
記住我
Understanding the etiology of depression for women living with the human immunodeficiency virus (HIV) is important for disease management. Persons living with HIV (PWH) are estimated to have two to three times greater risk of being diagnosed with major depressive disorder (MDD) compared with HIV-negative controls (1,2). Women with HIV are especially vulnerable to depression, in part, because of the chronicity of uncontrollable physiological and psychosocial stress (3–5). Compared with their male counterparts, women living with HIV are more likely to be diagnosed with MDD and report greater depressive symptom severity (6–8). Data from the Women’s Interagency HIV Study show that each additional year spent with an MDD diagnosis increases the risk of mortality by 72% (9). The clinical manifestation of depression is not solely germane to disease management in PWH. In the era of antiretroviral therapy (ART), greater depressive symptom severity was associated with a higher odds of mortality compared with those initiated on ART with minimal to no depressive symptoms (10). Certain groups of women seem to be at greater risk for depression with clinical diagnoses two to four times more likely to occur during and immediately after the menopausal transition than during premenopause (11,12). Among multiethnic samples of community-dwelling midlife women, higher ratings of depressive symptoms were most closely predicted by early postmenopausal stage and cumulative life stress (13). Much of the increase in depressive symptoms reported with the menopause transition in PWH is attributed to cardiovascular and autonomic somatic complaints (e.g., hot flash activity) (14–16). Therefore, it is essential to identify the contributing factors and interactive effects of depressive symptoms in the psychosomatic function. However, the field has yet to investigate interoceptive awareness (IA) of cardiac signals in relation to depressive symptoms among postmenopausal PWH.
Individuals with abnormal levels of interoceptive sensitivity seem to be at increased risk for psychopathology. Blunted cardiac IA is associated with depression (17,18). Behaviorally, women with major depressive disorder (MDD) have poorer interoceptive accuracy on a heartbeat counting task (19). Although behavioral studies of interoception are altogether absent in PWH, ancillary evidence in individuals with alexithymia supports interoceptive deficits in this population. Alexithymia, that is, difficulty identifying and describing feelings, has been described as a general deficit in IA and sensibility (20). In PWH, alexithymia has been linked to biomarkers of inflammation, cardiovascular disease risk, and HIV disease progression (21–25). Individuals reporting higher levels of alexithymia are shown to perform worse on heartbeat counting tasks (26–28). Moreover, mindfulness awareness training not only reduces self-reported alexithymia but also increases interoceptive accuracy during a heartbeat counting task over time (29). Given the disturbances in IA in depression and the rates of depression in HIV, the dearth of studies investigating how IA relates to depression in PWH is surprising.
Women in the perimenopausal and postmenopausal transition period are particularly affected by vasomotor symptoms. Perceptions of aberrant heart muscle contractions in the chest, including hard beats, fast beats, irregular beats, and/or pauses, increase IA, challenge self-regulation, and increase somatic symptom burden (30,31). Severity of vasomotor symptoms, including hot flashes, heart palpations, or changes in blood pressure during perimenopause and postmenopause, also predict depressive symptom severity (32,33). Indeed, strong associations are observed between severity of depressive symptoms reported in primary care patients and the extent to which bodily sensations are noticed, attended to, and trusted (34). Among women living with HIV, the menopausal transition is associated with reports of greater mood disturbance and somatic, that is, related to the body, symptom burden (35–38). In turn, frequency of symptoms and physical symptom burden consistently relate to mood disturbance and psychological distress in women living with HIV (39).
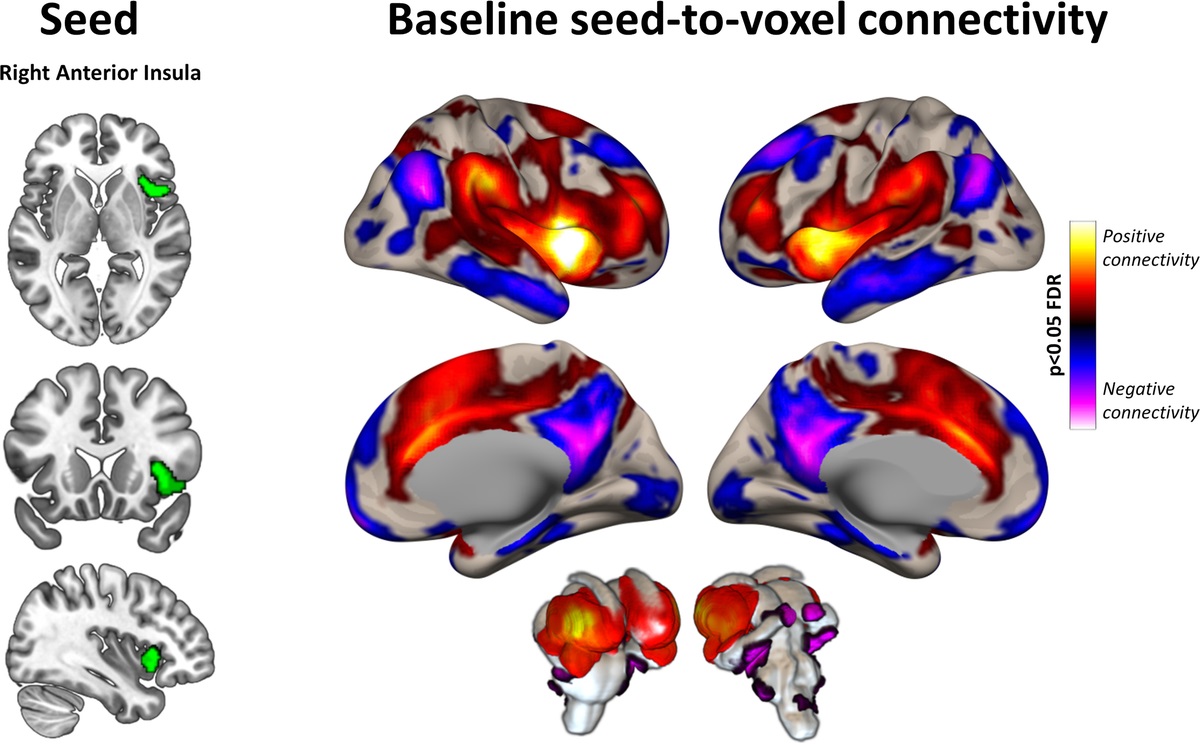
Computational models of interoception implicate prediction error in the manifestation of psychopathology. To maintain homeostasis, viscerosensory information is monitored and used to predict upcoming requirements (40,41). Interoception entails an active and iterative process of comparing the brain’s anticipation of incoming sensory information with concurrent state. When the prediction error is relatively small or nonexistent, the actual state of the body coincides with that of top-down predictions. However, when these signals are decoupled, larger prediction error and distress may emerge (18,42). The anterior insula, an important hub within the salience network, is involved in predicting afferent interoceptive stimuli (43–45). In healthy adults, functional activation of the insula is a commonly detected using cardiac interoception paradigms ranging from the counting (46–49) to attending (50–53) and discrimination of heartbeats (54). A computational model of IA has been put forth, suggesting that the anterior insula plays a critical role in the receipt of cardiac interoceptive information and in the generation of top-down predictions for moment-to-moment conscious states (55,56). This active interference model for the role of the anterior insula in depression suggests that mismatch of predicted and actual interoceptive state triggers allostatic compensatory mechanisms to restore the perceived loss of homeostasis. This increased anterior insula activity that signals detection of prediction error is thought to dampen over time, with this loss of sensitivity giving way to chronic ignoring or mislabeling of interoceptive stimuli and concomitant subsequent loss of homeostatic control (57). Indeed, compared with patients in remission and healthy controls, individuals with MDD show hyporesponsiveness of the anterior insula during a cardiac IA task suggesting a deficit in the interoceptive processing of these signals in the depressed state (58). Another study reported inverse associations between insula activity during heartbeats detection task and depressive symptom severity in persons with MDD (50). Altogether, these studies provide evidence implicating hypoactive anterior insula in the generation of predictive error from cardiac interoceptive signals.
Although no functional studies have examined IA in HIV, structural and neurochemical differences have been noted in the insula. Multiple studies have tested and confirmed that levels of HIV-1 DNA are inversely associated with insula volume in PWH (59,60). Most recently, evidence of structural alteration of the insula has been confirmed across several imaging parameters of cortical thinning, including the following: lower gray matter volume, gyrification index, and cortical thickness (61). For example, longitudinal data comparing the trajectory of whole-brain thinning in PWH versus HIV-negative controls reveal volumetric reduction of insula, tempoparietal, and cingulate regions (62). Serotonergic depletion in the insula is associated with an increased risk of depression in PWH (63–65). In addition, acute changes in serotonin can alter metacognitive insight into the reliability of judgments based on cardiac interoceptive information (66). Given the role of the anterior insula in IA and depression as well as neurobiological and psychosocial susceptibility to insula disruption and depression in PWH, a functional neuroimaging investigation of these interacting factors is warranted.
Despite the support for hypoactivation of anterior insula during cardiac IA in MDD, little is known about how this region functions in subclinical depressive states. Examining insula function in clinical populations may be confounded by behavioral and subjective aspects of depression as well as depression-related changes in insula structure, metabolism, and regional homogeneity (for a review, see Ref. (67)). Given evidence of structural alterations of the anterior insula and increased susceptibility to depression in PWH (1,2,21,59,60), the current study aimed to compare anterior insula activation to depressive symptoms as a function of HIV+ status in ethnically diverse community sample of postmenopausal women not currently diagnosed or treated for MDD. Based on a model of active interference, we hypothesize that during a cardiac IA task, persons with greater depressive symptom severity will evidence greater magnitude of blood oxygen level–dependent (BOLD) activity in the bilateral anterior insula when presented with a distracting external sound. Moreover, after adjusting for age and levels of perceived psychological stress, postmenopausal women living with HIV will evidence greater depressive symptoms as a function of bilateral insula activation.
METHODS ParticipantsThe study was conducted at the University of Miami. All recruitment procedures and consent were approved by the University of Miami Institutional Review Boards. First, participants recruited from the greater Miami–Dade County area were screened via telephone interview. Postmenopausal women, that is, women with the absence of a menstrual cycle for 12 or more consecutive months, were recruited for the study. The inclusion of postmenopausal women coincides with the primary objectives of the original study, which was to investigate the association between inflammatory-immune and endothelial cell functioning and mood disturbance in the context of vagal and estrogen withdrawal in women of postmenopausal age that are chronically infected with HIV. The rationale of exploring neurobehavioral markers of IA as a secondary analysis in this sample is based on the observation that changes in somatic symptoms of the vasomotor nature are linked to the mood disturbance postmenopause (33). Exclusion criteria included the following: a) diagnosis of a cardiovascular disease or condition, cancer, kidney/liver disease, or type 1 or type 2 diabetes; b) history of a cerebrovascular accident or loss of consciousness; c) current psychiatric medication treatment or diagnosis of psychiatric illnesses including major depressive disorder; d) current smoker; e) metal implants or debris within the body; f) current pregnancy, hormone replacement therapy, menstruation, or breastfeeding, g) positive urine toxicology screen for cocaine, amphetamines, or opioid; and h) if HIV+, had any interruption or change in prescribed antiretroviral regimen within the last 6 months, met the criteria for exclusion; however, women not currently on ARTs were not excluded, provided there was no change in this status over the last 6 months. Positive test result for tetrahydrocannabinol was not exclusionary in the current study. However, there were no positive screens for tetrahydrocannabinol in the current sample. Current diagnosis or treatment of MDD or other Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) Axis I disorders was determined using a structured clinical interview instrument, that is, the Mini International Neuropsychiatric Interview (68). Individuals meeting the criteria for current MDD were excluded from participating in the study.
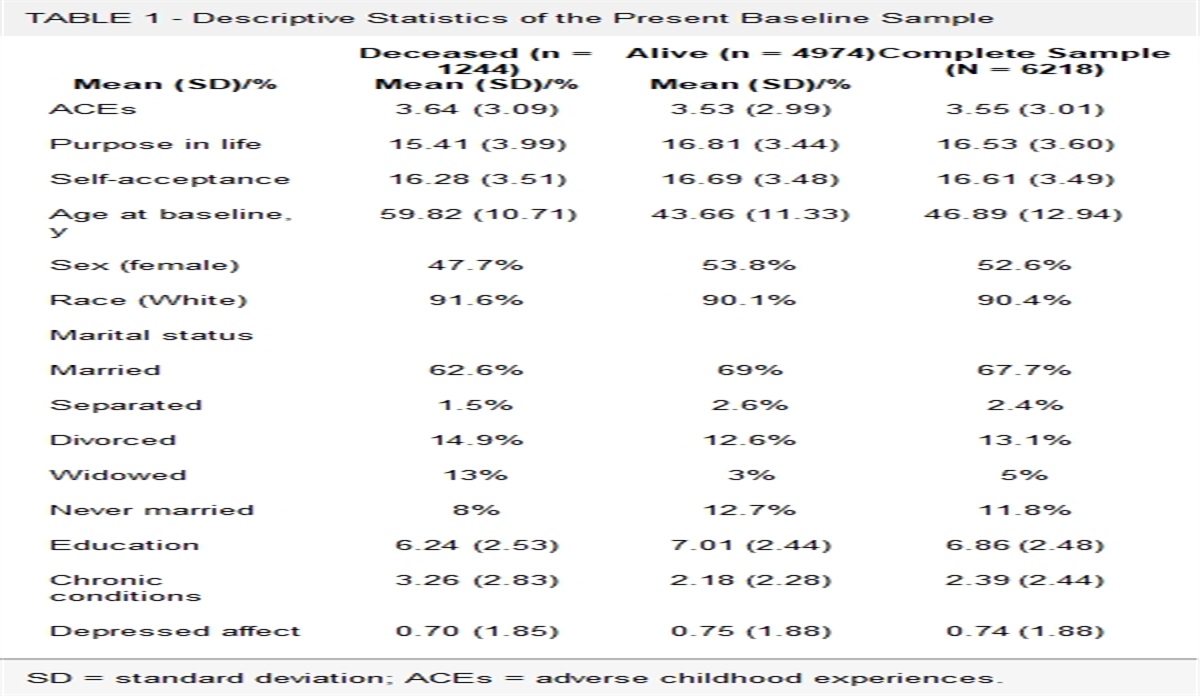
Of the 84 participants in the brain scanning portion of the study, a total of 50 participants (23 HIV+, 27 HIV-negative) completed the task and provided interpretable psychophysiological and behavioral response data (Table 1). Fifteen scans were aborted resulting in an incomplete scan sequence for one or both 7.5-minute cardiac interoception tasks. Eight participants provided insufficient behavioral response data for one or more blocks of heartbeat or tone detection trials during the IA task. Finally, the program for physiological noise correction failed for 11 participants because of excessive motion artifacts or otherwise uninterpretable photoplethysmography (PPG) signals.
HIV-Positive (n = 23), Mean (SD) or n HIV-Negative (n = 27), Mean (SD) or n Age, y 56.5 (4.82) 56.4 (8.0) Years postmenopausal 8.9 (11.3) 9.0 (10.7) Hispanic (n) 9.5 20.8 Black (n) 85.7 75.0 White (n) 4.8 4.2 BDI total score 10.5 (11.6) 12.8 (12.2) Perceived stress 19.5 (2.6) 19.3 (2.9) MAIA noticing 3.5 (1.1) 3.2 (1.3) MAIA not distracting 2.5 (1.5) 3.1 (1.1) MAIA not worrying 2.6 (0.7) 2.7 (1.0) MAIA attention regulation 2.8 (1.5) 3.1 (1.2) MAIA emotional awareness 3.6 (1.4) 3.6 (1.1) MAIA self-regulation 3.4 (1.6) 3.5 (1.2) MAIA body listening 3.2 (1.6) 2.8 (1.2) MAIA trusting 3.8 (1.5) 3.9 (1.2)SD = standard deviation; BDI = Beck Depression Inventory; MAIA = Multidimensional Assessment of Interoceptive Awareness.
Neuroimaging data were collected between October 2017 and January 2020. Participants were asked to refrain from exercise or alcoholic consumption within 24 hours before the appointment and from drinking caffeinated beverages on the morning of the scan. Laboratory studies were drawn from the HIV-positive individuals to determine CD4 count (in cells per cubic milliliters) and detectability of HIV-1 RNA. HIV-1 viral load was determined using an in vitro nucleic acid amplification test (AMPLICOR HIV-1 Monitor Test; Roche Diagnostics, Branchburg, New Jersey) with ultrasensitive methods (range, 50–750,000 HIV-1 RNA copies/ml) and repeated with standard methods to determine if viral load met the upper detection limit (range of 400 copies/ml to 10 million copies/ml). Date of HIV diagnosis, current ART regimen, and length of duration of ART treatment at the time of the questionnaire were collected (Table 2).
TABLE 2 - HIV+ Group Disease Characteristics Mean (SD) or n Years with HIV 18.3 (9.4) Years on antiretrovirals 11.34 (10.5) On cART (n) 82.1 NRTI 0 NNRTI 28.6 PI 19.0 NtRTIs 9.5 INIs 25.0 Fusion inhibitors 0 Undetectable viral load (n) 66.7SD = standard deviation; cART = combination antiretroviral therapy; NRTIs = Nucleoside reverse transcriptase inhibitors; NNRTIs = Non-nucleoside reverse transcriptase inhibitors; PIs = Protease Inhibitors; NtRTIs = Nucleotide reverse transcriptase inhibitors; INIs = HIV Integrase Inhibitors.
An IA paradigm was adopted from Zaki and colleagues (54) wherein participants were instructed to monitor and respond to cardiac interoceptive (i.e., heartbeat) stimuli in the presence or absence of an auditory exteroceptive (i.e., tone) stimuli or simply monitor and detect the auditory tones. During the heartbeat monitoring with tone condition (HT), participants were instructed to make a response each time they felt their heartbeat while ignoring tones. During the heartbeat monitoring condition (H), participants were instructed to make a button press response, as quickly as possible, each time they felt their heartbeat in the absence of tones. During the tone monitoring condition (T), participants were prompted to make a button press each time they heard a tone.
During the practice session, each participant’s resting heart rate was determined so that tones could be presented at that participant’s heart rate, Hr ± 25% random variance to simulate the natural variability in resting heart rate. For example, if a given participants’ resting heart rate was 60 beats/min, they would hear one tone every 1.00 ± 0.25 seconds.
Each task was presented in six 30-second blocks across two 7.5-minute functional runs. Participants were prompted to respond to visual and auditory prompts before the beginning of each of the cardiac IA blocks. Using an LCD Hyperion Magnetic Resonance Imaging (MRI) Digital Projection System, instructions were presented on a black background using white writing and viewed through a mirror mounted on the head coil. Each block was preceded by a 2-second visual presentation of the phrase “rate heart beat” or “rate tones,” indicating which task they should perform during that block. Blocks were separated by a fixation cross, presented for 3 ± 1 s. Biopac physiological recording systems were used to collect heart rate using a PPG and respiration rate using a respiratory transducer.
A standard protocol was implemented to familiarize study participants with the cardiac IA task and the MRI environment (e.g., scanner noises associated with the different pulse sequences) using a mock scanner outside of the MRI suite. Before entering the MRI environment, participants were provided noise canceling headphones (Avotec, Inc.; Silent Scan SS-3300 Hearing Protection, Communication and Music System) to attenuate scanner noise during the practice (mock MRI) and real MRI sessions. All participants further underwent a verbal and tone auditory check before engaging in the heartbeat detection task while in the scanner.
Measures DepressionSymptoms of depressive symptoms were assessed using the Beck Depression Inventory II (69). The Beck Depression Inventory II is a clinically robust 21-item self-report questionnaire. Individuals’ items are rated on a 4-point scale indicating degree of severity, with items rated between 0 (not at all) and 3 (extreme form of symptom). Although not intended for diagnostic purposes, the following cutoffs are recommended for determining symptom severity: minimal = 0–13, mild = 14–19, moderate = 20–28, and severe = 29–63. This measure demonstrated good internal consistency (α = .84).
StressSeverity of psychological stress was assessed using the 14-item Perceived Stress Scale (PSS) (70). The scale measured how often individuals appraised situations in their lives as being stressful on a scale of 0 (never) to 4 (very often). Positive items were reverse scored, and items were summed to create a total PSS score. This measure demonstrated good internal consistency (α = .81).
Multisource Interoceptive Awareness QuestionnaireThe Multidimensional Assessment of Interoceptive Awareness (MAIA) is a 32-item self-report of IA (71). Five dimensions: a) awareness of comfortable, uncomfortable, and neutral body sensations; b) attitude of body awareness; c) quality of attention to somatic sensation; d) mind-body integration; and e) not distracting or worrying are measured by a eight subscales, including noticing, not distracting, not worrying, attention regulation, emotional awareness, self-regulation, body listening, and trusting (71). As an exploratory aim, the bivariate correlation of each of these subscales with the study variables was analyzed to determine whether the self-report indices of IA correspond to behavioral markers of interoception in relation to the other study variables. Subscales of the MAIA show good internal consistency with Cronbach α values ranging from α = .66 to α = .87.
BehavioralDuring the H and HT conditions, individuals pressed the button when detecting their heartbeat. Accurate responses were recorded if the button press occurred within the biological response time allowable within the interbeat interval (≥120 milliseconds). Hit rate for each block of the H and HT conditions was calculated as number of accurate button presses divided by the total number of heartbeats detected by PPG signal. Response latency was determined by taking the time of the registered PPG signal and subtracting the time of the subsequent button press.
To test the null hypothesis that the hit rate and response latency did not vary across the H, HT, and T conditions, a repeated-measures analysis of variance was performed. Violations in the Mauchly test for sphericity necessitated Greenhouse-Geisser correction.
PhotoplethysmographyPPG uses a transducer to measure total hemoglobin content in the superficial vasculature of the skin. The amplitude of the PPG signal reflects blood volume and its pulsatile variations with the cardiac cycle (72). PPG signals were sampled at 1000 Hz using a Biopac’s AcqKnowledge software connected to the MP 150 digitizer system and PPG100C-MRI transducer attached to the participant’s left index finger and (Biopac Systems Inc., Goleta, California). The PPG signal was synchronized to the MRI scanner trigger.
MRI AcquisitionMRI was performed on a GE MR750 3.0T MR scanner and 32-channel head coil capable of performing functional and structural scans in humans. In two 7.5-minute blocks, functional T2*-weighted echo planar images with BOLD contrast were acquired parallel to the AC-PC plane in bottom-up interleaved order using the following settings: 24 slices per volume; slice thickness, 3 mm; field of view, 240 mm2, matrix, 96 × 96; spatial resolution, 2.5 × 2.5 × 3 mm3; echo time, 25 milliseconds; repetition time, 2000 milliseconds; and flip angle, 50degrees. The initial five nonequilibrium volumes of each functional run were discarded from further analyses. High-resolution T1-weighted anatomical images were also acquired for everyone using a magnetization-prepared rapid gradient echo sequence (thickness, 1 mm; field of view, 256 mm2; matrix, 256 × 256; repetition time, 9.2 milliseconds; echo time, = 3.7 milliseconds; flip angle, 12 degrees). Before analysis, MRI data were visually inspected for warping, head coverage, blurring, and signal artifacts (including ringing, striping, ghosting, or signal loss; see http://fcon_1000.projects.nitrc.org/indi/enhanced/qc.html).
Functional MRI Preprocessing and Single-Individual AnalysisBefore functional MRI analysis, the RETROICOR program was used for physiological noise correction to minimize global changes in BOLD signal within the brain because of low-frequency fluctuations in cardiac rate (73,74). This step was intended to enhance the signal of conscious cardiac processing and reduce the noise associated with afferent signaling of heart rate. Cardiac noise correction involved first removing the time-locked cardiac artifacts and then removing the low-frequency respiratory cardiac effects using methods previously described by Chang and Glover (74). Specifically, the heart rate time series was calculated as the inverse of the average interbeat interval using a 6-second sliding window. This time series was then convolved with the cardiac response function, and the resulting waveform is simultaneously regressed out of each voxel’s time series using multiple regression.
The fMRI data were preprocessed using the Analysis of Functional NeuroImages (AFNI) software package (75), version AFNI_17.3.00. DICOM images were reconstructed into AFNI’s *.BRIK format. Processing steps were generated with afni_proc.py. We used the following blocks: despike, tshift (default), align, tlrc, volreg (default), blur (default), and regress (default). Frames were first despiked and slice-timing corrected. All the functional images of each run were realigned to the third functional image of that run. During the volume registration step, six motion parameters (roll, pitch, yaw, dS, dL, dP) were derived and demeaned, and derivatives were specified. These parameters were included in the regression. Functional images were coregistered to the structural image. Echoplanar images were normalized to a high-resolution Montreal Neurological Institute (MNI-152) atlas template followed by manual inspection to confirm successful alignment. Outliers were generated for the volume-registered data set based on whether a given time point greatly exceeded the mean number of voxel outliers for the time series and were subsequentially removed using the regress_censor_motion function. A Gaussian filter (4-mm full-width half-maximum) was used for spatial blurring. A mask was created using the 3dAutomask algorithms. Voxels were resampled into 2.5-mm isotropic space. The .BRIK files were converted to NIFTI using the AFNI 3dAFNItoNIFTI command so that these outputs could be used for second-level exploratory analyses in SPM-12.
First-level design matrices for each participant were estimated within the general linear model using AFNI. Events were modeled by a standard hemodynamic response function. The onset times were documented for each of the task conditions, which included the cued events (HT, H, T). Only responses recorded within 2 seconds of the trials were included. Using the 3dDeconvolve function, the impulse response function was first estimated and convolved with the stimulus time series to yield the estimated results. A generalized additive model regression was selected for the basis function because this model is more robust to stimuli that is brief (<2 seconds) and of relatively same length, that is, tone and heartbeat. The β weights derived from this approach represent the peak height of a generalized additive model curve (approximately 12 seconds) found in the data (Cox, 1996). Effects for condition (HT, H, T) relative to baseline were computed using previously demeaned, cardiac noise-reduced, and normalized time series data for each voxel of the bilateral anterior insula. We focused on the contrast (H − HT) to best approximate activity germane to the discrimination of cardiac interoceptive information because each of the conditions in this contrast has interoceptive components. As outlined by Zaki and colleagues (54), examining this contrast provides a conservative estimate of anterior insula activity related to interoceptive attention when there is a need to filter out external distracters.
Regions of Interestβ Estimates of BOLD activity associated with button response during the HT, H, and T conditions relative to baseline were extracted from the anterior insula. The left and right anterior insula masks were adopted from a previous study implicating these structures as a key hub in the integration of afferent and efferent cardioautonomic signals (76). In that study, the anterior insula region of interest (ROI) was manually drawn by trained investigators on MRIcron using a high-resolution T1 MNI template (ch2better.nii; http://www.mccauslandcenter.sc.edu/mricro/mricron/stats.html). The total volume of both ROIs was 15,664 mm3. The center of mass for the left anterior insula ROI was at MNI x = 39.3 mm, y = 16.1 mm, and z = −0.8 mm, whereas the right anterior insula ROI was at MNI x = −35.3 mm, y = 16.6 mm, z = 0.3 mm.
Statistical AnalysisData screening included calculating descriptive statistics, intercorrelations between study variables, and variable distributions, and evaluating normality. No log transformations were required for variables departing from normality. Bivariate correlations were evaluated (two-tailed) and included primary and secondary (MAIA) study variables (Table 3). β Weights indicating BOLD activity to the H − HT contrast were extracted from left and right anterior insula ROIs were entered into two separate regression models, as independent variables, characterizing the main effect for activity in those ROIs on the dependent variable depressive symptoms. Controlling for the covariates of age and perceived level of psychological stress each model first tested the additive and then the interactive effect for the independent variables of HIV+ serostatus and BOLD activation to the H − HT contrast for both left and right anterior insula. To assess the statistical significance of the left and right insula models of cardiac IA, a Bonferroni correction of α = .025 (e.g., α = .05/2) was applied to each regression model. All analyses were conducted in SPSS version 27 (IBM Corp. Released 2020. IBM SPSS Statistics for Macintosh, Version 27.0; IBM Corp., Armonk, New York).
TABLE 3 - Bivariate Associations Between Study Variables (Two-Tailed) Variable 2 3 4 5 6 7 8 9 10 11 12 13 14 15 1 Age −0.18 −0.24 0.11 0.13 −0.06 0.18 −0.04 0.17 0.02 −0.05 0.07 0.21 −0.08 −0.08 2 PSS 0.36** 0.04 0.08 0.29* −0.19 −0.01 0.02 0.30* 0.10 0.05 −0.02 −0.09 −0.19 3 BDI-II 0.29* 0.31* 0.12 −0.57 −0.29* 0.01 0.17 0.03 0.01 −0.01 0.37** 0.29* 4 BOLD left aI 0.95** 0.21 −0.17 −0.26 0.26 0.33* 0.33* 0.30* 0.47** 0.12 0.23 5 BOLD right aI 0.14 −0.19 −0.29* 0.16 0.25 0.024 0.22 0.42** 0.09 0.27 6 MAIA noticing −0.23 −0.02 0.54** 0.68** 0.63** 0.51** 0.33* −0.21 −0.20 7 MAIA not distracting 0.41** −0.29* −0.31* −0.12 −0.24 −0.04 −0.15 −0.24 8 MAIA not worrying 0.03 0.08 0.10 0.03 −0.05 0.11 −0.25 9 MAIA attention Regulation 0.71** 0.68** 0.77** 0.41** 0.11 −0.13 10 MAIA emotional awareness 0.71** 0.63** 0.53** 0.01 −0.12 11 MAIA self-regulation 0.74** 0.49** −0.01 −0.25 12 MAIA body listening 0.53** 0.05 −0.16 13 MAIA trusting 0.09 −0.03 14 MAIA disability 0.44** 15 MAIA pain scalePSS = Perceived Stress Scale; BDI = BDI-II = Beck Depression Inventory II; BOLD = blood oxygen level dependent; Multidimensional Assessment of Interoceptive Awareness; aI = anterior insula.
* .05 level (two-tailed).
** .01 level (two-tailed).
As shown in Figure 1, the main effect for condition type on response hit rate was significant (F(2,96) = 88.87, p < .001, ηp2 = 0.649). Participants detected a lower number of heartbeats without the tone (H mean = 35.3%) as compared with the tone distractor (HT mean = 65.5%) or just the tone by itself (T mean = 75.4; p values < .001). There was also a statistical difference between H and HT conditions (p < .001). However, there was no effect for HIV group status on hit rate accuracy across tasks (F(1,48) = 0.420, p > .05). The condition by HIV serostatus interaction was also significant (F(2,96) = 5.37, p = .01, ηp2 = 0.101). In the tone condition, HIV+ participants also showed lower hit rates (mean = 68.4%) compared with HIV-negative women (mean = 82.4%; F(1,48) = 5.632, p = .022). However, this interactive effect was not observed for the H (F(1,48) = 0.808, p = .373) and HT conditions (F(1,48) = 0.165, p > .05).
 FIGURE 1:
FIGURE 1: Comparison between HIV+ and HIV-negative controls of the mean hit rate during each of the interoceptive task conditions. CI = confidence interval.
As a key node within the salience network, during interocept
留言 (0)