
記住我
Suicide is a serious global public health problem. The World Health Organization (WHO) reported that approximately 800,000 people worldwide die from suicide every year (an average of one death every 40 seconds) (1). The incidence of suicidal behavior of people living with human immunodeficiency virus (PLHIV) is three times higher than that of the general population (2). Furthermore, suicide mortality rates among PLHIV have continued to increase annually from 0.15 per 100 person-years (PY) in 1988 to 2008 to 0.47 per 100 PY in 2011 to 2012, whereas deaths from suicide have increased threefold (3,4). However, these data are derived from official registries and death certificate information (e.g., the Human Cause of Death Database and records on suicide hospitalizations) and do not include details of risk factors, suicidal ideation, and suicide attempts (4–7). Therefore, these aspects should be explored using scientific research.
Studies have found that poor social support, stigma associated with PLHIV, and associated comorbidities may influence the increase in suicide rates (8–11). A study conducted in Taiwan found that, because of stigma and a lack of social care or support, suicide is the second leading cause of death among PLHIV in Taiwan (12). As such, suicide has become a major health issue among PLHIV in the era of antiretroviral therapy (ART). A study conducted in the pre–highly active ART (pre-HAART; 1988–1995) and HAART (1996–2008) eras reported that the suicide rate was lower at those times than in the modern ART era (2005–2014). However, the relationship between antiviral therapy and suicidal behaviors remained unclear in the modern ART era (4,13–17). Despite this, to our knowledge, no studies have referenced previous studies and reported the global prevalence of suicidal behavior and associated risk factors among PLHIV.
Suicidal behavior is a complicated process with varying degrees of severity, from suicidal ideations to suicide attempts and ultimately death by suicide. Suicidal ideation is defined as thinking about, considering, or planning suicide, whereas a suicide attempt is defined as a failed attempt to commit suicide wherein the person survives (18,19). Death by suicide represents the extreme end of the spectrum; it is a complex interrelationship between behavior and suicide attempts that end in death (18,20).
There is a lack of studies evaluating the global suicidal behavior of PLHIV. Some studies in developing countries and settings have reported and a possibly high prevalence of suicidal behavior (2,20–22). Some have shown that suicidal ideation is more common than suicide attempts and suicide, and that the presence of suicidal ideation influences the high risk of suicide attempts and completion (20,23). Three methods used to commit suicide across countries/regions, races, social statuses, and risk factors have been investigated, whereas several primary studies (24–27) focused on specific at-risk populations (e.g., postpartum women, men who have sex with men, and prisoners). However, no studies have systematically included all at-risk populations and risk behaviors, and no systematic review studies have been conducted using primary research data from multiple countries.
Therefore, this systematic review and meta-analysis was conducted to determine the global prevalence of suicidal ideation, suicide attempts, and suicides, as well as the associated risk factors among PLHIV.
Objective of This StudyThe aim of this study was to estimate the global prevalence and risk factors associated with suicidal ideation, suicide attempts, and suicides among PLHIV.
Research QuestionWhat is the global prevalence of, and what are the risk factors associated with, suicidal ideation, suicide attempts, and suicides among PLHIV?
METHODS Search StrategyThis study came from five databases (Embase, MEDLINE, CINAHL, Scopus, and Web of Science) searched for studies on the prevalence of suicidal behavior among PLHIV published between January 1, 2010, and October 31, 2021. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed (28–30). English synonyms such as AIDS, T-lymphotropic virus, human T-cell lymphotropic virus, type III human T-cell leukemia virus, type III lymphadenopathy-associated virus, LAV-HTLV-III, HTLV-III-LAV, type III infection, and HTLV III infection were used to search each database. We also used several control phrases for the Emtree and MeSH databases. For Emtree, they included “human immunodeficiency virus,” “human immunodeficiency virus infection,” “suicidal behavior,” “automutilation,” and “suicide.” For MeSH, they included “HIV infections,” “HIV,” and “self-injurious behavior.” We supplemented the search results with the Endnote X9 bibliographical database. Publications that cited the articles identified during the search were manually screened, as well as the reference lists of relevant articles and previous systematic reviews to confirm the sensitivity of the search strategy (31).
Eligibility CriteriaThe inclusion criteria were as follows: a) the study provided primary data on the prevalence or incidence of suicidal ideation, suicide attempts, or suicides measured using validated assessment tools or coded medical report data within a population-based study; b) the participants were 15 years or older; c) the participants were diagnosed with human immunodeficiency virus (HIV)/AIDS; and d) observational studies (including cohort and cross-sectional studies) published in English, Chinese, or Sinhala, and published from 2010 to 2021 (the modern ART era within recent 10-year publications). The following types of studies were excluded: those in which the study population did not include PLHIV, and qualitative research and review studies.
Titles and abstracts were independently screened by three researchers based on the inclusion and exclusion criteria after removing duplicates using the Endnote X9 bibliographical database. Then, the full text of the selected studies was reviewed by three researchers independently, with any disagreement resolved by a fourth researcher to avoid selection bias.
Quality AssessmentAll eligible studies were assessed for quality of evidence using the Joanna Briggs Institute Critical Appraisal for Checklist for Prevalence Studies Scale, which contains nine items and four responses (yes, no, unclear, and not applicable) (32). Studies with a total score of 8 and higher were considered to have high-quality evidence and were included in this systematic review. Study quality and risk of bias were independently assessed by three researchers, with any disagreement resolved by a fourth researcher.
Data ExtractionThe following data were extracted: names of authors, year of publication, country, settings, study design, sample size, and participant ethnicity, age, sex, prevalence of suicidal ideation, suicide attempts, and suicides. Three authors independently assigned quality scores for the included studies according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (28), and any disagreements were resolved via a discussion among all four authors.
Statistical AnalysisA meta-analysis was conducted to identify statistical outcomes for three selected suicidal behaviors among PLHIV using the eligible studies. The pooled prevalence of either suicidal ideation, suicide attempt, or suicide was analyzed using number of events converted to the risk ratio (RR) of 95% confidence interval (CI) and p value and based on a fitted model based on the degree of heterogeneity. The random-effects model or a fixed-effects model was used based on the heterogeneity results for suicidal behavior among PLHIV. We transformed the proportions with the Freeman-Tukey double arcsine method before pooling the data for incident rate of suicide, and the heterogeneity value was assessed using DerSimonian-Laird estimator by I2, the Cochran Q test, and τ2 for the included studies (33–37). A value of zero indicated the absence of heterogeneity, 25% indicated no significance or low significance, 50% indicated moderate heterogeneity, and 75% indicated significant heterogeneity. In the present study, 75% to 100% indicated significant heterogeneity, where the Q statistic and p value were used to validate the heterogeneity results. In this meta-analysis, I2 > 75% and p > .05 indicated statistical significance.
Publication bias was determined using funnel plots, and Q statistic for Egger’s was used to determine the correlation between the effect estimate and the variances in the results for suicidal behavior among PLHIV via Comprehensive Meta-Analysis Software (Biostat, Englewood, New Jersey) and a visual examination of the funnel plots (38,39). A subgroup analysis and a meta-regression were performed to investigate potential sources of heterogeneity. For the meta-regression, we used the pool of effects size data as a single coverable that was introduced individually into the models. A simultaneous test was conducted to determine if all coefficients were zero in the model test. We used a null hypothesis model for the effect size comparison. Statistical analyses were conducted using Comprehensive Meta-Analysis Software version 3.0 (Biostat) (40).
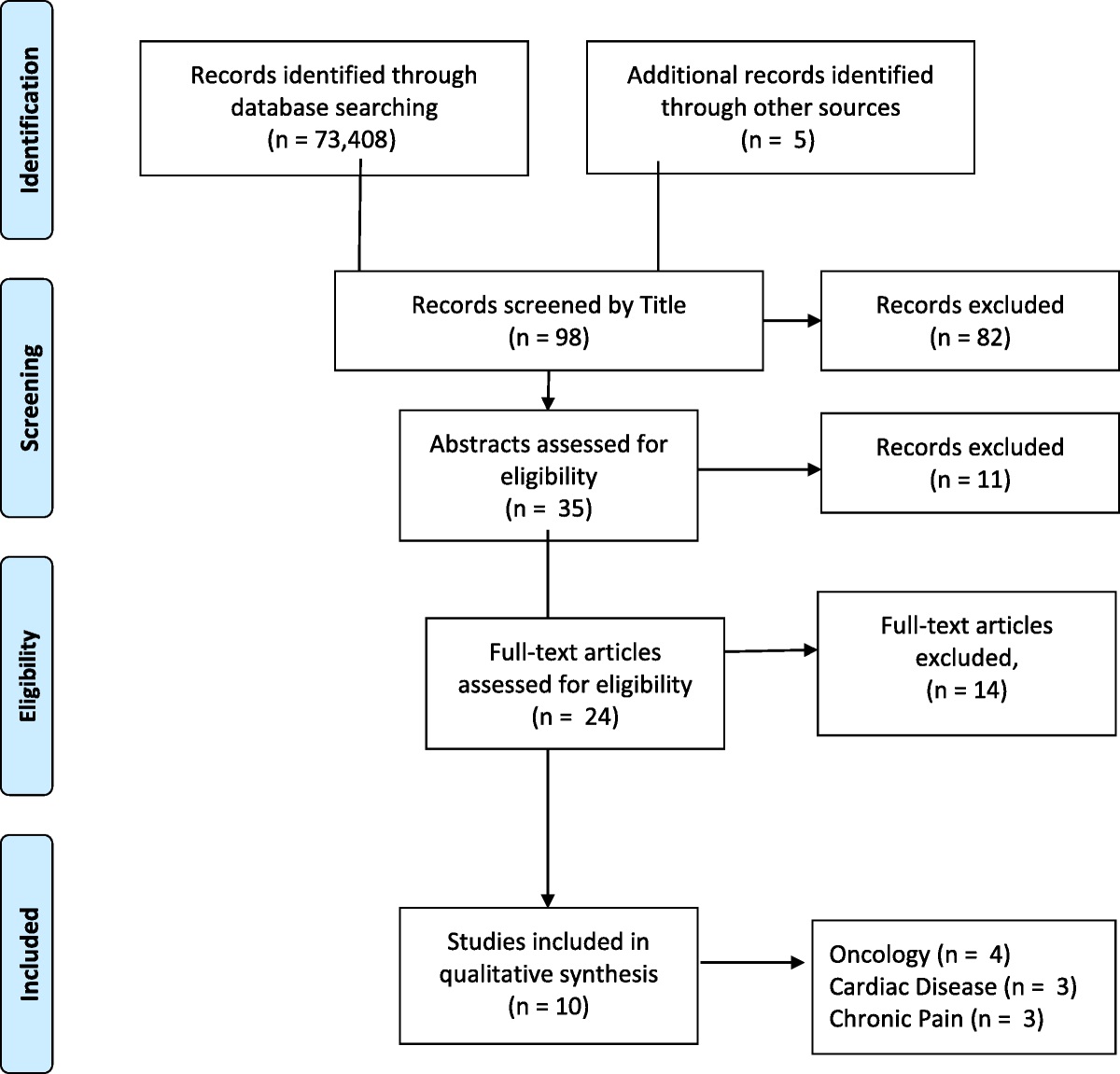
RESULTS Study IdentificationSearching the five databases resulted in 4199 articles being identified that were published between January 1, 2010, and October 31, 2021. After removing 843 duplicate articles using the Endnote X9 bibliographical database, the titles and abstracts of 3356 articles were screened, and 1854 articles met the inclusion criteria. The full text of each article was read to determine eligibility, and 1784 articles were excluded for the following reasons: 1166 articles did not have any relationship to HIV/AIDS, 488 articles did not mention suicidal behavior among PLHIV, 99 articles did not clearly assess the outcome variables, and 31 articles were not available in a full-text format. After the quality assessment, 27 articles were removed because of a low-quality score in the peer review. Thus, 43 articles were included in the systematic review and meta-regression (Figure 1). Studies with quality scores of 8 and higher were accepted as high quality (Supplemental Digital Content, Table S1, https://links.lww.com/PSYMED/A865).
 FIGURE 1:
FIGURE 1: PRISMA flow diagram of the included studies. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; JBI = Joanna Briggs Institute; HIV = human immunodeficiency virus.
Study CharacteristicsThe characteristics of the 43 studies included in this work are shown in Table 1. Studies were conducted in 21 countries (Argentina, Brazil, Canada, China, Estonia, Ethiopian, France, Indonesia, Iran, Japan, Kazakhstan, Korea, Lesotho, Nigeria, South Africa, Spain, Switzerland, Taiwan, Tanzania, Uganda, and the United States). Of all the included studies, seven were conducted in China (8,20,26,41,43,52,54), five were conducted in South Africa (11,24,25,45,63), four were conducted in Ethiopia (42,44,47,50), four were conducted in the United States (23,31,51,60), three were conducted in Nigeria (9,58,59), and two were conducted in Switzerland (4,6), France (33,57), Canada (3,13), and Brazil (10,64) Single studies were conducted in each of the other countries. Regarding the study design, 33 were cross-sectional studies, 9 were cohort studies, and 1 was a retrospective study. In terms of the study setting, 18 studies were conducted in a hospital, another 19 studies had participants recruited from HIV clinics/community centers, and 6 studies used national data from a database. The studies were published between 2010 and 2021, with 32 studies published in the past 5 years (2015 and later) and the remaining 11 studies published before 2015 (Table 1).
TABLE 1 - Characteristics of the Selected Studies Author, Country
留言 (0)