
記住我







Respiratory virus infection can cause severe illnesses capable of inducing acute respiratory failure that can progress rapidly to acute respiratory distress syndrome (ARDS). ARDS is related to poor outcomes, especially in individuals with a higher risk of infection, such as the elderly and those with comorbidities, i.e. obesity, asthma, diabetes mellitus and chronic respiratory or cardiovascular disease. Despite this, effective antiviral treatments available for severe viral lung infections are scarce. The coronavirus disease 2019 (COVID-19) pandemic demonstrated that there is also a need to understand the role of airborne transmission of respiratory viruses. Robust evidence supporting this exists, but better comprehension could help implement adequate measures to mitigate respiratory viral infections. In severe viral lung infections, early diagnosis, risk stratification and prognosis are essential in managing patients. Biomarkers can provide reliable, timely and accessible information possibly helpful for clinicians in managing severe lung viral infections. Although respiratory viruses highly impact global health, more research is needed to improve care and prognosis of severe lung viral infections. In this review, we discuss the epidemiology, diagnosis, clinical characteristics, management and prognosis of patients with severe infections due to respiratory viruses.
AbstractRespiratory viruses can cause severe disease with poor outcomes, especially in individuals with a higher risk of infection. Early identification, epidemiological tracing, and preventative and therapeutic measures are crucial to limiting their spread. https://bit.ly/3mpuFat
IntroductionIn April 2022, the World Health Organisation (WHO) reported almost 504 million coronavirus disease 2019 (COVID-19) cases, more than 6.2 million COVID-19-related deaths and more than 11.3 billion vaccine doses administered globally [1].
The clinical severity of COVID-19 infection ranges widely, from asymptomatic or mild disease of the upper airways to pneumonia and acute respiratory distress syndrome (ARDS) (figure 1). Several studies have described cases as being 70% mild, 20% severe and 10% critically ill [4–6]. For patients treated in intensive care units (ICUs), mortality falls between 40–50% and is higher in patients with ARDS [7, 8]. However, this clinical picture changed as different waves of COVID-19 took place. Patients who were elderly, fragile or with chronic comorbidities comprised the population most affected in the first and second waves worldwide [9, 10]. In the subsequent waves, a surge of COVID-19 cases was more prevalent in younger unvaccinated adults [11, 12]. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic showed us how respiratory viruses affect individuals and continue to be underestimated, even though lower respiratory viral infections (LRVIs) are a significant cause of morbidity and mortality. The pandemic also highlighted the advances made in molecular diagnosis techniques that facilitated early identification in SARS-CoV-2 infection.
 FIGURE 1
FIGURE 1 Coronavirus disease 2019 (COVID-19) spectrum. COVID-19 has various clinical manifestations, with the spectrum of the disease ranging from asymptomatic to critical illness. Managing patients with COVID-19 will depend on disease severity. Patients with risk factors for severe disease and those with moderate disease should be monitored closely. The presence of respiratory rate ≥30 breaths per minute, oxygen saturation <94%; arterial oxygen tension (PaO2)/inspiratory oxygen fraction (FIO2) <300 mmHg and lung infiltrates >50% are indicators of severe disease. Critical illness is related to respiratory failure, septic shock and/or multiple organ dysfunction. Viral replication is higher before or soon after symptom onset. Inflammation presents later in the disease. SpO2: oxygen saturation measured by pulse oximetry, peripheral oxygen saturation. Information from [2, 3, 132].
This review focuses on the primary viruses responsible for severe respiratory infections. We summarise their role and importance in global health.
The impact of LRVIsInfluenza A virus, influenza B virus, respiratory syncytial virus (RSV), rhinovirus, adenovirus and parainfluenza virus are the most frequent respiratory viruses that cause acute LRVI [13–21]. However, progress in molecular diagnostic techniques has facilitated the identification of other viruses like metapneumoviruses, bocavirus and coronaviruses, with a reported rise occurring in the general population [5, 22–24]. Importantly, in immunocompromised individuals, viruses such as cytomegalovirus, herpes simplex virus or varicella zoster virus constitute the pathogens often responsible for LRVI [25–29].
Approximately 11.5% of all lower respiratory tract infection (LRTI) episodes occurring in 2017 were attributable to the influenza virus This corresponds to about 54 million episodes, including 9.4 million hospitalisations [30]. Also, influenza LRTI was reported as being responsible for an estimated 145 000 (95% confidence interval (CI) 99 000–200 000) deaths among all ages that year. Adults aged >70 years have the highest mortality rate (16.4 deaths per 100 000 (95% CI 11.6–21.9)).
In the case of RSV, 2015 data from industrialised countries showed that about 1.5 million episodes of RSV-causing acute respiratory infections (ARI) occurred in older adults (aged ≥65 years). This study also reported that approximately 14% of the population needed hospitalisation and an estimated 14 000 persons died due to RSV-ARI [31]. Interestingly, a recent systematic review and meta-analysis in industrialised countries reported the annual incidence of RSV-ARI in adults with any comorbidity as 37.6 per 1000 person per year [32]. In the case of children aged <5 years, 33 million RSV-ARI episodes were reported to result in 3.2 million hospital admissions and 59 000 in-hospital deaths [33].
Recently, a prospective European primary care study evaluated 2957 adults presenting acute cough and/or suspected LRTI. A polymerase chain reaction (PCR) test was performed to test six respiratory viruses. The study authors reported that testing was positive in 46% (n=1354) of patients, with rhinovirus (40%; n=537) being the most frequently detected virus, followed by influenza viruses (20%; n=276) and coronavirus (13%; n=174) [34].
Respiratory viruses are also involved in causing chronic obstructive pulmonary disease (COPD) exacerbations. Several studies have reported that 50% of COPD exacerbations are due to respiratory viruses. For instance, in a systematic review that included 19 studies where PCR was used in sputum samples of 1728 patients with COPD exacerbations, the authors reported that rhinovirus/enterovirus (16%), RSV (10%) and influenza viruses (8%) were the most frequent viruses, whereas adenovirus (2%), human metapneumovirus (3%) and bocavirus (0.56%) constituted a rare cause of such exacerbations [35]. Furthermore, a recently published retrospective study of 262 cases of severe COPD exacerbations showed that a respiratory virus was detected in 41% of cases, with rhinovirus/enterovirus (27.5%), influenza virus (23%), RSV (13%), parainfluenza virus (13%) and coronavirus (13%) being the most frequently detected viruses. The authors reported that patients with viral exacerbations faced higher severity [36].
In the case of pneumonia, respiratory viruses comprise 10–20% of adult community-acquired pneumonia (CAP) cases with an established microbiologic diagnosis [37–40]. Respiratory viruses are identifiable in 15–45% of severe CAP cases [21, 41–45]. With respect to hospital-acquired pneumonia (HAP), respiratory viruses account for 10–30% of cases in adults [46, 47]. A retrospective case-control study by Micek et al. [48] including 174 nonventilated (NV) HAP cases and 696 controls reported a prevalence rate of 24% of respiratory viruses in NV-HAP. Similarly, a secondary analysis of a prospective cohort by Shorr et al. [49] detected respiratory viruses in 22% of patients with NV-HAP. In order of frequency, the most common viruses were rhinoviruses, influenza, parainfluenza, coronaviruses, metapneumoviruses and RSV [48, 50].
With the arrival of the COVID-19 pandemic (figure 2), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the role of respiratory viruses in causing severe lung infections like pneumonia has become ever more important. Indeed, as observed in other epidemics, e.g. severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS) and the H1N1 strain of influenza virus A, these types of viruses can lead to complications such as ARDS [22, 38, 51, 52].
 FIGURE 2
FIGURE 2 Evolution of the coronavirus disease 2019 (COVID-19) pandemic. The first cases of unknown pneumonia were reported in Wuhan, China in December 2019. Over the following 2 years, more than 504 million cases were confirmed worldwide, including 6.2 million deaths. FDA: Food and Drug Administration; IDSA: Infectious Diseases Society of America; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2; WHO: World Health Organization.
Respiratory virus transmission and transmissibilityAerosol (fine, <5 µm, short and long range), droplet spray (large >100 µm), direct contact (physical) and indirect contact (fomite) are the four main modes of respiratory virus transmission. During an acute respiratory viral infection, an infected person may shed the virus during expiratory activities (examples include breathing, speaking, exhalation, sneezing and coughing) in the form of droplets and aerosols [53, 54]. Droplets can travel less than 2 m and, due to their size (>100 µm), fall to the ground or surfaces, resulting in contaminated areas (hands, clothing, tables, etc.). This can then facilitate direct (handshake with contaminated skin) and indirect contact transmission (touching a table with fomites). Furthermore, aerosols (<5 µm) can travel within and beyond a metre. These aerosols can also float in the air for hours, allowing transmission over short and long distances [55].
During the COVID-19 pandemic, research on the role of airborne transmission of respiratory viruses, especially that of SARS-CoV-2, accelerated. This mode of transmission is currently under re-evaluation in respiratory viral infections. The sites of respiratory aerosol formation (oral, laryngeal, bronchial, bronchiolar and alveolar), the process involved in aerosol formation (fluid lining the airways), host characteristics (children and adults) and environment play an important role in the size and number of aerosols produced, as well as the viral content of such aerosols and transmission. For example, during coughing, sneezing, breathing and talking, individuals produce small aerosols (1 µm). Despite their size, they can carry respiratory viruses like influenza virus (100 nm–1 µm) or rhinovirus (15–30 nm). An experimental study by Yan et al. [56] analysed nasopharyngeal and 30 min breath samples (coarse >5 µm and fine ≤5 µm fractions) on days one to three after symptom onset in 355 symptomatic volunteers with acute respiratory illness, where confirmed influenza infection was reported in 142 volunteers. The authors assessed viral RNA copy number for all samples and cultured nasopharyngeal samples and fine aerosols (≤5 µm). They recovered infected virus from 89% of the nasopharyngeal samples (n=150) and 39% from fine aerosols (n=52). They reported RNA copy numbers as follows: 3.8×104 in the 30 min fine sample, 1.2×104 in the 30 min coarse aerosol sample and 8.2×108 in the nasopharyngeal sample. The significance of the study comes from the finding that in the small aerosols produced during natural breathing of infected individuals, recovering influenza viral RNA is possible. Another point of interest obtained from this study was the possible role of asymptomatic individuals in spreading viruses; its relationship to the rapid spread of SARS-CoV-2 is worth considering [57].
A prospective proof-of-concept study by Malik et al. [58] detected a mean viral load of 2.47×103 copies per 20 times exhaled breath samples from patients with COVID-19. Interestingly, an experimental study by Liu et al. [59] measuring viral RNA in aerosols from different areas of two Wuhan hospitals that treated patients with COVID-19 found that higher concentrations of SARS-CoV-2 RNA were detected in patient bathrooms (19 copies·m−3) and healthcare personnel areas (meeting room: 18 copies·m−3; male staff changing room: 20 copies·m−3; female staff changing room: 11). Lower levels of SARS-CoV-2 RNA were detected in isolation wards and ventilated patient rooms. The authors reported that detection of SARS-CoV-2 occurs most commonly in aerosols in the submicron (0.25–1.0 μm) and supermicron (>2.5 μm) ranges. The authors also reported finding deposited samples in the ICU with a range of deposition between 31 and 113 copies·m−2·h−1; these samples were detected approximately 1–3 m away from patients’ beds.
A study by Fears et al. [60] compared the dynamic aerosol efficiency of SARS-CoV-2 with that of SARS-CoV and Middle Eastern respiratory syndrome coronavirus (MERS-CoV), and quantified long-term persistence and the ability to maintain infectivity when suspended in aerosols. The authors reported that, unlike other beta-coronaviruses, SARS-CoV-2 maintained its infectivity when transmitted through the air over short distances. In addition, aerosols containing SARS-CoV-2 kept their morphology, size and aspect ratios for up to 16 h. All these data suggest that an infected person with SARS-CoV-2 is able to produce possibly infectious aerosols via human shedding and airborne transport for a long period, and that SARS-CoV-2 is very resistant in aerosol form, even over lengthy periods.
Airborne transmission was demonstrated in respiratory viruses such as influenza virus, RSV, human rhinovirus, adenovirus, enterovirus, SARS-CoV, SARS-CoV-2 and MERS-CoV. This evidence, therefore, supports the need to continue investigating this mode of transmission and to implement precautionary measures against infections and outbreaks [61–71].
TransmissibilityTo determine the transmissibility of a pathogen, we should consider several factors, including infectivity of the micro-organism, host susceptibility, contact patterns between micro-organism and host, and environmental characteristics during transmission [72]. Determining the ability of a pathogen to spread is important for applying preventive measures for infections and outbreaks. The basic reproductive number (R0) measures the average number of new cases generated per infectious case; the higher the R0 number, the greater the risk for transmissibility. Figure 3 shows the R0 number of the main respiratory viruses.
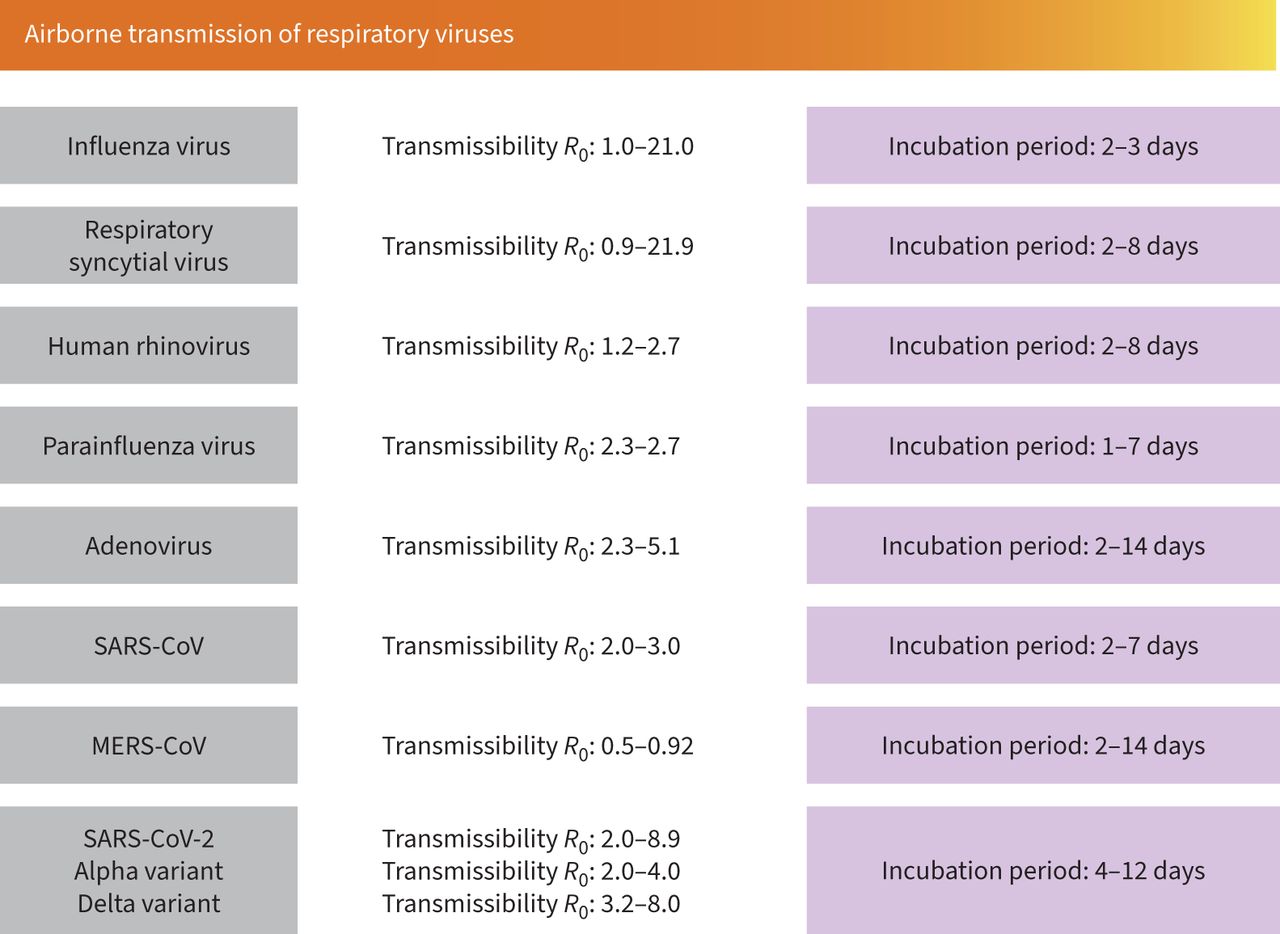 FIGURE 3
FIGURE 3 Airborne transmission of respiratory viruses. Data about the incubation period for various respiratory viruses and their basic reproduction number (R0).
Host risk factors for severe lung viral infectionAge, sex, previous comorbidities (e.g., obesity, diabetes mellitus, hypertension, cardiovascular disease, cerebrovascular disease, chronic pulmonary disease, liver disease) and immune impairments (e.g., pregnancy, presence of malignancies, cytotoxic therapies, autoimmune diseases, advanced HIV infection) are the main host factors related to severe outcomes (ICU admission and short- and long-term mortality) in lung viral infections (table 1) [73–75].
TABLE 1Patient-related risk factors for severe viral lung infections
A decline in immune function or immunosenescence in older adults increases susceptibility to infections and the risk of serious complications. This occurs as a result of a deterioration in function in both the acquired and innate immune systems. In addition, ageing and chronic comorbidities (e.g., hypertension, diabetes and cardiovascular diseases) induce chronic endothelial dysfunction, which is also related to vasoconstriction, inflammation and coagulation. Endothelial dysfunction has been suggested to be related to the pathologic process in severe lung infections due to pathogens like influenza A virus, SARS-CoV, MERS-CoV and SARS-CoV-2 [76–78]. It is important to recognise that immunosenescence and chronic comorbidities impair the capacity of the endothelial progenitor cells to regenerate after endothelial cell injury [79, 80].
In a retrospective observational study by Cillóniz et al. [21], investigators analysed data from 2760 hospitalised patients with CAP, finding that 8% presented viral CAP. The most frequently identified viruses in these cases were influenza virus A (52%), rhinovirus (13%) and RSV (10%). Amongst the patients with viral CAP, 61% presented sepsis; male sex and age ≥65 years were independent risk factors for viral sepsis. Although the pathogenesis of COVID-19 has not been fully investigated, reports from several global studies provide enough information to consider severe COVID-19 as viral sepsis. This hypothesis finds its basis in observations made of the systemic inflammatory response, immunosuppression, damage or failure of multiple systems and organs, and chronic damage in some patients. There is a similarity to the pathogenesis of bacterial sepsis [81, 82].
Conditions such as obesity are risk factors due to diminished antibody response, immune deregulation due to adiposity and deficient adaptive responses. Results from a large cross-sectional study in the US including data from 540 667 adults hospitalised with COVID-19 (1 March 2020–31 March 2021) showed that chronic comorbidities increased the risk of severe COVID-19. Obesity had the strongest association with death [83].
In cases of pregnancy, risk is related to both the tolerant immunologic state and the influence of sex steroid on the immune response. During the influenza pandemic in 1918, pregnant women were at a particularly high risk of infection and poor outcomes. Approximately 50% of pregnant women infected during that time died [84]. Similar findings were reported during the influenza A(H1N1)pdm09, in which pregnant women faced a high risk of severe disease, required intensive care, had complications and experienced mortality more than nonpregnant women [85]. In a repeated cross-sectional study done in the US over nine influenza seasons (2010–2019) [86], which included data of 9652 hospitalised women with influenza infection, investigators reported that 2690 (28%) were pregnant and had a median age of 28 years. Similarly, 62% of these women were in their third trimester, with 42% presenting at least one comorbidity. The authors report that 5% of pregnant women required ICU admission, 2% needed mechanical ventilation and 0.3% died (n=8). Cases in which influenza A H1N1 was identified had more severe outcomes than those in which influenza A H3N2 was the causative pathogen. A propensity score-matched analysis (COV19Mx) analysed data from pregnant and nonpregnant women (n=5183 in each group) hospitalised due to COVID-19. The authors reported that pregnant women had a higher risk of death (odds ratio (OR) 1.84, 95% CI 1.26–2.69), pneumonia (OR 1.86, 95% CI 1.60–2.16) and ICU admission (OR 1.86, 95% CI 1.41–2.45) than non-pregnant women [87]. An interesting systematic review and meta-analysis [88] revealed the outcomes of 19 studies that included data from 79 pregnant women (41 with COVID-19, 12 with MERS and 26 with SARS). 90% of hospitalised pregnant women with coronavirus infections (MERS, SARS, COVID-19) presented pneumonia, with fever, cough and lymphopenia being the most frequent symptoms. These women also presented a higher rate of pre-term birth, pre-eclampsia, caesarean and perinatal death. Interestingly, ICU admission (9%) and mechanical ventilation (5%) were less common in pregnant women with COVID-19 compared to those with either MERS (44% and 40%, respectively) or SARS (53% and 40%, respectively). There was no case of maternal death due to COVID-19 infection; however, the pooled mortality of MERS and SARS infections ranged from 25% to 30%. Finally, a multinational cohort study [89] including data from 706 pregnant women with a COVID-19 diagnosis and 1424 pregnant women without a COVID-19 diagnosis reported that the former group were at a higher risk of pre-eclampsia/eclampsia (relative risk 1.76, 95% CI 1.27–2.43), severe infections (relative risk 3.38; 95% CI 1.63–7.01), ICU admission (relative risk 5.04; 95% CI 3.13–8.10), maternal mortality (relative risk 22.3, 95% CI 2.88–172), pre-term birth (relative risk 1.59, 95% CI 1.30–1.94), medically indicated pre-term birth (relative risk 1.97, 95% CI 1.56–2.51), severe neonatal morbidity index (relative risk 2.66, 95% CI 1.69–4.18) and severe perinatal morbidity and mortality index (relative risk 2.14, 95% CI 1.66–2.75). The most frequent presentation was pneumonia (91.8%), whilst the most common symptoms were fever (82.6%), cough (57.1%) and dyspnoea (27.0%). For all coronavirus infections, the pooled proportion of miscarriage was 64.7%. Eighty percent of pregnant women underwent a caesarean delivery. The pooled proportion of perinatal death was 11.1% and 57.2% of newborns needed intensive care. The pooled maternal death was 12.3%. Finally, a systematic review and meta-analysis including 192 studies and data from more than 67 000 pregnant women reported that those with COVID-19 were more likely to deliver pre-term. Similarly, this same group faced an increased risk of maternal death and needed intensive care. Their babies would also be more likely to need intensive care [90]. All of these data emphasise the importance of influenza and COVID-19 vaccination in this specific population.
The role of biomarkers in severe lung viral infectionsThe first line of defence against virus infection and limiting viral disease is the innate immune response. However, an excessive and uncontrolled innate immune response can cause damage to the host. This, in turn, can cause excessive tissue infiltration by immune cells and possibly lead to tissue destruction. Indeed, this was the case for the influenza pandemic in 1918, where an exaggerated pro-inflammatory immune response was thought to have played an important role in the high level of morbidity and mortality [91]. During the influenza A H1N1(pdm)09 pandemic in 2009, an exuberant inflammatory cytokine response was also reported in severe cases related to ARDS complication. Increased levels of interleukins (IL) 1, 8, 10, 6 and tumour necrosis factor α (TNF-α) were observed in severe cases of influenza AH1N1 [92]. In patients with MERS infection, serum levels of cytokines (IL-10, IL-15, TGF-β and epidermal growth factor) correlated with disease severity [93]. Similarly, in patients who developed ARDS due to SARS-CoV infection, cytokines such as IL-1, IL-6, IL-8 and TNF-α were detected at higher levels in plasma. In patients with severe COVID-19, many cytokines such as interferon-γ, TNF, granulocyte-colony stimulating factor, IL-1, IL-6, IL-18 and IL-33 were also detected at higher levels. In some cases, these laboratory findings were related to severe complications such as ARDS or multiple organ dysfunction [94, 95]. Interestingly, in most severe COVID-19 cases, lymphopenia was reported. This may explain how SARS-CoV-2 has been able to evade the immune system [96–98]. Lymphocytes play a key role in the immune homeostasis and inflammatory response. Until now, the mechanism responsible for lymphopenia has yet to be fully understood. However, some studies have suggested that lymphocyte apoptosis due to direct SARS-CoV-2 infection is possible [96]. Another possible mechanism that could induce lymphopenia may be the higher levels of cytokines and their synergic actions [96, 99].
Considering the aforementioned studies, the importance of biomarkers for the prognosis of severe lung viral infection is evident, especially in critically ill patients who need prompt intensive care.
Inflammatory biomarkersInflammatory biomarkers such as C-reactive protein (CRP), procalcitonin (PCT), IL-6, IL-8, IL-10, lactate dehydrogenase (LDH), ferritin and D-dimer increase greatly during a systemic inflammatory response and are correlated to disease severity. Higher levels of CRP were associated with disease severity in SARS, MERS, influenza AH1N1 and SARS-CoV-2 infection. There are data that indicate that higher levels of CRP are associated with the severity and prognosis of excessive inflammatory responses [100, 101]. Elevated values of PCT would reflect bacterial co-infection, which is related to severe lung viral disease. Especially useful in severe disease, consistent measurements of PCT levels in critically ill patients may provide an important value in predicting co-infections and helping guide antibiotic therapy [102, 103]. In severe viral lung infection, co-infection and superinfection with bacteria (Streptococcus pneumoniae, Staphylococcus aureus, Pseudomonas aeruginosa) or fungi (Aspergillus spp.) should always be considered, especially in critically ill patients. Recent reports showed a higher incidence of co-infections and superinfection in patients with COVID-19, especially in severe cases requiring mechanical ventilation [104–109].
Patients with ARDS and sepsis presented elevated levels of PCT. Such patient characteristics could facilitate early identification and treatment. PCT has been suggested to be a mediator of inflammation; partly because higher levels of PCT are a result of a complex interaction between cytokines such as IL-6 and TNF-α. Two meta-analyses reported an association between higher levels of PCT and COVID-19 severity. In the first meta-analysis, which included data from four studies, the authors reported that an increase in PCT values was associated with a nearly fivefold higher risk of severe COVID-19 (OR 4.76, 95% CI 2.74–8.29) [110]. The second large meta-analysis included 32 studies with data from 10 491 COVID-19 cases and reported an association between elevated PCT values and poor outcomes (OR 6.99, 95% CI 4.76–10.27) [111].
Haematological and biochemical biomarkersLeukocyte, neutrophil, lymphocyte and platelet counts, as well as the neutrophil-to-lymphocyte ratio, are easily available biomarkers and related to disease severity in severe lung viral infection.
Leukocytosis, neutrophilia, lymphopenia and thrombocytopenia are correlated with viral lung infection severity. These patterns have been commonly observed in severe cases of influenza AH1N1 (2009 pandemic), SARS, MERS and COVID-19. There is no clear explanation for lymphopenia; however, a dysregulated immune response to the viral infection is believed to cause lymphocyte apoptosis or result from direct lymphocyte infection.
The continuous infiltration of neutrophils at the site of viral infection and their degranulation and release of neutrophil extracellular traps induce the production of pro-inflammatory cytokines. This elevation in cytokines caused by the dysregulation of the immune response could also contribute to endothelial injury resulting from ARDS and sepsis [112].
Neutrophils and lymphocytes rapidly respond to viral infection. Neutrophil count increases dramatically and then these cells migrate to the area of infection. Conversely, lymphocyte count decreases due to immunosuppression. This explains the relationship between an increase in neutrophil to lymphocyte ratio and severe lung viral disease: the ratio reflects the balance between systemic inflammation and immunity [112].
Thrombocytopenia was reported in severe cases of influenza A/H1N1 (2009 pandemic), SARS, MERS and COVID-19 [92, 113]. Platelets are mediators of inflammation. Viral infections cause a systemic inflammatory response which can cause a dysregulation between pro-coagulant and anticoagulant homeostatic mechanisms. An elevated level of D-dimer reflects a state of hypercoagulability and fibrinolysis and may indicate thrombotic risk. A systematic review and meta-analysis of 100 studies included data from 38 310 patients with COVID-19 and reported that a higher D-dimer level served as a good predictive prognostic marker of disease severity (area under the curve (AUC) 0.69) and mortality (AUC 0.79) [114]. This finding was also observed in severe cases of SARS, MERS and influenza AH1N1 (2009 pandemic) [113, 115].
A dysfunctional immune response is associated with severe lung viral infections and an elevation in biomarkers such as ferritin, LDH and IL-6. Therefore, biomarkers provide reliable, timely and accessible information that could help clinicians in managing severe lung viral infections.
Microbiologic diagnosisAn accurate microbiologic diagnosis of respiratory viruses might help to avoid unnecessary antibiotic treatment and accurately prescribe specific antiviral treatment when indicated. Nasopharyngeal swabs, sputum samples, endotracheal aspirate and bronchoalveolar lavage are recommended to detect respiratory viruses. In mild cases, nasopharyngeal swabs are optimal samples for detecting respiratory viruses due to the higher viral replication. In severe cases, lower respiratory samples (sputum, endotracheal aspirate or bronchoalveolar lavage samples) are recommended. Virus replication in the lower respiratory tract may be detectable for longer periods than in the upper respiratory tract and nasopharyngeal swabs can give false negatives. Two review articles provided general overviews of the microbiologic diagnosis of pneumonia, including important data about microbiologic diagnostic testing for respiratory viruses that cause pneumonia [116, 117]. A recent review by Colagrossi et al. [118] provided an overview of the rapid microbiologic detection of the main respiratory viruses.
Identifying the causative respiratory viruses of severe lung infection is vital for the management and prevention of hospital transmission. There are different diagnostic approaches in cases of severe pulmonary viral infection. In the last few years, the use of molecular techniques has contributed to an increase in the reported rate of respiratory viruses causing severe lung infections. Due to its high sensitivity and specificity, nucleic acid amplification testing is the method of choice for the microbiological diagnosis of virus infection. In any cases, due to the risk of co-infection or superinfection with other viruses or bacteria, it is necessary to use multiplex PCR techniques [119, 120].
Antiviral therapyOseltamivir, a neuraminidase inhibitor (NAI), is the most frequently used antiviral to treat severe influenza lung infection [121]. Oseltamivir is active against influenza A and B viruses, but not against other respiratory viruses [121]. Furthermore, oseltamivir is currently recommended as a first-line treatment for severe influenza infection and in patients with a risk of complications [122, 123]. Timing of treatment initiation is a critical aspect when using oseltamivir. Initiating treatment within 2 days of symptom onset or hospitalisation appears to be more efficacious, although benefits have also been reported up to within 4 or 5 days of symptom onset [122]. A meta-analysis that included data from 29 234 patients with influenza virus A (H1N1), of whom 5103 were critically ill adults, reported a significant reduction in mortality risk in patients receiving early NAI (≤2 days of symptom onset) [124]. Another observational study reported that early therapy (<48 h) was associated with reduced mortality (OR 0.69, 95% CI 0.51–0.95) in 2124 critically ill patients with influenza virus lung infection [125]. Early oseltamivir therapy was associated with a 33% reduction in ICU mortality when compared with late therapy. Early oseltamivir therapy was also associated with both a shorter ICU length of stay and duration of mechanical ventilation. Additionally, a cohort study reported that early therapy was associated with a significantly lower mortality and shorter ICU length of stay in critically ill patients with severe influenza A/H3N2 lung infection [126]. However, in cases caused by either influenza A/H1N1 or B viruses, this effect was not observed.
Another NAI is peramivir. A recent randomised controlled study by Chen et al. [127] evaluated the efficacy of peramivir and oseltamivir in severe influenza pneumonia. In terms of virus positivity duration and time of symptom remission, the authors reported no significant differences between patients who received oseltamivir and those who received peramivir. Nevertheless, the study population was small, with 20 cases in each group. Further evidence is needed to evaluate the efficacy and safety of NAIs other than oseltamivir in treating severe influenza lung infections.
In a human airway epithelium model, baloxavir, a new antiviral that inhibits the endonuclease function of the polymerase acidic protein, was investigated in vitro in combination with an NAI in treating severe influenza infections. A synergism was demonstrated between these two antivirals in the model [128]. The FLAGSTONE study compared the efficacy of the combination of baloxavir and NAI (241 cases) with the use of neuraminidase alone (125 cases) in treating severe influenza infections [129].
The combination of baloxavir and NAI was not superior to NAI alone in terms of reduction of median time to clinical improvement (97.5 versus 100.2 h, p=0.467). Interestingly, patients in the baloxavir–NAI group cleared infectious virus from the upper respiratory tract sooner than patients in the NAI-alone group did (23.9 h versus 63.7 h; p<0.0001). Despite that result, this study did not show superiority in the use of combination therapy in treating severe influenza cases. It is important to remark that the reduction in viral load shown with the combination therapy of baloxavir–NAI, together with the fact that the combination therapy targeted different sites of the virus, could reduce the possibility of resistance. However, more research is needed in the use of such therapies for severe influenza infections.
Antivirals used to treat severe and high-risk RSV infections include ribavirin (blocks viral polymerase) and palivizumab (a monoclonal antibody that prevents membrane fusion by binding to the viral envelope fusion protein) [130, 131]. Specific antivirals for the treatment of severe viral lung infections caused by non-influenza viruses are scarce.
In cases of COVID-19, we can distinguish five stages of severity (figure 1): 1) asymptomatic stage, when an individual tests positive for SARS-CoV-2 but does not present symptoms of infection; 2) mild disease stage, when an individual develops mild symptoms (e.g., fever, cough, taste/smell changes but does not present dyspnoea); 3) moderate disease stage, characterised by an oxygen saturation ≥94% and lower respiratory tract disease; 4) severe disease stage, characterised by an oxygen saturation <94%, respiratory rate >30 per min and lung infiltrates >50%; and 5) critical disease stage, characterised by the presence of respiratory failure, shock, multi-organ dysfunction or failure [132]. In the first stages of COVID-19 disease, viral replication is higher, whereas in the moderate to severe stages, inflammation is prominent. In the severe and critically ill disease stages, hypercoagulability has been reported. The current recommendation for treating COVID-19 cases is based on these principles. The effectiveness of antiviral therapy is higher in the early stages of COVID-19 and the effectiveness of anti-inflammatory agents is key during the severe and critical disease stages [133–135]. In hospitalised patients with COVID-19 requiring supplementary oxygen therapy, recommendations include using remdesivir or dexamethasone or a combination of both [133]. In hospitalised patients with COVID-19 requiring oxygen through a high-flow device or noninvasive ventilation, the recommendation is to use dexamethasone alone or in combination with remdesivir. For those patients with systemic inflammation or whose oxygen needs are rapidly increasing, it is advisable to add baricitinib or tocilizumab. Patients requiring extracorporeal membrane oxygenation or invasive mechanical ventilation should receive dexamethasone alone or dexamethasone plus tocilizumab [133].
Interestingly, a recently published prospective controlled nonrandomised study [136] investigated the effectiveness of the combination remdesivir–dexamethasone (76 cases received remdesivir–dexamethasone) compared with dexamethasone alone (75 cases received dexamethasone alone) in cases of severe COVID-19 requiring supplemental oxygen therapy. It showed a significant reduction in mortality and length of hospitalisation and faster SARS-CoV-2 clearance in patients who received remdesivir–dexamethasone compared to patients who received dexamethasone alone.
Despite the higher burden of severe lung viral infections, available effective antiviral treatments are generally scarce.
Corticosteroids: benefit or harmThere are strong data that show a relationship between the administration of corticosteroids and higher mortality rates in patients with severe influenza infection [117, 137, 138] (table 2). In a meta-analysis that included data from 6548 patients with influenza pneumonia, the authors reported that the mortality risk ratio was 1.75 for the group of patients who received corticosteroids [139]. Similar results were reported when only patients with influenza A (H1N1) virus were analysed (relative risk 1.61). In this report, patients who received corticosteroids had a longer ICU length of stay compared to those patients who did not. Another systematic review and meta-analysis that included data of 6427 patients with severe pneumonia and ARDS reported that patients who received corticosteroids had a higher mortality (OR 1.53) and incidence of nosocomial infections (OR 3.15) [140]. A retrospective observational study published in 2021 that used propensity score analysis reported that 25% of the study population received systemic corticosteroids within 7 days of hospital admission. The author found an increased risk of mortality in patients with severe influenza pneumonia, even if corticosteroids were started within this period [141]. The current recommendations from the American Thoracic Society and Infectious Diseases Society of America are against the use of corticosteroids in adults with severe influenza pneumonia (this is a conditional recommendation with low-quality evidence) [122].
TABLE 2Experience with corticosteroids: severe influenza virus infection and coronavirus disease 2019 (COVID-19)
On the other hand, at the beginning of the COVID-19 pandemic, the systemic inflammation observed in patients with severe cases of COVID-19 suggested that the use of corticosteroids may be a good option to modulate the immune response to the viral infection. However, there was not enough clinical evidence about their use (table 2). The results from the RECOVERY trial reported that the use of 6 mg dexamethasone per day for 10 days in patients with COVID-19 requiring oxygen therapy showed a reduction in all-cause, 28-day mortality (p<0.001) [142]. The results of a prospective meta-analysis of clinical trials including critically ill patients with COVID-19 carried out by the WHO showed that the use of systemic corticosteroids compared with routine care or placebo was associated with a reduction in all-cause, 28-day mortality [143]. These findings contribute the necessary clinical evidence to recommend the use of corticosteroids in patients with severe COVID-19 requiring oxygen therapy. Currently, there are more data suggesting that the use of corticosteroids in an early stage of infection could be harmful for the patient, suppress host antiviral activity and cause cytopathic damage to the alveolar epithelial cells [144]. However, the use of corticosteroids in patients whose immune system has controlled viral replication could prove beneficial: these drugs could help reduce pro-inflammatory cytokines, enhance anti-inflammatory cytokines, decrease lung vascular permeability, improve epithelial barrier integrity and promote alveolar oedema fluid clearance [145–148].
The European Respiratory Society living guidelines on COVID-19 recommend the use of corticosteroids only for patients with hypoxemic respiratory failure requiring oxygen administration [149]. The recommendation set in the National Institutes of Health guidelines for COVID-19 therapy recommend the use of systemic corticosteroids in patients requiring supplemental oxygen [150].
At present, there are some remaining questions that warrant further investigations of the use of corticosteroids in severe COVID-19 (including determining the required dosage) in order to understand the effect of corticosteroids on viral clearance and replication and to elucidate any possible long-term benefits in pulmonary sequelae.
PreventionInfluenza vaccination is particularly important for people who are at a higher risk of severe influenza infection (the elderly, pregnant women and those with immunosuppression or chronic medical conditions). Yearly influenza vaccination is also recommended for healthcare workers, inpatient and outpatient settings, and long-term care facilities [151]. Despite the fact that RSV infection can cause severe lung infection (especially in immunocompromised patients), there is no licensed vaccine for RSV. To date, five COVID-19 vaccines (BioNTech-Pfizer, Moderna, AstraZeneca, Johnson & Johnson and Novavax) have been authorised by the European Medicines Agency [152]. These vaccines have demonstrated efficacy and effectiveness [153]; however, more investigation is needed, especially in specific populations such as pregnant women and immunocompromised patients. The type and dose of vaccine and the timing of the primary and booster vaccinations depend on the characteristics of each individual and possible chronic comorbidities. International organisations and scientific societies regularly update clinical considerations for the use of COVID-19 vaccines.
Following the COVID-19 pandemic, different strategies to prevent the transmission of SARS-CoV-2 virus were established. Today, there is an overwhelming amount of scientific evidence about the possible airborne transmission of SARS-CoV-2 and other respiratory viruses. Important strategies to prevent the transmission of respiratory viruses include quarantine in infected people [154], wearing masks [155–157], washing hands, disinfecting surfaces, social distancing [158] and ventilating spaces [159].
The application of these simple measures during the COVID-19 pandemic considerably reduced the transmission of influenza and other respiratory viruses (RSV, metapneumovirus, enterovirus, adenovirus, parainfluenza virus types 1–3 and rhinovirus) in the winter season of the southern hemisphere during 2020 [160, 161]. These observations showed the importance of such measures in reducing the impact of viral infections.
ConclusionSince COVID-19 first emerged in December 2019, we have witnessed an unprecedented collaborative research effort between the global scientific and medical communities. Such actions have afforded us a better understanding of this disease, including its mode of transmission, symptoms, diagnosis, evaluation, management, prevention and short- and long-term sequelae. Similarly, continually updated knowledge about COVID-19 has facilitated the development of rapid diagnostic techniques, contributing to improved management and treatment of people with a higher risk of severe disease. We are strengthening our comprehension of the relationship at play between our immune systems and SARS-CoV-2, with numerous biomarkers already being investigated to help predict disease severity. Indeed, it has even become possible to develop effective antiviral drugs against SARS-CoV-2 and conceive effective vaccines. However, much remains to be understood about SARS-CoV-2 and the aftermath of the COVID-19 pandemic. The scientific advances made thus far have set the bar high for scientists and clinicians; we must apply this same degree of commitment to other respiratory viruses related to severe lung infection for which high morbidity and mortality pose a real risk for certain patients. There is a critical need to optimise care as it relates to the diagnosis, evaluation, management and therapy of those patients with severe viral lung infections.
AcknowledgmentsThank you to Anthony Armenta, ECHAlliance (European Connected Health Alliance), Spain, for providing language editing assistance for this article.
FootnotesThis article has an editorial commentary: https://doi.org/10.1183/16000617.0150-2022
Provenance: Commissioned article, peer reviewed.
Previous articles in this series: No. 1: Kumar K, Daley CL, Griffith DE, et al. Management of Mycobacterium avium complex and Mycobacterium abscessus pulmonary disease: therapeutic advances and emerging treatments. Eur Respir Rev 2022; 31: 210212.
Number 2 in the Series “Respiratory infections” Edited by Antoni Torres and Michael S. Niederman
Author contributions: All authors participated in the conception, design, critical revision for important intellectual content and final approval of the submitted version.
Conflicts of interest: A. Torres reports he is a current Editorial board member for the European Respiratory Review, and reports participation on Advisory Boards or lectures for Pfizer, MSD, Biomerieux, Biotest and Jansen. The remaining authors have nothing to disclose.
Support statement: C. Cilloniz received a grant from the Fondo de Investigación Sanitaria (PI19/00207).
Received March 19, 2022.Accepted May 30, 2022.
留言 (0)