
記住我
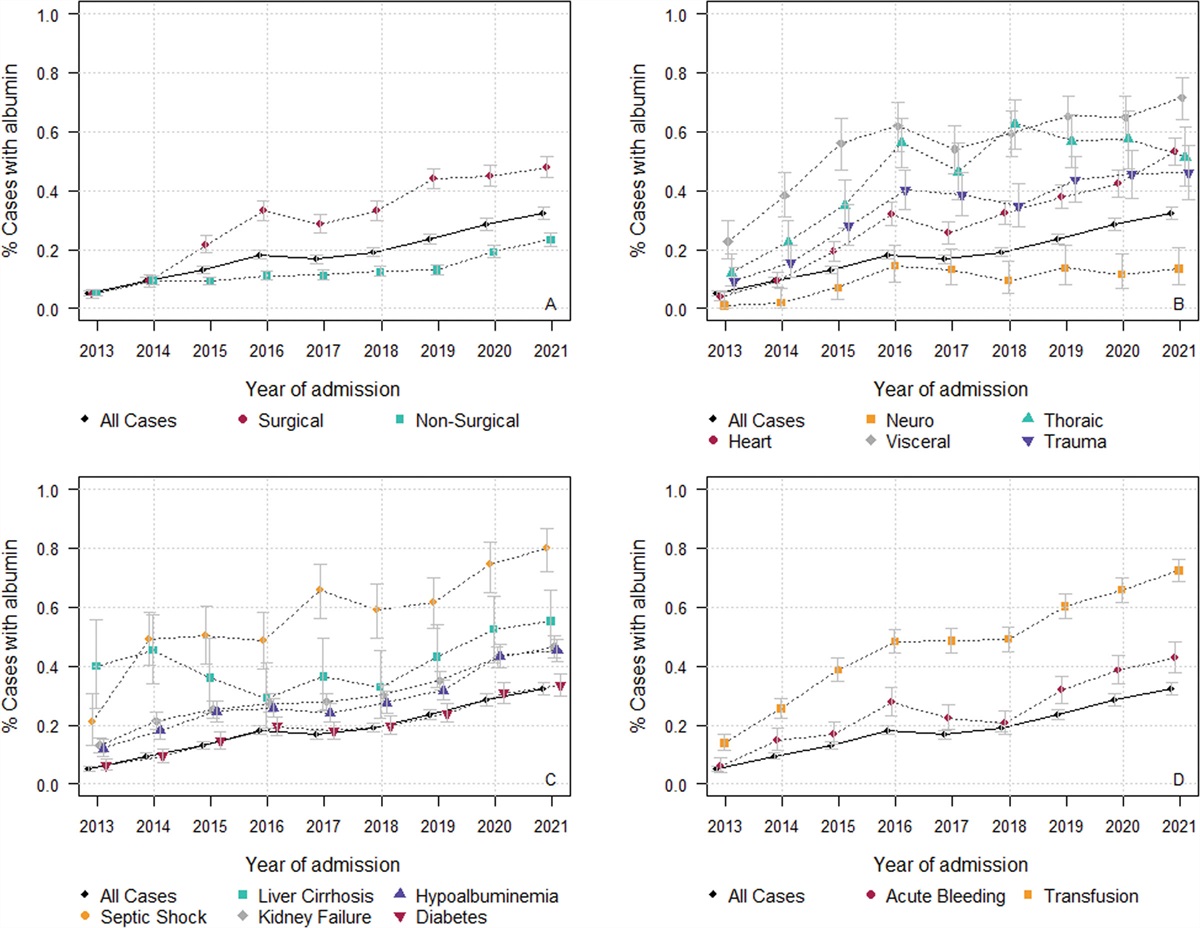
The disparity between the supply of organs to match the growing transplantation needs has driven the development of donation after the circulatory determination of death (DCDD). Controlled DCDD (cDCDD) is now performed in 15 countries throughout the world (Fig. 1), but organ damage caused by the ischemia that is inherent to the cDCDD pathway is a limiting factor for its expansion.
 Figure 1.:
Figure 1.: Activity of controlled donation after the circulatory determination of death (DCD) in countries reporting to the global observatory on donation and transplantation. Rates per million population (pmp). Absolute number of donors is shown in brackets. Year 2020. *Includes cases of donation after medical assistance in dying.
Normothermic regional perfusion (NRP), based on the use of extracorporeal membrane oxygenation (ECMO) devices to restore blood flow in the donor after death and prior to organ recovery, has emerged as an optimal preservation strategy to improve organ utilization and outcomes of transplant recipients in cDCDD (1). An extracorporeal pump and a membrane oxygenator are used to recover donor venous blood, oxygenate it, and return it to the arterial circulation of the region of interest—usually the abdominal cavity (abdominal NRP [A-NRP]). An occlusion balloon or a clamp is placed at the thoracic aorta to restrict circulation to the abdominal region and avoid perfusion of the brain (2). In cases where the donation of the heart is considered, the re-establishment of circulation after death may be extended to the thorax (thoraco-abdominal NRP [TA-NRP]), with the clamping of aortic arch vessels (3). This in situ preservation strategy restores cellular energy substrates, removes metabolic waste products, and induces antioxidant and other protective mechanisms against ischemia-reperfusion injury. The technique also allows clinicians to validate organs before recovery. Finally, NRP turns an urgent into an elective recovery procedure, with the potential of reducing organ damage and losses due to surgical accidents (2).
NRP is routine practice in Spain and compulsory for liver recovery in France and Italy. The use of NRP is expanding in other countries, with a clear need for a well-funded and well-designed infrastructure (4). There are different approaches to the practice of NRP, according to local regulatory frameworks. For example, antemortem cannulation or identification of femoral vessels is allowed in Belgium, France, Italy, Norway, Spain, and Sweden, whereas banned in the United Kingdom.
There are recognized ethical controversies about the use of NRP in cDCDD. To help address such concerns, a first question to answer is whether NRP is worth it from the perspective of recipients in need. The straightforward answer is yes, it is.
NRP Improves Posttransplant Outcomes of Abdominal Organs and Makes Heart Transplantation PossibleA-NRP has shown benefits in cDCDD liver transplantation. Early experiences showed a reduction in primary nonfunction and biliary complications (5,6,7). More recently, two multicenter studies performed in Spain and the United Kingdom revealed that A-NRP makes a significant difference in cDCDD liver transplant outcomes compared with the standard rapid recovery (SRR) technique (8,9). In the largest experience published so far, including more than 800 cDCDD liver transplants, A-NRP was associated with improved patient and graft survival and a significant reduction in the occurrence rate of early allograft dysfunction, thrombosis of the hepatic artery, ischemic cholangiopathy (IC), and all-type biliary complications (10). Gaurav et al (10) compared the outcomes of recipients of cDCDD liver grafts obtained with SRR (n = 97) versus NRP (n = 69) versus ex situ normothermic machine perfusion (NMP) (n = 67). Both NRP and NMP were associated with improved early posttransplant outcomes, but NRP had advantages over NMP and static cold storage after adjusting for donor, recipient, and transplant factors. Importantly, A-NRP allows to safely expand donor age in cDCDD liver transplantation—advanced donor age being a recognized risk factor for IC in this type of donation (10).
Contrary to what described in liver transplantation, the benefits of NRP in kidney transplantation were not that clear, although preliminary experiences reported a decreased occurrence rate of delayed graft function (DGF), with no impact upon graft survival (6,7,8). However, in a recent multicenter Spanish experience including more than 2,000 cDCDD kidney transplants, A-NRP lead to a decreased risk of DGF and 1-year graft loss in a propensity score matching model (11).
In a systematic review and meta-analysis, De Beule et al (1) confirmed the improved outcomes of cDCDD liver and kidney transplants that are obtained when using A-NRP—summarized above. A-NRP seems feasible and safe in cDCDD pancreas transplantation, but large series have not been reported.
There are few experiences on cDCDD heart transplantation using TA-NRP. The Papworth group described the outcomes of 100 cDCDD donor hearts, with similar recipients’ outcomes than those described for recipients of donors after the neurologic determination of death (DNDD) (12). There was a trend to better results with TA-NRP compared with SRR, although ex situ machine perfusion was also applied in both groups. Small successful experiences have been published on cDCDD heart transplantation using TA-NRP followed by cold storage in Belgium, Spain, and the United States (13,14,15). Although results are promising, the limited number of cases and the short follow-up of recipients warrant further investigation.
Because of improved posttransplant outcomes, A-NRP can help to maximize the number of organs recovered and transplanted in cDCDD, but refined research studies that quantify this impact on organ utilization are needed.
NRP Does Not Have a Negative Impact Upon Lung RecoveryDespite the benefits of A-NRP for abdominal organs, there is scarce information on how this strategy may impact upon the quality of cDCDD donor lungs. The SRR technique for both lungs and abdominal organs is considered the ideal approach, as it simplifies the recovery procedure. The combined strategy of SRR of lungs with A-NRP increases the complexity of donor management and represents a potential conflict with the current approach to cDCDD lung recovery—since it could result in graft damage due to the difference in temperature between the abdominal cavity and the lungs (16). In addition, abdominal grafts can be damaged as a result of low flow in the pump during A-NRP after vena cava clamping or due to intraoperative bleeding.
A recent single-center experience described an outstanding recovery rate for lungs and livers obtained from cDCDD donors with this combined recovery approach (17). In fact, liver and lung recipients transplanted with this technique exhibited in outcomes similar to those obtained with organs from DNDD donors. The rapid spread of A-NRP in cDCDD worldwide calls for new studies to evaluate the impact of this preservation strategy on cDCDD donor lungs. The impact of TA-NRP on DCDD lung transplantation remains unknown, although anecdotal experiences show promising results (16,19,18).
NRP Is Feasible and Cost-Effective Compared With Ex Situ Machine Perfusion TechniquesNRP must be managed by experienced donor coordinators and recovery performed by skilled surgical teams, particularly when using the combined recovery of abdominal and thoracic grafts. Not all centers have enough experience and background to deal with this preservation strategy or count on the required resources. To make this technology available in all donor centers, cooperation agreements may be established, so that teams with the knowledge and expertise provide the needed support. In Spain, authorities have organized mobile ECMO teams to make NRP feasible in small centers, with successful results (19).
A frequent concern about NRP is its potential cost. Although no studies have been published on the economic impact of NRP in cDCDD, additional expenditures associated with NRP range between 2,000 and 3,500 euros per procedure (20). Costs are likely much lower than those of ex situ machine perfusion technologies that are also organ-specific and not necessarily lead to the optimal outcomes observed with NRP (21). NRP is unique in offering the possibility to preserve up to five grafts in the same donor (heart, kidneys, liver and pancreas). Simultaneous treatment of multiple organs using the same device and resources is an advantage of this modality compared with ex situ machine perfusion.
Ethical and Legal Barriers Preclude the Expansion of NRPThe main ethical and legal concern about the use of NRP in cDCDD is related to the re-establishment of circulation in the donor after the determination of death—which could retroactively negate the death diagnosis. The definition of human death is based on the permanent loss of capacity for consciousness and all brainstem functions that may occur as a result of a devastating brain injury or of the permanent loss of circulation (22). The determination of death by circulatory criteria should hence be based on the permanent cessation of circulation—to the brain. Once death has been declared, it must be ensured that circulation to the brain is not restored either spontaneously or artificially. Following the withdrawal of life-sustaining therapies, cases of autoresuscitation have not been observed beyond 5 minutes after the cessation of circulation (23)—which should be the minimum duration of the no-touch period. When NRP is used, technical means must be applied to avoid reperfusion of the brain when the pump is started. Techniques applied to isolate the brain include either a balloon occlusion or surgical clamping of the aorta in A-NRP that can be monitored by the absence of constant pressure at the radial artery (24). When TA-NRP is used, the clamping of aortic arch vessels with drainage to atmospheric or negative pressure diverts collateral flow from the brain (25). Brain activity or brain perfusion should be monitored during the procedure to identity a failed exclusion of circulation to the brain that should lead to halting NRP (e.g., at a minimum, the bispectral index is required in Spain). Intentionally excluding circulation to the brain is not the cause of death of the patient, but the disease or condition that lead to the decision to withdraw life-sustaining therapies. Furthermore, it respects the decisions made by the donor or their surrogates of not resuscitation and of maximizing the benefit of organs to be used for transplantation (3). Thus, it can be considered ethically appropriate.
We acknowledge the relevance of ongoing debates about the ethical issues surrounding NRP in cDCDD and the need for frameworks that regulate its use and set appropriate safeguards. But, we are also convinced that efforts should be made to facilitate the implementation of a preservation strategy that can increase the number of organs available for transplantation and improve posttransplant outcomes, helping us make the most of the altruistic gesture of organ donation.
REFERENCES 1. De Beule J, Vandendriessche K, Pengel LHM, et al.: A systematic review and meta-analyses of regional perfusion in donation after circulatory death solid organ transplantation. Transpl Int. 2021; 34:2046–2060 2. Miñambres E, Rubio JJ, Coll E, et al.: Donation after circulatory death and its expansion in Spain. Curr Opin Organ Transplant. 2018; 23:120–129 3. Domínguez-Gil B, Ascher N, Capron AM, et al.: Expanding controlled donation after the circulatory determination of death: Statement from an international collaborative. Intensive Care Med. 2021; 47:265–281 4. Lomero M, Gardiner D, Coll E, et al.; European Committee on Organ Transplantation of the Council of Europe (CD-P-TO): Donation after circulatory death today: An updated overview of the European landscape. Transpl Int. 2020; 33:76–88 5. Rojas-Peña A, Sall LE, Gravel MT, et al.: Donation after circulatory determination of death: The University of Michigan experience with extracorporeal support. Transplantation. 2014; 98:328–334 6. Oniscu GC, Randle LV, Muiesan P, et al.: In situ normothermic regional perfusion for controlled donation after circulatory death–the United Kingdom experience. Am J Transplant. 2014; 14:2846–2854 7. Miñambres E, Suberviola B, Dominguez-Gil B, et al.: Improving the outcomes of organs obtained from controlled donation after circulatory death donors using abdominal normothermic regional perfusion. Am J Transplant. 2017; 17:2165–2172 8. Watson CJE, Hunt F, Messer S, et al.: In situ normothermic perfusion of livers in controlled circulatory death donation may prevent ischemic cholangiopathy and improve graft survival. Am J Transplant. 2019; 19:1745–1758 9. Hessheimer AJ, de la Rosa G, Gastaca M, et al.: Abdominal normothermic regional perfusion in controlled donation after circulatory determination of death liver transplantation: Outcomes and risk factors for graft loss. Am J Transplant. 2022; 22:1169–1181 10. Gaurav R, Butler AJ, Kosmoliaptsis V, et al.: Liver transplantation outcomes from controlled circulatory death donors: SCS vs in situ NRP vs ex situ NMP. Ann Surg. 2022; 275:1156–1164 11. Padilla M, Coll E, Fernández-Pérez C, et al.: Improved short-term outcomes of kidney transplants in controlled donation after the circulatory determination of death with the use of normothermic regional perfusion. Am J Transplant. 2021; 21:3618–3628 12. Messer S, Cernic S, Page A, et al.: A 5-year single-center early experience of heart transplantation from donation after circulatory-determined death donors. J Heart Lung Transplant. 2020; 39:1463–1475 13. Tchana-Sato V, Ledoux D, Detry O, et al.: Successful clinical transplantation of hearts donated after circulatory death using normothermic regional perfusion. J Heart Lung Transplant. 2019; 38:593–598 14. Hoffman JRH, McMaster WG, Rali AS, et al.: Early US experience with cardiac donation after circulatory death (DCD) using normothermic regional perfusion. J Heart Lung Transplant. 2021; 40:1408–1418 15. Miñambres E, Royo-Villanova M, Pérez-Redondo M, et al.: Spanish experience with heart transplants from controlled donation after the circulatory determination of death using thoraco-abdominal normothermic regional perfusion and cold storage. Am J Transplant. 2021; 21:1597–1602 16. Miñambres E, Ruiz P, Ballesteros MA, et al.: Combined lung and liver procurement in controlled donation after circulatory death using normothermic abdominal perfusion. Initial experience in two Spanish centers. Am J Transplant. 2020; 20:231–240 17. Mora V, Ballesteros MA, Naranjo S, et al.: Lung transplantation from controlled donation after circulatory death using simultaneous abdominal normothermic regional perfusion: A single center experience. Am J Transplant. 2022; 22:1852–1860 18. Urban M, Castleberry AW, Markin NW, et al.: Successful lung transplantation with graft recovered after thoracoabdominal normothermic perfusion from donor after circulatory death. Am J Transplant. 2022; 22:294–298 19. Pérez Redondo M, Alcántara Carmona S, Fernández Simón I, et al.: Implementation of a mobile team to provide normothermic regional perfusion in controlled donation after circulatory death: Pilot study and first results. Clin Transplant. 2020; 34:e13899 20. Boteon YL, Hessheimer AJ, Brüggenwirth IMA, et al.: The economic impact of machine perfusion technology in liver transplantation. Artif Organs. 2022; 46:191–200 21. Muller X, Mohkam K, Mueller M, et al.: Hypothermic oxygenated perfusion versus normothermic regional perfusion in liver transplantation from controlled donation after circulatory death: First international comparative study. Ann Surg. 2020; 272:751–758 22. Shemie SD, Hornby L, Baker A, et al.; The International Guidelines for Determination of Death phase 1 participants, in collaboration with the World Health Organization: International guideline development for the determination of death. Intensive Care Med. 2014; 40:788–797 23. Dhanani S, Hornby L, van Beinum A, et al.; Canadian Critical Care Trials Group; Canadian Donation and Transplantation Research Program: Resumption of cardiac activity after withdrawal of life-sustaining measures. N Engl J Med. 2021; 384:345–352 24. Perez-Villares JM, Rubio JJ, Del Río F, et al: Validation of a new proposal to avoid donor resuscitation in controlled donation after circulatory death with normothermic regional perfusion. Resuscitation. 2017; 117:46–49 25. Manara A, Shemie SD, Large S, et al: Maintaining the permanence principle for death during in situ normothermic regional perfusion for donation after circulatory death organ recovery: A United Kingdom and Canadian proposal. Am J Transplant. 2020; 20:2017–2025
留言 (0)