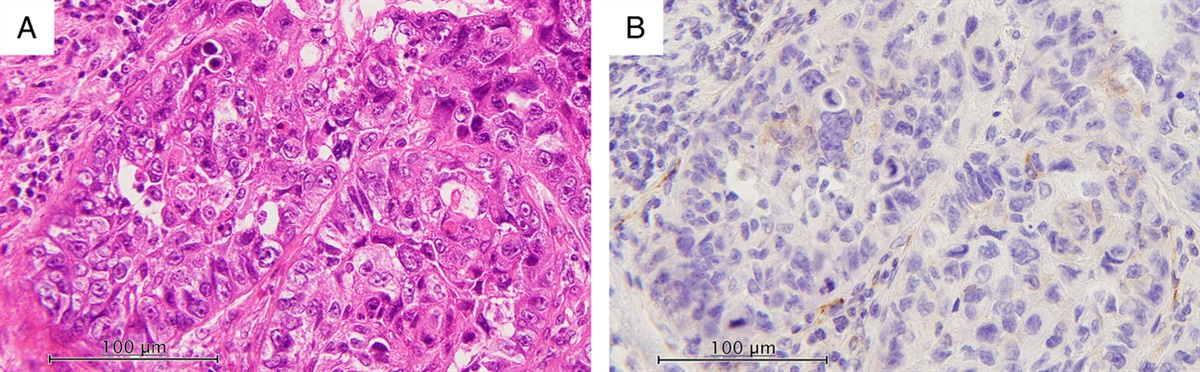
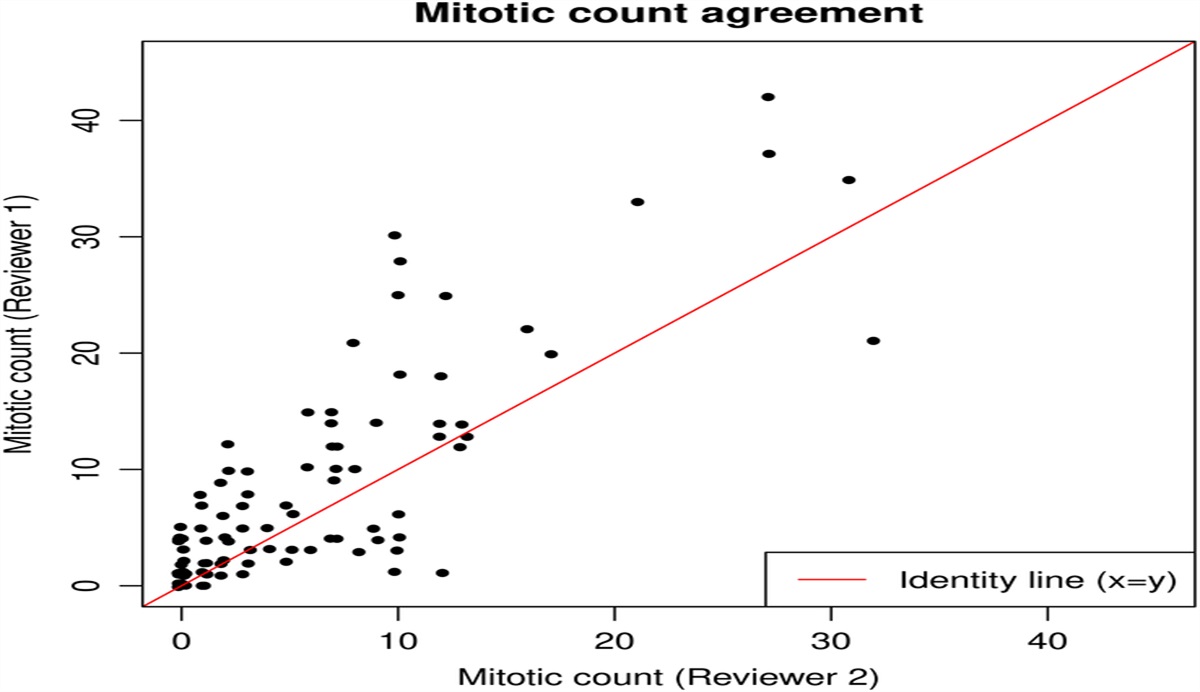
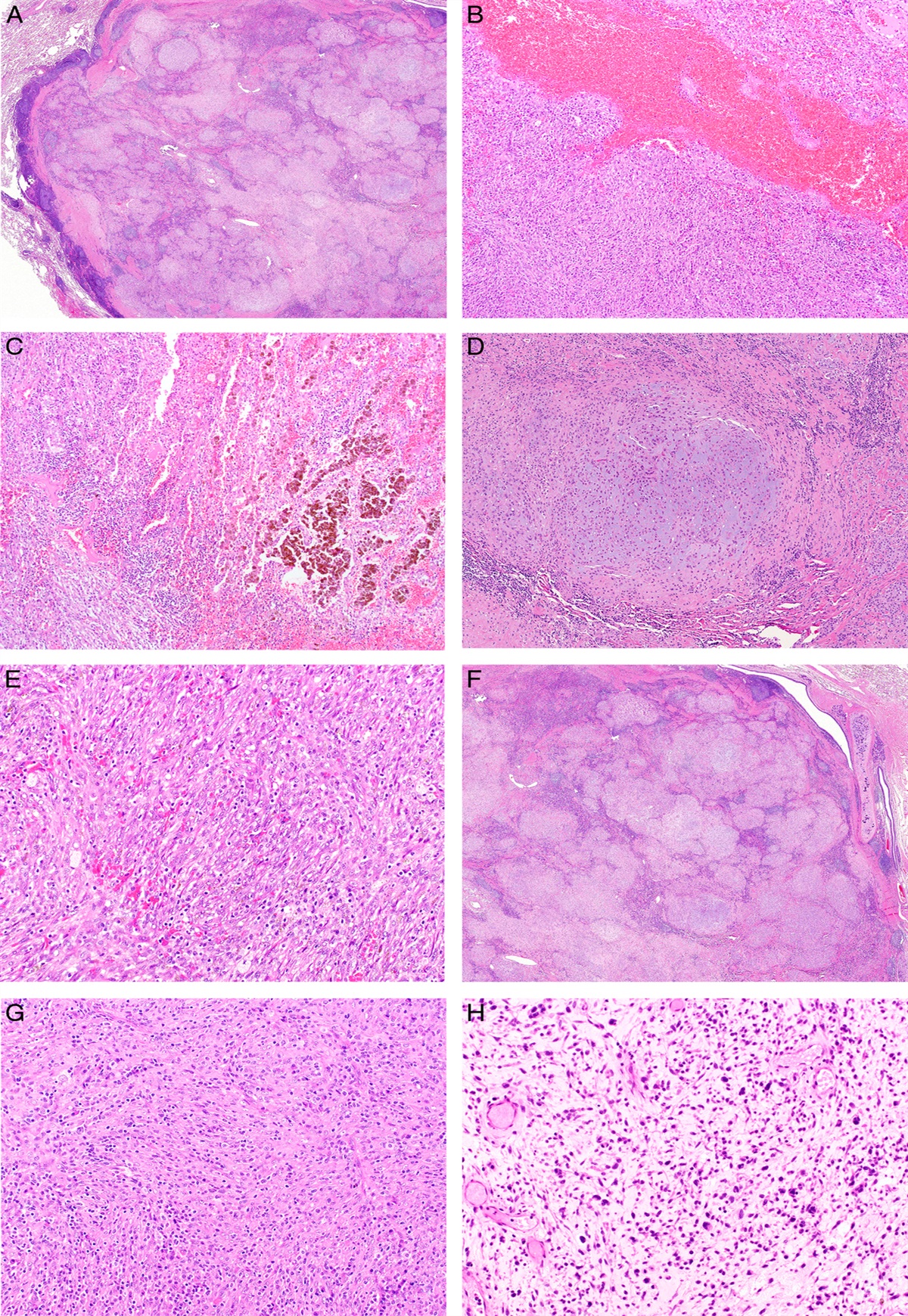
Embryonal rhabdomyosarcoma of the uterine cervix (cERMS) is rare and frequently associated with DICER1 mutations. We report 94 tumors that arose in patients aged 7 to 59 (median=23) years and presented with vaginal bleeding (52), protruding vaginal mass (17), cervical polyp (8), or expelled tumor fragments per vagina (5). Nine had DICER1 syndrome, 8 of whom had other syndromic manifestations including ovarian Sertoli-Leydig cell tumor (7), multinodular goiter (3), pleuropulmonary blastoma (2), pineoblastoma (1), and osteosarcoma (1). Syndromic patients were younger than nonsyndromic patients (16 vs. 24 y). Tumor size ranged from 2 to 24 (median=4.5) cm. Ninety-two tumors were polypoid, most being grape-like (77 of 92). They were characterized by aggregates of primitive cells, almost always exhibiting a cambium layer, within a variably myxoedematous stroma and were hypocellular (63), moderately cellular (22), or hypercellular (9). Entrapped glands, typically scant, were present in 84 tumors. Primitive hyperchromatic ovoid to spindled cells with minimal cytoplasm predominated but differentiated rhabdomyoblasts with abundant eosinophilic cytoplasm (having cross-striations in 30) were seen in 83 tumors; they were often sparse but predominated in three. Nine tumors showed areas of intersecting fascicles and 4 zones with densely cellular (solid) growth. Cartilage was present in 38. Anaplasia was seen in 15 tumors, as was necrosis. Mitotic activity ranged from 1 to 58/10 high-power fields (median=8). The varied microscopic features resulted in a spectrum of differential diagnostic considerations, mainly typical and cellular forms of fibroepithelial polyps, Mullerian adenosarcoma, and other sarcomas. Follow-up was available for 79 patients ranging from 6 to 492 (median=90) months. Treatment information was available in 62 and included polypectomy in 6 patients (2 also received chemotherapy), limited resection in 26 (14 also received chemotherapy), hysterectomy in 29 (15 with adjuvant chemotherapy), and biopsies only in 1 (with chemotherapy). Staging was possible in 56 tumors; according to the “uterine sarcoma” system (tumor size and extent) they were: stage I (10/56; could not be further subclassified as size not available), IA (22/56), IB (18/56), IIA (2/56), IIB 3/56), IIIC (1/56). According to the “adenosarcoma” system (depth of invasion and extent) they were: stage IA (26/56), IB (14/56), IC (10/56), IIA (2/56), IIB (3/56), IIIC (1/56). Eight patients had local recurrence following incomplete excision (10%). Eleven of 79 patients had extrauterine recurrences (14%) and 9 died of disease (11%). Older age was associated with extrauterine recurrence (median 44 vs. 22; P=0.002) and decreased disease-specific survival (median 44 vs. 22; P=0.02). For patients with tumors initially confined to the cervix, the adenosarcoma staging system was superior to the uterine sarcoma staging system for predicting survival (P=0.02). Three patients with DICER1 syndrome who underwent fertility-preserving surgery developed a second primary cERMS 7, 7, and 12 years after their primary tumor. All 9 patients with DICER1 syndrome had tumors confined to the cervix and none died of disease. This study highlights the intriguing clinical aspects of cERMS including its long-known tendency to occur in the young but also more recently appreciated association with DICER1 syndrome. Establishing the diagnosis may still be difficult because of the hazard of sampling a neoplasm which in areas may appear remarkably bland and also because of its potential confusion with other neoplasms. This study indicates that this tumor has a good prognosis at this site and in selected cases a conservative surgical approach is a realistic consideration.

留言 (0)