
記住我

Injuries to the fingertip are common.1 However, severe injuries may result in skin and soft tissue defects with the exposure of the bone, joint, tendon, blood vessels, and nerve, leading to disfigurement and impairment of finger function. Several approaches to repairing injured fingers are being practiced.2 For those injured fingers with bone exposure and local soft tissue defects, stump revision (ie, phalangeal shortening and direct suture) is the simplest and fastest way to recovery.3 The application of an abdominal flap allows possible rescue of the injured fingers.4,5 However, the abdominal flap belongs to the distal flap and has several shortcomings, such as requiring multistage surgeries, poor wear resistance, swollen appearance, poor sense of touch, and requiring hand attachment to another part of the body for up to 3 weeks.6,7 While local flaps, such as the V-Y flaps, have the advantages of having similar texture and sensation to the defect area, their applicability is limited when the defect area is large that the wound cannot be covered.8,9 To overcome these limitations, homodigital island flaps have been reported, which include a neurovascular bundle, and immediate sensory recovery is expected.10 In this study, we aim to provide an easier and more versatile surgical technique to treat fingertip defects. Moreover, the aesthetic and function of fingers were preserved. We compare parallelogram transposition flaps, antegrade homodigital island flaps, and reverse digital artery island flaps in the treatment of PNB356 finger amputation injuries (Fig. 1).11 (Transverse amputation with the loss of distal pulp, nails, and bone was defined as PNB356.)
 FIGURE 1:
FIGURE 1: PNB356 finger amputation injuries. Transverse amputation with the loss of distal pulp, nails, and bone.
METHODOLOGY PatientsFrom January 2017 to January 2021, clinical patient data with parallelogram flaps (78 cases), antegrade homodigital island flaps (78 cases), and reverse digital artery island flaps (78 cases) to repair fingertip defects were collected and analyzed. Two hundred thirty-four cases (234 fingers) were included in our study. The study was submitted to the ethics committee. Patients deemed suitable for this procedure would satisfy the following inclusion criteria: (1) single fingertip injury of one hand, (2) transverse amputation with the loss of distal pulp, nails, and bone. (3) the injured finger had not been longer than 8 hours, (4) 6 mm < advancement required < 10 mm; (5) PNB356 finger amputation injuries; and (6) the patient agreed to participate at the 6-month follow-up.
Researchers coded patients in the order of admission and used SSPS20.0 software to randomly group. All operations were performed by 2 surgical teams who had many years of clinical experience.
Operative Method Harvesting of Skin Flap Group AAccording to the size of the defect, the flap was designed on the side with more residual skin (Figs. 2, 3). Step 1: A longitudinal incision was made along the bone surface on both sides of the fingertip and the incised position should not exceed the transverse crease of the distal interphalangeal joint. Then, the skin and subcutaneous tissue were incised along the edge of the skin, and the skin flap was dissected sharply within the subcutaneous fascia. Step 2: The level of surgical incision is closed to the bone surface of the distal phalanx to avoid injuring the proper digital artery and nerve. Step 3: The most important step is a transverse incision was made on the side with more remaining skin to provide sufficient angle for flap turnover. Step 4: Once freed, the designed flap was flipped over. Given its shape resembling a parallelogram, we named the flap a parallelogram flap. The longest hypotenuse C should be longer than the longitudinal length A + the width of defect B (Figs. 3, 4), which was sufficient to cover the defective area. If the flap could not cover the wound, the length of the transverse incision should be increased. Step 5: After the flap was flipped over, a piece of skin graft A was left on the opposite side. The constructed skin graft A could be used to repair the transferred skin defect B (Fig. 5).
 FIGURE 2:
FIGURE 2: A, Nervi digitales dorsales and nervi digitales palmares. B, Proper palmar digital arteries and dorsal digital arteries. C, Flexor digitorum profundus. D, Flexor digitorum superficialis, E, The level of surgical incision is closed to the surface of the periosteum and the tendon sheath of flexor digitorum profundus.
 FIGURE 3:
FIGURE 3: Surgical steps of the parallelogram flap. A, A longitudinal incision was made along the bone surface on both sides of the fingertip and the incised position should not exceed the transverse striation of the distal interphalangeal joint. B, A transverse incision was made on the side with more remaining skin to provide sufficient angle for flap turnover. If the flap could not cover the wound, the length of the transverse incision should be increased. C, A piece of skin graft A was left on the opposite side and to fill the defect B. D, The parallelogram flap reconstruction and skin grafts are completed.
 FIGURE 4:
FIGURE 4: Schematic drawing of the parallelogram flap. The red represents the injured finger and the black represents the parallelogram flap. The longest hypotenuse C should be longer than the longitudinal length A + the width of defect B.
 FIGURE 5:
FIGURE 5: Intraoperative performance. Patients treated by parallelogram flaps (A, B). Postoperative performance (C, D, E). The procedure of surgery (F, G) 4 months after surgery.
Group BThe operation was performed under local finger anesthesia. The incision was first made at the midaxis of the finger, and then, the neurovascular pedicle proximal end of the flap was exposed and isolated. A finger pulp oblique incision was made to harvest the flap. Afterward, the flap was raised above the superficial flexor tendon of the finger from the distal defect area to the proximal interphalangeal. When the donor flap was raised, sufficient subcutaneous fat was incorporated to ensure maximal cosmetic value. The flap was pulled to the distal defect area in the straight position of the finger, ensuring no tension to the neurovascular bundle in the flap. Finally, the donor area was sutured directly (Fig. 6).
 FIGURE 6:
FIGURE 6: Intraoperative performance. Patients treated by antegrade homodigital island flaps.
Group CThe flap was designed according to the shape and size of the defect and located at the ipsilateral side of the injury near the base of the finger. The flap was symmetric to the midaxial line. With the midaxial approach to the finger, the artery and nerve were meticulously dissected and separated proximally and distally to the flap. After the digital artery was ligated, this flap was raised with the artery, preserving the digital nerve with the finger. The flap was then turned 180 degrees at the pivot point 5 mm proximal to the distal interphalangeal joint to reach the fingertip defect. The donor site was resurfaced with a split-thickness skin graft harvested from the inner aspect of the arm or suture the wound directly if possible (Fig. 7).
 FIGURE 7:
FIGURE 7: Intraoperative performance. Patients treated by reverse digital artery island flaps suture of the wound directly (A–C); reverse digital artery island with a split-thickness skin graft (D, E).
Postoperative ManagementPostoperatively, antibiotics were given intravenously to reduce the risk of infection, in addition to lamp baking heat preservation and other symptomatic treatment. Moreover, patients received regular dressing changes and were advised to avoid overactivity, elevate the affected limb, stop smoking, keep warm, and regularly observe the perfusion of the skin flap.
Follow-upAt 6-month follow-up, the total active movement (TAM) and 2-point discrimination (2PD) were collected, and the subjective satisfaction of the patients regarding clinical efficacy was evaluated based on the Michigan Hand Questionnaire (MHQ). The TAM of the injured fingers was measured using a standard hand goniometer. The system sums the degrees of active flexion at the interphalangeal joints and metacarpophalangeal joint and subtracts the degrees of the extension deficits (100% for excellent, >75% for good, >50% for fair, <50% for poor). The sensibility of the palmar part of the flaps was measured using static 2PD. The modified American Society for Surgery of the Hand guidelines were used to classify the 2PD (<6 mm for excellent, 6–10 mm for good, 11–15 mm for fair, >15 mm for poor). The MHQ was used to subjectively evaluate outcomes of the repaired hands. The MHQ includes 6 subscales (overall hand function, activities of daily living, pain, work performance, aesthetics, and satisfaction).
Statistical AnalysisData analysis was performed using the SPSS 20.0 statistical software. The Kolmogorov-Smirnov test was used to identify the normality, and all data conformed to the normal distribution. Measured data were expressed as mean ± SD and the independent sample t test was used to compare 3 groups and in groups. The count data were compared by χ2 test between groups. P values less than 0.05 were considered statistically significant. Horizontal comparison of differences between same surgical groups was performed; the same letter has no difference, and different letters have differences.
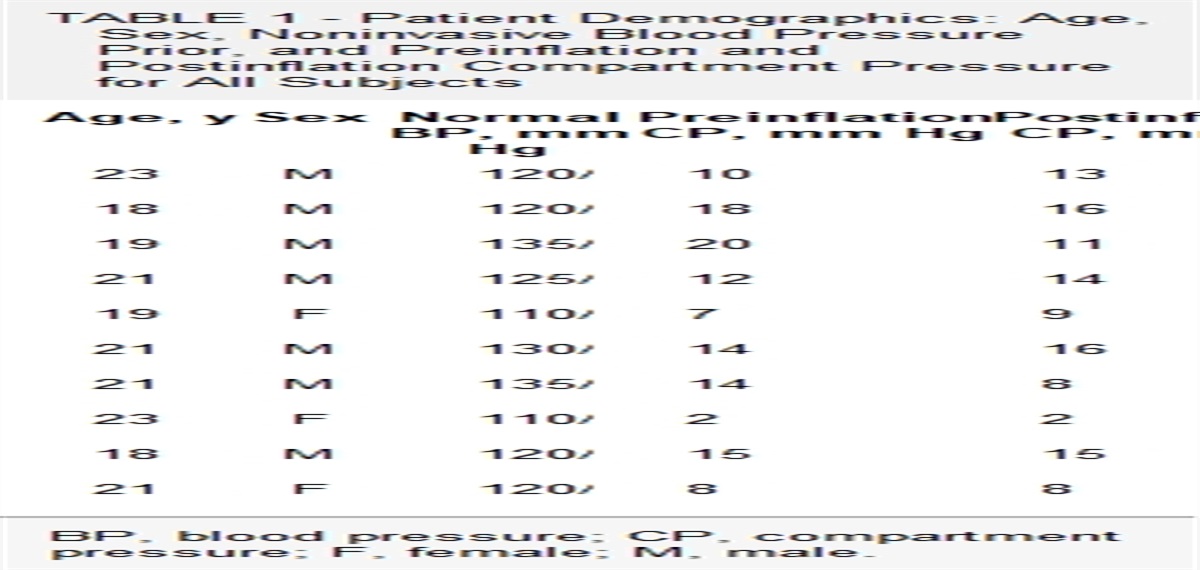
RESULTSThe characteristics of the study samples are detailed in Table 1. All the flaps and the skin grafts survived completely in 3 groups. Patients in 2 groups did not differ with respect to age, sex, the cause of injury, the finger type, the defect area, the interval between injury and surgery, and the duration of surgery (P > 0.05 for each). The operative duration of group A is shorter than group B and group C (A < B < C, P < 0.05 for each; Table 1). Accordingly, the patients' baseline assessment indicated that the 3 groups were functionally similar, and the selection bias seems to have been limited.
TABLE 1 - Characteristics of the Sample Characteristics of the Sample Group A Group B Group C Age, y 40.2 (SD, 11.3; range, 17–60)* 36.4 (SD, 9.1; range, 20–58)* 45.2 (SD, 12.1; range, 21–65)* Sex, n * * * Male 58 54 56 Female 20 33 22 Cause of injury, n * * * Twisting 26 21 19 Crushing 22 25 20 Cutting 30 32 39 Finger type, n * * * Thumb 18 16 20 Index fingers 17 19 21 Middle fingers 31 29 25 Ring fingers 8 11 10 Little fingers 4 3 2 Finger defect size, cm2 2.32 ± 0.82 (range, 1.8 × 1–2 × 1.5)* 2.41 ± 0.74 (range, 2 × 1–2.2 × 1.5)* 2.45 ± 0.66 (range, 2 × 1–2.5 × 1.5)* Interval between injury and operation, h 5.78 (range, 4.7–8.4)* 5.12 (range, 4.6–8.2)* 5.62 (range, 4.9–7.9)* Operation duration, min 31.5 ± 6.6* 95.6 ± 10.3† 125.3 ± 9.3†*Horizontal comparison of differences between same surgical group; the same letter has no difference, and different letters have differences.
†P < 0.05, statistically significant.
At the last 6-month follow-up, there was no difference with the 2PD of the palmar part of the flaps in group A and group B but better than group C (Table 2). There was no difference with the TAM of injured figures in 3 groups (Table 3). The MHQ summary scores in group A were much higher than that in group B and group C. Evaluation of the MHQ subscale performance showed that the overall hand function, activities of daily living, work performance and pain score had no differences, but aesthetics and satisfaction score was the highest in group A (A > B > C; Table 4).
TABLE 2 - Two-Point Discrimination of the Palmar Part of the Flap Value Group A* Group B* Group C* Excellent 15 12 3 Good 48 45 25 Fair 15 22 40 Poor 0 1 10*Horizontal comparison of differences between same surgical group; the same letter has no difference, and different letters have differences.
†P < 0.05, statistically significant.
Data are presented as number.
*Horizontal comparison of differences between same surgical group; the same letter has no difference, and different letters have differences.
†P < 0.05, statistically significant.
*Horizontal comparison of differences between same surgical group; the same letter has no difference, and different letters have differences.
†P < 0.05, statistically significant.
Injuries to the fingertip are common,12 which are often distal to the insertion of the flexor and extensor tendons on the distal phalanx and are treated depending on the amount of soft tissue loss and the exact level of the injury.13 In the management of a fingertip injury, although it is essential to maintain the length and preserve the nail and the appearance, the main goal of treatment is to ensure the durability of the fingertip and painless at the skin. Therefore, the treatment must be individualized based on several patient-related factors and unique trauma characteristics.14
Injuries with exposed bone and a lack of available soft tissue for coverage often require flap reconstruction if completion amputation is not desired by the patient. At present, the “V-Y” advancement flap15 is widely performed in the management of fingertip injuries. “V-Y” flap is best used for transverse or anticlinal fingertip amputation and is suitable for injury to any finger. The contraindications of applying this flap include oblique metacarpal fingertip amputation and extensive palmar soft tissue defects. The maximum distance of the skin flap is limited to 3 to 4 mm.16 The parallelogram transfer method allows a longer transfer distance of the transposition flap. In our practice, the advancement distance can achieve 6 to 10 mm. The transverse width of the flap was abandoned, and the longitudinal length of the flap was obtained. The defects were evenly distributed on each side of the parallelogram to achieve sufficient transfer distance to cover the exposed bone and tissues. The principle of antegrade homodigital island flap is advancement flap. Compared with parallelogram transfer flaps, antegrade homodigital island flap can repair a larger wound. Reverse digital artery island flaps can choose flap size freely, which can deal with various large flap defects. Therefore, the defect area repaired by retrograde flap is larger than that repaired by anterograde flap and parallelogram flap. However, our research object is transverse finger amputation with the loss of distal pulp, nails, and bone, and the defect area is relatively fixed. Parallelogram flaps and antegrade homodigital island flaps were sufficient for the operation. However, it is still necessary to use reverse digital artery island flaps for finger injury with large abdominal defect.
Antegrade homodigital island flaps are pedicled with the finger artery.10 We harvested the flap from the palmar side of the finger and pushed the flap forward to cover the wound. The flap includes a lateral proper digital artery and a digital nerve.17 The operation of reverse digital artery island flaps is more complicated and takes more time. The parallelogram flaps do not need to require stripping the artery, After a careful preoperative design of the parallelogram flap, we abandon the finger's width and retain the length, successfully achieving the purpose of the operation and reduce the operation time. In our study, the operation time was obviously shorter in the group A than that in the group B and group C.
This article provided a detailed description of a modified flap for the surgical management of fingertip defects. The transfer flap was incised closely to the bone surface of the distal phalanx, and the interphalangeal artery was not damaged during stripping,18,19 which is key to flap survival. Venous outflow is maintained by venules and capillaries in the perivascular adipose tissues through a retrograde fashion.20 Therefore, if the interphalangeal artery is well protected during the flap design, the flap survival can be assured more confidently, as evidenced in our analyses that all our parallelogram flaps had survived postoperatively.
The purpose of reconstructive surgery for fingertip injury is to obtain stable tissue coverage, achieve an acceptable appearance, restore sensitivity, maintain finger length, and resume normal physical activities in time.21 Some patients with reverse digital artery island flaps had very obvious donor site scarring and skin sinking with poor aesthetics, and they were not very satisfied with the appearance of their fingers.22 The incision of the parallelogram flap is distributed at both sides of the fingertip, and therefore, the scar is at the sides of the finger. The patients with parallelogram flaps did not complain about the appearance of the fingers, and the MHQ (appearance) scores were significantly different between the groups.
The sensory reconstruction of fingers is an important part in the hand surgery. Studies have reported that an average of 10 mm in the static 2PD test when a “senseless” reverse digital artery island flap has been performed.23,24 Conversely, other studies have demonstrated a normal static 2PD test (1–5 mm) following neurovascular island flaps.25,26 The findings of these studies indicate a reduced ability of flaps to restore sensation in the absence of nerve connections.27–29 In parallelogram flaps and antegrade homodigital island flaps, the digital nerve can usually be preserved, so 2 types of operative method both provided a good sensory reconstruction of fingers, leading to satisfactory recovery in the finger movement, strength, etc. Reverse digital artery island flaps usually does not include the digital nerve, and sensory recovery depends on the degree of peripheral nerve regeneration around the flap, so the sensory recovery of retrograde flaps is often inferior to that of parallelogram flaps and antegrade homodigital island flaps.
There is a limitation in parallelogram flaps. The palmar skin of the finger has a large defect, which cannot provide enough flipped flap. This situation is the contraindication of parallelogram flaps.
CONCLUSIONSThe reconstruction of transverse finger amputation using parallelogram flaps can achieve a shorter operation time, a more satisfying appearance. Parallelogram flaps and antegrade homodigital island flaps can both achieve a better sensory recovery. Parallelogram flaps is a better choice for reconstruction of transverse finger amputation with the loss of distal pulp, nails, and bone.
REFERENCES 1. Abbase EA, Tadjalli HE, Shenaq SM. Fingertip and nail bed injuries. Postgrad Med. 1995;98:217–236. 2. Tang JB, Elliot D, Adani R, et al. Repair and reconstruction of thumb and fingertip injuries: a global view. Clin Plast Surg. 2014;41:325–359. 3. Holm A, Zachariae L. Fingertip lesions. An evaluation of conservative treatment versus free skin grafting. Acta Orthop Scand. 1974;45:382–392. 4. Kleinman WB, Dustman JA. Preservation of function following complete degloving injuries to the hand: use of simultaneous groin flap, random abdominal flap, and partial-thickness skin graft. J Hand Surg Am. 1981;6:82–89. 5. Bevin AG, Chase RA. The management of ring avulsion injuries and associated conditions in the hand. Plast Reconstr Surg. 1963;32:391–400. 6. Giessler GA, Erdmann D, Germann G. Soft tissue coverage in devastating hand injuries. Hand Clin. 2003. 19 : 63–71, vi. 7. Buja Z, Arifi H, Hoxha E. Repair of degloving fingers with abdominal tunnelization flap. J Hand Surg Eur Vol. 2013;38:439–440. 8. Bogov A, Mullin R, Kubitskiy A. The double flap partial reconstruction technique for the avulsion-type finger injuries: a case report. J Hand Surg Eur Vol. 2011;36:423–425. 9. Silva Dos Santos TP, de Oliveira MT, Angelini LC. Retrospective study to evaluate the treatment of digital pulp lesions using a homodigital flap. Rev Bras Ortop. 2018;53:200–207. 10. Sano K, Ozeki S, Kimura K, et al. Relationship between sensory recovery and advancement distance of oblique triangular flap for fingertip reconstruction. J Hand Surg Am. 2008;33:1088–1092. 11. Evans DM, Bernardis C. A new classification for fingertip injuries. J Hand Surg Br. 2000;25:58–60. 12. Patel L. Management of simple nail bed lacerations and subungual hematomas in the emergency department. Pediatr Emerg Care. 2014;30:742–745. 13. Hawken JB, Giladi AM. Primary management of nail bed and fingertip injuries in the emergency department. Hand Clin. 2021;37:1–10. 14. Hao R, Wang B, Wang H, et al. Repair of distal thumb degloving injury using combination of reverse dorsoradial flap of the thumb and middle finger proper digital arterial island flap. J Orthop Surg Res. 2020;15:417. 15. Atasoy E, Ioakimidis E, Kasdan ML, et al. Reconstruction of the amputated fingertip with a triangular volar flap. A new surgical procedure. J Bone Joint Surg Am. 1970;52:921–926. 16. Lee DH, Mignemi ME, Crosby SN. Fingertip injuries: an update on management. J Am Acad Orthop Surg. 2013;21:756–766. 17. Lim JX, Chong AKS, Sebastin SJ. Maximal advancement of homodigital neurovascular island flaps. J Hand Surg Eur Vol. 2019;44:1008–1012. 18. Braga-Silva J, Kuyven CR, Fallopa F, et al. An anatomical study of the dorsal cutaneous branches of the digital arteries. J Hand Surg Br. 2002;27:577–579. 19. Takeishi M, Shinoda A, Sugiyama A, et al. Innervated reverse dorsal digital island flap for fingertip reconstruction. J Hand Surg Am. 2006;31:1094–1099. 20. Lucas GL. The pattern of venous drainage of the digits. J Hand Surg Am. 1984;9:448–450. 21. Germann G, Rudolf KD, Levin SL, et al. Fingertip and thumb tip wounds: changing algorithms for sensation, aesthetics, and function. J Hand Surg Am. 2017;42:274–284. 22. Chen QZ, Sun YC, Chen J, et al. Comparative study of functional and aesthetically outcomes of reverse digital artery and reverse dorsal homodigital island flaps for fingertip repair. J Hand Surg Eur Vol. 2015;40:935–943. 23. Yildirim S, Avci G, Akan M, et al. Complications of the reverse antegrade homodigital island flap in fingertip reconstruction. Ann Plast Surg. 2002;48:586–592. 24. Zhang JF, Wang L, Hao RZ, et al. Treatment of fingertip avulsion injuries using two periposition pedicled flaps. J Plast Reconstr Aesthet Surg. 2019;72:628–635. 25. Storvik HM. The extended neurovascular island flap in thum reconstruction. Scand J Plast Reconstr Surg. 1973;7:147–149. 26. Hueston J. The extended neurovascular island flap. Br J Plast Surg. 1965;18:304–305. 27. Kleinert HE, McAlister CG, MacDonald CJ, et al. A critical evaluation of cross finger flaps. J Trauma. 1974;14:756–763. 28. Johnson RK, Iverson RE. Cross-finger pedicle flaps in the hand. J Bone Joint Surg Am. 1971;53:913–919. 29. Hammouda AA, El-Khatib HA, Al-Hetmi T. Extended step-advancement flap for avulsed amputated fingertip—a new technique to preserve finger length: case series. J Hand Surg Am. 2011;36:129–134.
留言 (0)