
記住我
The ICU provides health services to patients with complex and critical conditions (1). Delirium, an acutely disturbed state of consciousness, characterized by sudden onset or fluctuating course, inattention, and disorganized thinking (2), impacts up to 50% of critically ill patients (3), Delirium may lead to worse patient and health system outcomes, such as increased risk of long-term cognitive impairment, mental health problems (e.g., anxiety), higher risk of mortality, and higher healthcare costs (3–7).
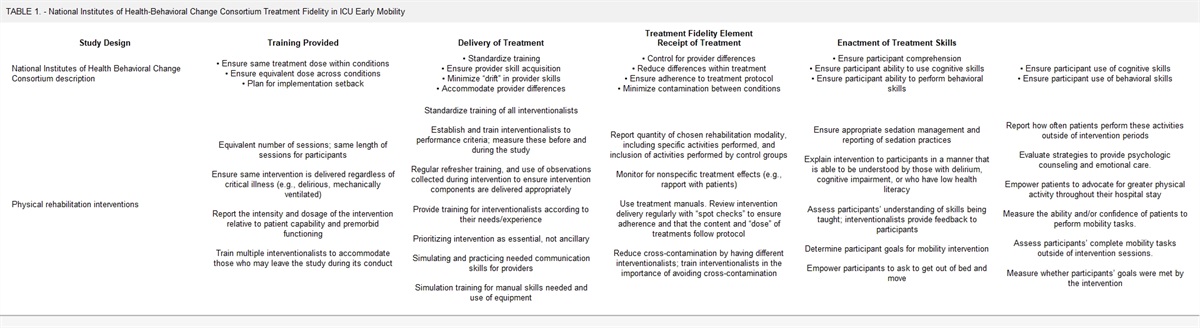
Delirium is difficult to detect and manage given its fluctuating course, numerous risk factors (e.g., age, sedatives, infection, sleep deprivation), and resistance to pharmacologic management (8). Given this, the Society of Critical Care Medicine (SCCM) guidelines highlight the management and treatment of delirium as top priority for future research (5). Nonpharmacologic therapies (e.g., early mobilization) are preferred over pharmacologic interventions to prevent and manage delirium in the critically ill (8,9). A systematic review reported that pharmacologic prophylaxis for the prevention and the treatment of delirium was not only ineffective (8), but in some cases (administration of rivastigimine in patients with high delirium severity) led to increased mortality (9). Conversely, the use of nonpharmacologic interventions such as cognitive stimulation, maintenance of sleep, and mobilization reduces the prevalence of delirium in critically ill patients (5,10).
Family members of critically ill patients may help facilitate nonpharmacologic delirium prevention and management interventions such as maintaining a day/night schedule, promoting early mobilization, and general environmental support (e.g. hygiene routine) (11,12). The SCCM recommends that regular communication between patient, families, and providers such as meetings, attendance of rounds, and in person or telephone call updates is important for Patient Family Centered Care. Family member presence in the ICU may relieve patient anxiety by providing familiarity to patients (13). As such, family presence may help minimize delirium burden among patients admitted to ICUs. Few studies have investigated the impact of family presence on the prevalence of delirium, and to our knowledge, none have assessed the impact of family presence on the duration of delirium in critically ill patients (14,15). The purpose of this study was to evaluate the association between family presence and: 1) delirium prevalence (primary outcome) and 2) duration of delirium among adults admitted to ICU (secondary outcome).
METHODSThis retrospective cohort study was reported according to STrengthening of Reporting of OBservational studies in Epidemiology (16) and REporting of studies Conducted using Observational Routinely-collected Data statement (eTable 1, https://links.lww.com/CCM/H191) (17). The project was approved by the Conjoint Health Research Ethics Board at the University of Calgary (REB17-0389).
Study PopulationThe study population consisted of patients admitted to any of 14 general medical-surgical ICUs in Alberta, Canada, between January 1, 2014, and December 30, 2018. All included ICUs used the same standard of care that includes 24 hours a day, 7 days a week open visitation hours, and routine delirium assessment, prevention, and management (18). The Province of Alberta has an ICU Delirium Framework that provides standardized surveillance for delirium and requires ICUs to develop locally tailored sedation strategies. Sedation was delivered according to local guidelines within each participating ICU. There was no limitation on the number of visitors or time allowed to stay in the ICU. Patients were included if they met the following criteria: 1) age 18 years old or older, 2) had at least one assessment of delirium using the Intensive Care Delirium Screening Checklist (ICDSC) during their ICU stay, 3) stayed at least 24 hours in the ICU, 4) had data that was linked to the Discharge Abstract Database (DAD), and 5) resided in Alberta at the time of ICU admission (to ensure population from Alberta).
Data SourcesPatient clinical information was extracted from eCritical, a population-based bedside clinical information system which captures real-time clinical data for all adult ICU patients in Alberta (19). eCritical was linked to the DAD, which includes demographic, diagnostic, and procedural data on all patients discharged from the hospital (20). Using deterministic linkage to eCritical, the DAD was used to confirm Alberta residency status (20).
Measurement of Exposure: Family PresenceFamily presence was recorded in eCritical as free-text, making it time-consuming to categorize manually (21,22). To eliminate this barrier, a natural language processing (NLP) algorithm was developed by our team (K.K., F.L.) to determine family presence from the medical record (21). The NLP algorithm was developed by analyzing human language documented in eCritical (21,23) using a rule-based classifier training, which uses “IF-THEN” rules (21). If a record for a patient contained information related to the defined inclusion category (condition 1, e.g., “Phone Calls”) and subcategory (condition 2, e.g., “Comment on Family Phone Call”), then the record was classified as “true,” which was indicative of family presence (eTable 2, https://links.lww.com/CCM/H191). Family included relatives and friends and was defined by the algorithm’s inclusion criteria variables (i.e., parent, child, sibling, significant other, details in eTable 3, https://links.lww.com/CCM/H191). The algorithm also captured the mode of family presence (e.g., in-person or telephone call), yielding a three-level exposure used in the study: 1) family physical presence in ICU (in-person), 2) telephone call (telephone call(s) from family and no in-person presence), or 3) no in-person family presence or telephone call (reference group, determined by rule-based classifier exclusion, details in eTable 3 [https://links.lww.com/CCM/H191]).
The NLP algorithm used in this study was validated in a retrospective cohort study using randomized adult patients admitted to 15 ICUs in Alberta (21). The study tested over 2,700 NLP methods to specifically identify family presence from free text (21). The best performed NLP method used rule-based classification as described above (21). The area under the receiver operating characteristic curves ranged from 0.882 to 0.975 based on the mode of family presence when comparing the performance of the rule-based classifier with a reference standard manual chart review (21).
Measurement of Outcomes: ICDSCAmong eligible patients with a Richmond Agitation and Sedation Scale (RASS) score greater than –4, bedside nurses in all Alberta ICUs assess delirium twice per shift (morning and night) (24), using the ICDSC (25). This has been standard practice since 2012. The ICDSC is a validated eight-item delirium assessment tool for use in the ICU (1 point per item [i.e., inattention, disorientation] minimum 0 and maximum 8) (26). Scores of greater than or equal to 4 of 8 on the ICDSC are indicative of delirium (sensitivity: 99%; specificity: 64) (26). For the primary outcome, prevalent delirium was defined as an ICDSC score of greater than or equal to 4 that occurred after documentation of family presence. The secondary outcome, duration of delirium (in patients who had delirium), was measured as the total number of ICU days (24-hr periods) with a positive ICDSC score (≥ 4 points). Proportion of days with delirium (secondary analysis) was calculated by dividing the number of days with delirium (ICDSC score ≥ 4 of 8) by the total length of ICU stay the patient was eligible for a delirium assessment (i.e., RASS > –4) and subsequently reported in the following strata: 0–24.99%, 25–49.99%, 50–74.99%, 75–100%.
Measurement of Delirium Risk Factors, Modifiers, and ConfoundersSelected covariates to include in the regression models were informed by previous studies (4,15,27,28) (provided in detail in Appendix 1, https://links.lww.com/CCM/H191). We collected patient characteristics (age, sex, chronic health conditions, Clinical Frailty Scale [29]) and clinical characteristics (admitting Acute Physiology And Chronic Health Evaluation [APACHE] II score (30), Sequential Organ Failure Assessment, GCS at admission (31), Charlson Comorbidity Index score, ICU admission type, invasive/noninvasive mechanical ventilation, dialysis, vasoactive medication, continuous renal replacement therapy, RASS (24), and ICDSC [32]) from eCritical. Hospital characteristics were also collected, such as teaching status, hospital type, and hospital size.
Data AnalysisStatistical analyses were performed using Stata Version 16.0 (StataCorp, College Station, TX), and the two-sided significance level was set at 5%, with 95% CIs accompanying estimates. Patient characteristics were summarized using descriptive statistics (i.e., mean, median, proportions). Methods of data handling and cleaning are described in eTable 4 (https://links.lww.com/CCM/H191) (20,33,34).
Multivariable mixed-effects logistic and linear regression were used to evaluate the association between family presence (physically present in the ICU, telephone call only, no presence or telephone calls [reference group]) and prevalence (outcomes of association are presented as odds ratios [ORs]) and duration (regression estimates reflecting the difference in mean days of delirium between groups) of delirium, respectively. Family presence was categorized as family physical presence in the ICU during or prior to patient delirium onset. The above models were performed using a mixed-effects modeling to compare estimates when data were analyzed after accounting for clustering by ICU site and ICU readmission and standard errors of repeated measures. The analysis accounted for both random and fixed effects (34). Random effects represent shared effects of each patient (34,35), which means the outcomes of patients were allowed to vary in defined aggregated group means (ICU readmission, ICU site). Results from the mixed-effects analysis were reported where the omnibus test was significant, meaning it is necessary to adjust estimates for either patient readmission, ICU site, or both. Covariates in models were assessed as potential effect measure modifiers prior to an assessment of confounding by examining the significance of interaction terms in each model (effect modification present if p < 0.05). Sensitivity analyses were performed: 1) excluding those who died in the ICU and 2) comparing family presence as a binary variable (grouping physical presence and call). Secondary analyses were completed to explore granular patient diagnoses (e.g., cancer, trauma) for each admission type and percentage days with delirium stratified by family presence (36).
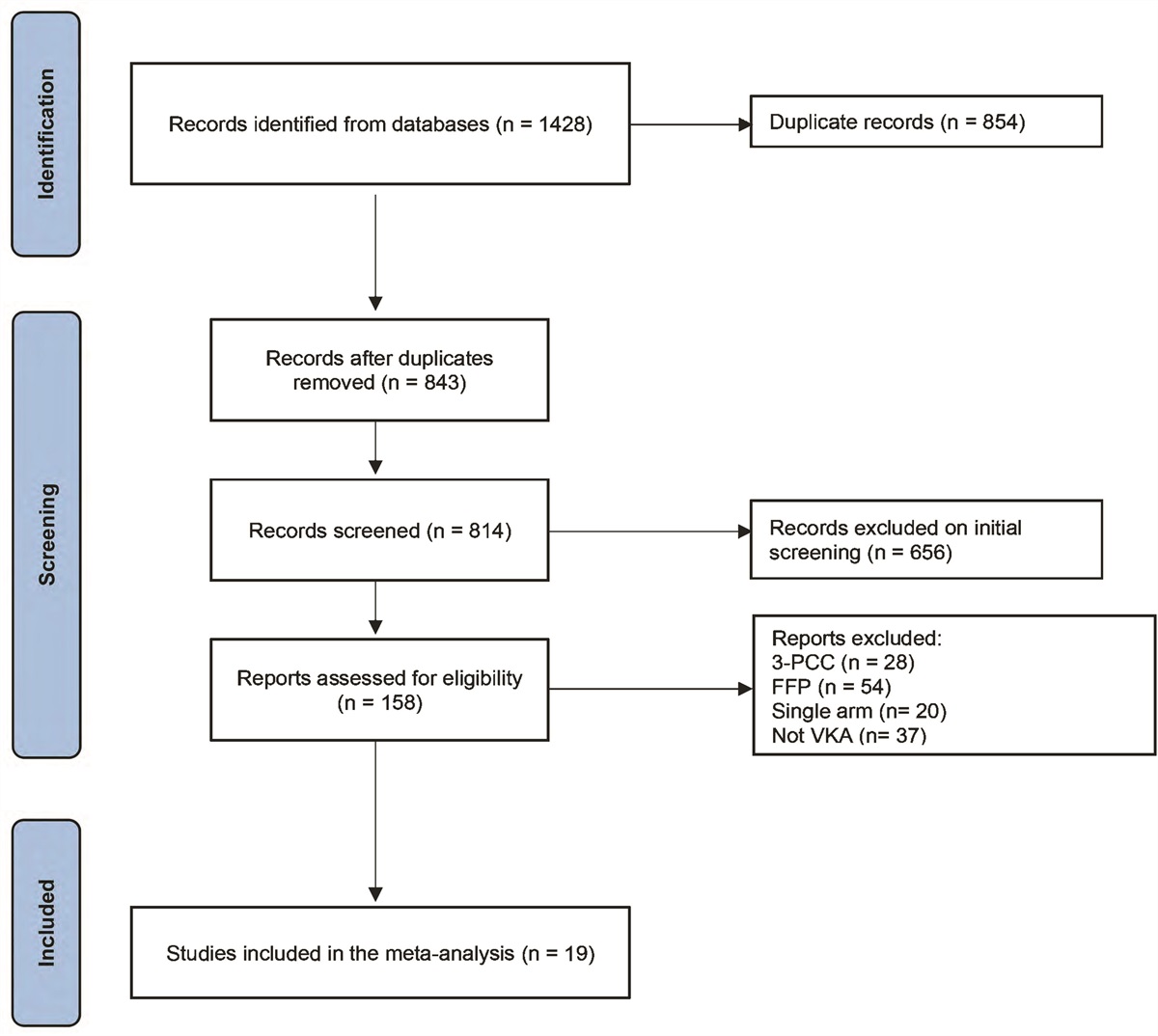
RESULTS Study PopulationBetween January 1, 2014, and December 31, 2018, 47,195 unique patients were admitted at least once to an Alberta ICU. A total of 36,496 unique patients met initial inclusion criteria (Fig. 1). Of those patients, 10,396 patients (28.4%) did not have the complete data required to determine family presence and the mode using the family presence algorithm, leaving 14,847 patients with delirium for the secondary outcome (eTable 5, https://links.lww.com/CCM/H191). For the primary outcome, 563 patients had delirium prior to family exposure, leaving 25,537 unique patients in the study population. Included patients had a median age of 59 years (interquartile range [IQR], 46–70 yr), were predominately male (n = 14,690; 57.5%), and were admitted for medical reasons (n = 18,600; 74.7%), and 2,107 (8.3%) died in the ICU (Table 1). The median ICDSC score during ICU stay was 4 (IQR, 2–6), and 14,284 had delirium at least once during their ICU stay (55.9%; 95% CI, 55.3–56.5%) (eTable 6, https://links.lww.com/CCM/H191). Patients who had family members present in the ICU had a median admission APACHE-II score of 19 (IQR, 14–25), whereas those with a family telephone call or no ICU family present had a median APACHE-II score of 17 (IQR, 12–22) and 14 (IQR, 10–19), respectively (Table 1). The most common ICU admitting diagnoses by admission type are shown in eTable 7 (https://links.lww.com/CCM/H191).
TABLE 1. - Demographic and Clinical Characteristics of the Study Population (Primary Outcome) Characteristics Family presence Total (N = 25,537) Physical Presencea (N = 23,121) Telephone Callb (N = 591) No Visitc (N = 1,825) Age, yr, median (IQR) 59 (46–70) 59 (46–70) 59 (49–68) 58 (47–67) Sex, female, n (%) 10,847 (42.5) 9,980 (43.2) 202 (34.2) 665 (36.4) Patient admitting type, n (%)d Elective-surgical 2,018 (8.1) 1,597 (7.0) 65 (11.4) 356 (21.5) Emergency-surgical 4,285 (17.2) 3,904 (17.2) 1.07 (18.7) 274 (16.5) Medical 18,600 (74.7) 17,171 (75.7) 400 (69.9) 1,029 (62.0) Admission Acute Physiology and Chronic Health Evaluation II score, median (IQR) 19 (14–25) 19 (14–25) 17 (12–22) 14 (10–19) Charlson Comorbidity Index, median (IQR) 1 (0–3) 1 (0–2) 1 (0–2) 0 (0–2) Admission Sequential Organ Failure Assessment score, median (IQR) 6 (4–9) 6 (4–9) 5 (3–8) 4 (2–6) Admission GCS score, median (IQR) 14 (10–15) 14 (10–15) 15 (13–15) 15 (14–15) GCS score 15 by, n (%) 10,239 (40.1) 8,955 (38.7) 292 (49.4) 992 (54.4) GCS score <15, n (%) 15,298 (60.0) 14,166 (61.3) 299 (50.6) 833 (45.6) Clinical Frailty Score, median (IQR)e 3 (2–5) 3 (2–5) 3 (2–4) 4 (2–4) ICU interventions, n (%) Dialysis 642 (2.5) 575 (2.5) 17 (2.9) 50 (2.7) Vasoactive medication 11,504 (47.4) 10,929 (47.3) 205 (34.7) 369 (20.2) Invasive mechanical ventilation 16,398 (64.2) 15,440 (66.8) 305 (51.6) 653 (35.8) Noninvasive ventilation 3,624 (14.2) 3,415 (14.8) 72 (12.2) 136 (7.5) Continuous renal replacement therapy 1,506 (5.9) 1,485 (6.4) 3 (0.5) 18 (1.0) Hospital length of stay, d, median (IQR) 12 (6–26) 13 (6–27) 10 (5–20.5) 9 (4–17) ICU length of stay, median (IQR) days 4.2 (2.3–8.0) 4.5 (2.6–8.6) 2.7 (1.9–4.1) 2.1 (1.6–3.4) Died in ICU, n (%) 2,107 (8.3) 2,076 (9.0) 11 (1.9) 20 (1.1) Died in hospital, n (%) 3,579 (14.0) 3,479 (15.1) 32 (5.4) 68 (3.7)GCS = Glasgow Coma Scale, IQR = interquartile range.
aFamily physical presence at any time during ICU stay.
bFamily providing telephone call only.
cNo in-person family presence or telephone call.
dSix hundred thirty-four patients missing admission type.
eTwenty-three thousand five hundred two patients missing frailty score.
 Figure 1.:
Figure 1.: Participant flow chart. DAD = discharge abstract database, ICDSC = Intensive Care Delirium Screening Checklist.
Family Presence and Prevalence of Delirium (Primary Outcome)The omnibus test from the mixed-effects model, adjusting for ICU readmission, had a p value of 0.04, suggesting that adjustment of results by ICU readmissions was necessary to assess the relationship between family presence and prevalence of delirium. Family physical presence was associated with increased prevalence delirium in the overall cohort (unadjusted OR [OR], 1.19; 95% CI, 1.11–1.27; p = 0.02), compared with patients in the reference group (eTable 8, https://links.lww.com/CCM/H191). When stratified by admission type (elective-surgical, emergency-surgical, medical; effect modifier, p = 0.01) and whether the patient’s GCS score was intact (GCS = 15 vs < 15; effect modifier, p < 0.001) (concurrent effect modification by GCS and admission type, p < 0.001), family physical presence was associated with lower prevalence of delirium for patients admitted following elective surgery with intact GCS (GCS = 15) (OR, 0.60; 95% CI, 0.39–0.97), compared with patients in the reference group (no family physical presence or telephone call [eTable 8, https://links.lww.com/CCM/H191]). There was a total of 1,375 neurologically intact elective surgical patients with a median age of 62 years (IQR, 51–60 yr) and median APACHE-II score of 13 (IQR, 10–26). There was no significant difference in prevalence of delirium among patients with intact or impaired GCS (GCS = 15 vs <15) in medical and emergency-surgical admissions given family physical or telephone call presence compared with patients in the reference group (Fig. 2; and eTable 8, https://links.lww.com/CCM/H191).
 Figure 2.:
Figure 2.: Forest plot delirium association with physical family presence compared with no family presence or telephone call in the ICU. GCS = Glasgow Coma Scale.
Family Presence and Duration of Delirium (Secondary Outcome)The omnibus test from the mixed-effects regression, adjusting for ICU readmission, had a p value of 0.01, suggesting that adjusting for ICU readmission was necessary to assess the relationship between family presence and delirium duration. After adjusting for covariates, both family physical presence and a family call were associated with decreased duration of delirium (Mean difference [MD] –1.87 d; 95% CI, –2.01 to –1.81 and MD, –1.41 d; 95% CI, –1.52 to –1.31, respectively), as compared to patients in the reference group (Table 2).
TABLE 2. - Association Between Delirium Duration in Days and Family Presence in the ICU Family Presence Adjusted Modela (95% CI) Crude Model (95% CI) (n = 14,847) All Patient Admissionsa (n = 14,847) Physical presenceb (n = 13,984) 1.33 (1.26–1.41); p < 0.001 –1.87 (–2.01 to –1.81); p < 0.001 Family call onlyc (n = 289) –0.74 (–0.86 to –0.63); p < 0.001 –1.41 (–1.52 to –1.31); p < 0.001 No visitd (n = 574) — —aAdjusted for age, sex, hospital type, Acute Physiology and Chronic Health Disease Classification System II score at ICU admission, Richmond Agitation Sedation Scale score at ICU admission, hospital length of stay, ICU length of stay, number of ICU beds, any receipt of invasive mechanical ventilation, Charlson Comorbidity Index score at ICU admission, Sequential Organ Failure Assessment score at admission, and Glasgow Comma Scale score at admission.
bFamily physical presence as defined by physical presence at any time during ICU stay.
cFamily call only as defined by telephone, without physical presence.
dNo visit means that the patient did not receive any physical presence or phone call with their family members.
Dashes indicate reference group for multilevel mixed-effects linear regression analyses.
Sensitivity analysis excluding patients who died in the ICU showed similar results for the association between family presence and the prevalence and duration of delirium (eTables 9 and 10, https://links.lww.com/CCM/H191). The adjusted MD (–1.90 d; 95% CI, –2.13 to –0.73) in patient delirium days comparing family presence (as a binary variable) and the reference group was similar to ICU family physical presence when coded as a three-level exposure (eTable 11, https://links.lww.com/CCM/H191). The association between family presence and percentage days with delirium is shown in eTable 12 (https://links.lww.com/CCM/H191).
DISCUSSIONFew studies have evaluated the effect of family presence on delirium in critically ill patients (37–42). A before-and-after study by Westphal et al (37) found that an increase in visitation hours resulted in a significant (5.4%) reduction in the cumulative prevalence of delirium in critically ill patients. A systematic review reported that flexible visitation policies were associated with reduced frequency of delirium in critically ill patients (pooled OR, 0.39; 95% CI, 0.22–0.69; I2 = 0%) (40). A recent multicenter retrospective cohort study found that family presence in person or virtual was associated with lower risk of delirium (pooled OR, 0.73; 95% CI, 0.63–0.84) in ICU patients with COVID-19 (41). Similarly, our findings support that family physical presence may reduce prevalence of delirium in specific patient subgroups (elective-surgical critically ill patients with intact GCS). Physical family presence was not significantly associated with prevalent delirium in medical and emergency surgical patients. Such results suggest that the association between family physical presence and prevalent delirium in ICU patients is dependent on multiple factors (three-level exposure, effect modification by two variables [GCS and ICU admission type], and confounding), thus highlighting the complexity of both delirium and critical illness. In contrast, a randomized controlled trial of flexible ICU visitation hours reported no association between flexible ICU visitation hours and the prevalence of delirium in critically ill patients (43). We found that family physical presence decreased delirium duration by 2 days when adjusting for patient readmission. Patients who were previously admitted to the ICU may be predisposed to experiencing delirium in their next admission, thereby underestimating the effect of recurrent delirium when analyzing per patient admission (44). If patients are readmitted to an ICU, it may be important for family members to be present to aid in delirium management.
The association between family physical presence and prevalence of delirium in the ICU is highly complex, with the presence of confounding highly likely (e.g. APACHE-II, RASS, ICU mortality) and major differences observed among strata defined by patient admission type, and GCS at admission. As such, family absence could be a modifiable risk factor for prevalent delirium in elective-surgical patients with intact GCS. Patients admitted for elective-surgical reasons have lower risk of developing delirium, compared with patients admitted for emergency-surgical or medical reasons, given that they have less risk factors for delirium such as reduced illness severity (27). ICU patients admitted for medical reasons may have limited benefit from family member presence given their high exposure to nonmodifiable delirium risk factors (i.e., high comorbidity) (27). Patients admitted with intact GCS (i.e., high GCS scores indicating normal consciousness and brain function) can receive cognitive stimulation from family members through family interaction (45). Conversely, patients with impaired GCS (low GCS scores) may not be able to meaningfully engage with their family members due to the patient’s limited capacity (46), thereby restricting potential benefit from interaction with the family member.
Given the high prevalence of delirium and its detrimental outcomes, it is imperative to understand how family member presence impacts patient delirium. Our findings highlight the effect of family presence in the ICU. Future prospective studies may further aid in exploring the complex association between family presence and engagement among different ICU admission types and GCS patient subgroups. Research on defining meaningful family engagement is also needed to optimize provision of opportunities for safe and beneficial family ICU presence and involvement. For example, a recent study showed that it is feasible for family to aid in the detection of delirium, therefore increasing opportunities for them to provide bedside care and aid in shared decision-making (47).
This study has strengths and limitations. Our large population-based sample size (n = 25,537) from all adult ICUs in Alberta is a major strength, increasing the precision of our results. This may allow generalization to other ICUs with similar healthcare systems and populations. Family presence was captured using a novel NLP algorithm developed by our team (16), yielding an accurate representation of family presence compared with quantifying family presence according to visitation policy alone. Our study found that 90.5% of patients had a family member present that is comparable with provincial estimates (i.e., 90%) (48). However, family presence/absence may have been underreported as it required manual documentation of free-text by clinicians and healthcare workers. This may have led to systematic bias of exposure status (i.e., family presence) irrespective of outcome status, thereby biasing estimates of effect toward the null value. Family presence may have been overreported as we coded family as present when family met with ICU nurses or healthcare staff because we assumed that families would visit their loved ones before or after these meetings. Lastly, since this was a retrospective study design, we did not have data on what activities, if any, the family members engaged in. For example, some family members may not have actively engaged with the patient, thus underestimating the effect of active family engagement on prevalence and duration of delirium. Furthermore, no interrater reliability was performed on the ICDSC prior to the current study. However, an ICDSC dashboard on the electronic medical record includes individual items of the ICDSC and additional resources to ensure that delirium is measured consistently among ICU care team members. In addition, we did not account for the use of sedatives (i.e., propofol, fentanyl, midazolam) as a potential confounder in our estimates. The overall ICU mortality of our cohort is 8.3% that is similar to 2016 Canadian ICU mortality of 9% (1). Last, we did not assess for time-dependent change in the prevalence of delirium associated with family presence (exposure). Thus, our results may be a conservative estimate of the association between family presence and delirium in critically ill patients and causality cannot be inferred.
This retrospective population-based cohort study of 25,537 adults admitted to the ICU found that the association between family presence and delirium prevalence was modified by admission type and GCS. Compared with no family visit or telephone call, family physical presence was associated with reduced prevalence of delirium in patients admitted following elective surgery with intact GCS at the time of admission. Irrespective of GCS scores, physical presence of family was not significantly associated with prevalence of delirium in patients admitted for medical and emergency surgical reasons. Family providing telephone calls alone was not significantly associated with delirium prevalence in any patient group. In all patients, family presence, both physically and via telephone call, was associated with reduced duration of delirium compared with when no family physical visits or telephone calls were observed. In general, sicker patients had more in-person visit than those with less severe illness. Our findings suggest that in select critically ill patients, family physical presence may be associated with reduced prevalence of delirium. Additionally, both family physical presence and family providing telephone calls only may be associated with reduced duration of delirium.
CONCLUSIONSThe association between family presence and delirium in ICU patients is complex and modified by reason for ICU admission and brain function. Data suggest that in specific groups (patients with intact GCS admitted following elective surgery), physical presence of family may reduce the prevalence of delirium; however, in other groups there was no association. In all patients, family physical presence in the ICU and telephone call was associated with reduced duration of delirium of up to 2 days and 2 day, respectively. Family member presence (and involvement in care) in the ICU may be an important mechanism to achieve better delirium-related outcomes for critically ill patients. Last, we clarified that the association between family telephone calls and patient care should be further explored.
REFERENCES 1. Canadian Institute for Health Information (CIHI): Care in Canadian ICUs. Ottawa, Canada, CIHI, 2016 2. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. Washington, DC, American Psychiatric Association, 2000 3. Salluh JI, Wang H, Schneider EB, et al.: Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. 2015; 350:h2538 4. Ely E, Shintani A, Truman B, et al.: Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2014; 16:1753–1752 5. Devlin JW, Skrobik Y, Gélinas C, et al.: Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018; 46:e825–e873 6. Collinsworth AW, Priest EL, Campbell CR, et al.: A review of multifaceted care approaches for the prevention and mitigation of delirium in Intensive Care Units. J Intensive Care Med. 2016; 31:127–141 7. Wolters AE, Peelen LM, Welling MC, et al.: Long-term mental health problems after delirium in the ICU. Crit Care Med. 2016; 44:1808–1813 8. Serafim RB, Bozza FA, Soares M, et al.: Pharmacologic prevention and treatment of delirium in intensive care patients: A systematic review. J Crit Care. 2015; 30:799–807 9. van Eijk MM, Roes KC, Honing ML, et al.: Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: A multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010; 376:1829–1837 10. Teixeira C, Rosa RG: The rationale of flexible ICU visiting hours for delirium prevention. Journal of Emergency and Critical Care Medicine. 2018; 2:90–105 11. Gonzalez CE, Carroll DL, Elliott JS, et al.: Visiting preferences of patients in the intensive care unit and in a complex care medical unit. Am J Crit Care. 2004; 13:194–198 12. Martinez FT, Tobar C, Beddings CI, et al.: Preventing delirium in an acute hospital using a non-pharmacological intervention. Age Ageing. 2012; 41:629–634 13. Burns KEA, Misak C, Herridge M, et al.; Patient and Family Partnership Committee of the Canadian Critical Care Trials Group: Patient and family engagement in the ICU. untapped opportunities and underrecognized challenges. Am J Respir Crit Care Med. 2018; 198:310–319 14. Davidson JE: Family presence on rounds in neonatal, pediatric, and adult intensive care units. Ann Am Thorac Soc. 2013; 10:152–156 15. Van Rompaey B, Elseviers MM, Schuurmans MJ, et al.: Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care. 2009; 13:R77 16. von Elm E, Altman DG, Egger M, et al.: The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J Clin Epidemiol 2018; 61:344–349 17. Benchimol EI, Smeeth L, Guttmann A, et al.; RECORD Working Committee: The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. 2015; 12:e1001885 18. Bowker SL, Stelfox HT, Bagshaw SM; Critical Care Strategic Clinical Network: Critical care strategic clinical network: Information infrastructure ensures a learning health system. CMAJ. 2019; 191:S22–S23 19. Brundin-Mather R, Soo A, Zuege DJ, et al.: Secondary EMR data for quality improvement and research: A comparison of manual and electronic data collection from an integrated critical care electronic medical record system. J Crit Care. 2018; 47:295–301 20. Canadian Institute for Health Information: CIHI data quality study of the 2009–2010 discharge abstract database. CIHI Data Quality Study of the 2009–2010 Discharge Abstract Database. 2012 21. Lucini FR, Krewulak KD, Fiest KM, et al.: Natural language processing to measure the frequency and mode of communication between healthcare professionals and family members of critically ill patients. J Am Med Inform Assoc. 2021; 28:541–548 22. Au SS, Roze des Ordons A, Soo A, et al.: Family participation in intensive care unit rounds: Comparing family and provider perspectives. J Crit Care. 2017; 38:132–136 23. Kreimeyer K, Foster M, Pandey A, et al.: Natural language processing systems for capturing and standardizing unstructured clinical information: A systematic review. J Biomed Inform. 2017; 73:14–29 24. Sessler CN, Gosnell MS, Grap MJ, et al.: The Richmond agitation-sedation scale: Validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002; 166:1338–1344 25. Alberta Health Services: Provincial Clinical Knowledge Topic Delirium, Adult – Critical Care. Book Provincial Clinical Knowledge Topic Delirium, Adult – Critical Care. Alberta, Canada, Alberta Health Services, 2017 26. Bergeron N, Dubois MJ, Dumont M, et al.: Intensive care delirium screening checklist: Evaluation of a new screening tool. Intensive Care Med. 2001; 27:859–864 27. Cherak SJ, Rosgen BK, Amarbayan M, et al.: Mental health interventions to improve psychological outcomes in informal caregivers of critically ill patients: A systematic review and meta-analysis. Crit Care Med. 2021; 49:1414–1426 28. Pisani MA, Kong SY, Kasl SV, et al.: Days of delirium are associated with 1-year mortality in an older intensive care unit population. Am J Respir Crit Care Med. 2009; 180:1092–1097 29. Rockwood K, Song X, MacKnight C, et al.: A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005; 173:489–495 30. Wong DT, Crofts SL, Gomez M, et al.: Evaluation of predictive ability of APACHE II system and hospital outcome in Canadian intensive care unit patients. Crit Care Med. 1995; 23:1177–1183 31. Teasdale G, Jennett B: Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974; 2:81–84 32. Fiest KM, Krewulak KD, Brundin-Mather R, et al.; for Sepsis Canada: Patient, public, and healthcare professionals’ sepsis awareness, knowledge, and information seeking behaviors: A scoping review. Crit Care Med
留言 (0)