
記住我
Sir,
Granuloma annulare, first described by Colcott and Fox in 1895, and formally named in 1902 by Radcliffe-Crocker, is a common noninfectious granulomatous cutaneous condition.1 Granuloma annulare has several sub-types, including localised, generalised, sub-cutaneous, macular or patch and various atypical morphologies. Granuloma annulare localised to the external ear is very rare. Herein, we report a case of auricular granuloma annulare with dermoscopic manifestations.
A 49-year-old male presented with a 6-month history of multiple asymptomatic firm skin-coloured to erythematous papules involving both auricular antihelixes [Figures 1a and b]. There was no history of trauma, insect bite, or excess solar exposure. The patient was in good health and stated no prior medical history. On dermoscopy (JD801D, Jiangsu Jieda Technology Co., Ltd, Jiangsu, China), the right auricular lesion presented a daisy pattern comprising a central yellow crust with peripheral linear and hairpin vessels on a white background [Figure 2a]; and the left auricular lesion revealed a central yellowish-orange structure-less area with surrounding capillary network [Figure 2b]. A lesional skin biopsy and histopathological examination from the right ear revealed palisading infiltration of histiocytes and lymphocytes around degenerated collagen fibres in the dermis [Figure 3], suggestive of granuloma annulare. After three months of topical 0.05% halobetasole cream, the lesions resolved without any recurrence at 1-year follow-up.
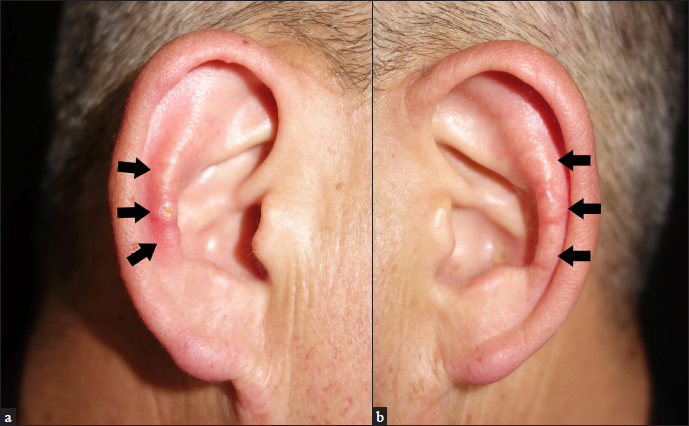
Figure 1a and b:: Multiple firm skin-colored papules (arrows) on the bilateral antihelixes: (a) right, (b) left
Export to PPT
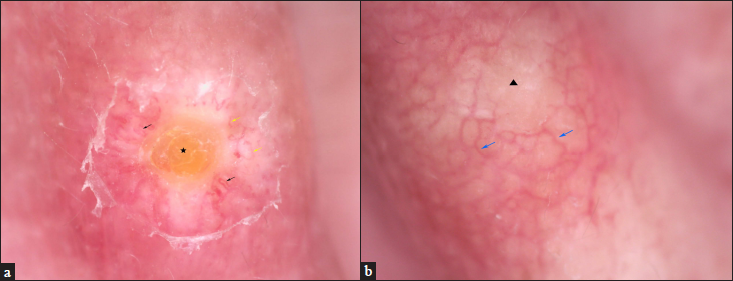
Figure 2a and b:: (a) The right lesion showed central yellow crust (pentagram) and peripheral linear (yellow arrows) and hairpin vessels (black arrows) on a white background. (non-contact polarised dermoscopy, ×50); (b) the left lesion showed central yellowish-orange structureless area (triangle) with the peripheral capillary network (blue arrows). (non-contact polarised dermoscopy, ×50)
Export to PPT
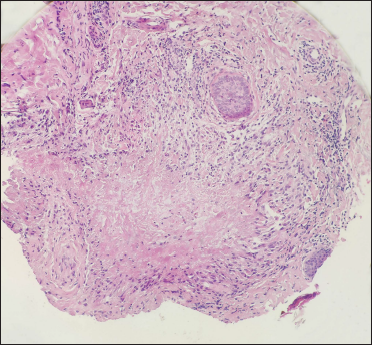
Figure 3:: Dermal palisading infiltration contained histiocytes and lymphocytes around degenerated collagen fibres (H&E, ×200)
Export to PPT
Granuloma annulare is a common non-infectious granulomatous cutaneous condition classically presenting as annular grouped skin-coloured to erythematous papules on the extremities. Although the exact pathogenesis remains unclear, cell-mediated hypersensitivity reaction is one of the proposed explanations for its development.2 It may occur as an isolated idiopathic entity, however, some reports have associated it with diabetes, hyperlipidemia, malignancy, thyroid disease and systemic infections.2 Several triggers of granuloma annulare have been reported, such as lightning strikes, tattoos, insect bites, contact dermatitis, vaccination, isomorphic response and medication.2
Granuloma annulare is more prevalent in females, with a female-to-male ratio of 2:1, and onset commonly occurs before 30 years age.3 It has varying morphologies and sub-types, and the common subtypes include localised, generalised, perforating and sub-cutaneous granuloma annulare. Other rare subtypes are linear, palmar, patch, pustular and giant granuloma annulare. Histopathology is a confirmatory diagnostic tool, characterised by dermal collagen degeneration, mucin deposition and either a palisaded or interstitial histiocytic infiltrate. The common dermoscopic features of granuloma annulare include multiform whitish areas, yellowish-orange structureless areas, and unfocused vessels (dotted, linear and branching) with an evident pinkish-reddish background.4,5 Whitish areas probably result from collagen degeneration and mucin deposition in dermis, while the granuomatous infiltrate is depicted by yellowish-orange structureless areas.4 Other dermoscopic features include pigmented structures, whitish scaling, rosettes, and crystalline leaf venations.4,5 Apart from the common dermoscopic features of granuloma annulare, we observed a special daisy pattern in our patient, which has also been described in chondrodermatitis nodularis helicis.6
Granuloma annulare localised to the external ear is very rare. To date, a total of 12 cases of auricular granuloma annulare have been reported in the literature.7,16 While granuloma annulare has female predilection, all patients with auricular granuloma annulare were male. Table 1 summarizes the cases of auricular granuloma annulare reported in literature [Table 1]. Although the exact reason for granuloma annulare on the external ear is unknown, trauma seems to be related, as reported in five patients. The lesions of auricular granuloma annulare commonly involve bilateral helixes or/and antihelixes, or occasionally ear lobe, and present as multiple skin-coloured, yellow, or erythematous papules and nodules. The majority of auricular granuloma annulare are asymptomatic, while occasional slight tenderness may be present. The histopathologic features are consistent with typical granuloma annulare. Farrar reported a case of auricular granuloma annulare with perforating features, and the lesions presented on extra-auricular sites.12 In 10 patients, the lesions were localised to the ear [Table 1]. Auricular granuloma annulare usually resolves with treatment, and only one patient presented with local recurrence in the literature.15 The effective management options include trauma avoidance, topical glucocorticoids or calcineurin inhibitors, cryotherapy and excision.7,8
Table 1:: The clinical features of 11 cases auricular granuloma annulare
Case Sex Age, year Course Clinical features Sites Possible inducement Treatment Prognosis Author 1 M 36 Several months Single tender nodule Left ear lobe Trauma Excision No recurrence Mills, 1992 2 M 21 6 months Multiple nodules Both helixes and antihelixes Trauma Excision Not described Mills, 1992 3 M 27 3 years Yellow papules Both inner helixes None Cryotherapy Improved Farrar, 2002 4 M 40 5–6 years Multiple nodules Left antihelix Trauma Not described Not described Raghava, 2004 5 M 28 1 year Skin-coloured papules Both antihelixes None Topical steroid And pimecrolimus Improved Kim, 2009 6 M 26 5 years Yellow papules Both antihelixes None Cryotherapy, excision No recurrence Dias, 2010 7 M 31 18 months Skin-coloured papules Right antihelix Trauma Avoid trauma Spontaneous regression without recurrence Shim, 2010 8 M 36 1 month Skin-coloured papules Both antihelixes Trauma Local injection of steroid No recurrence Shim, 2010 9 M 20 10 years Yellowish tender papules Left antihelix None Excision, topical steroid Recurrence Gerdes, 2013 10 M 7 6 months Skin-coloured papules Both helixes and antihelixes None Topical steroid Improved Cho, 2014 11 M 49 6 months Skin-coloured, reddish papules Both antihelixes None Topical steroid No recurrence Our caseThe differential diagnoses of granuloma annulare include rheumatoid nodules, chondrodermatitis nodularis helicis, auricular pseudocyst, sarcoidosis and epidermal cysts. Rheumatoid nodules are well-demarcated, flesh-coloured, sub-cutaneous lumps or masses, usually encountered on extensor surfaces, pressure and trauma-prone areas, in patients with rheumatoid arthritis. Typical histologic features include necrobiosis, with fibrin deposition and palisading epithelioid histiocytes.17 The dermoscopic findings comprise a pink or pink and white mixed homogeneous background, reticulate pigmentation, and fewer vessels.5 Chondrodermatitis nodularis helicis typically presents as a tender round nodule with raised edges with a central ulcer or crust, involving the helix or antihelix. Histopathology reveals epidermal ulceration with surrounding acanthosis, orthokeratosis, dermal inflammation and hyalinised eosinophilic material overlying the cartilage.18 The dermoscopic feature of chondrodermatitis nodularis helicis is a daisy pattern consisting of thick white lines, radially arranged, converging to a central rounded yellow/brown clod.6 Auricular pseudocyst is a rare benign condition corresponding to an intra-cartilaginous collection resulting in a non-inflammatory cystic swelling of the ear. Ultrasound is a useful early diagnostic tool for auricular pseudocyst.19 About 25% of sarcoidosis patients have cutaneous lesions, manifesting as maculopapules, nodules, plaques, sub-cutaneous nodules, infiltrative scars and lupus pernio.20 Histologic examination of sarcoidosis shows well-demarcated islands of epithelioid cells with occasional giant cell formation and no necrosis.20 Dermoscopy of sarcoidosis displays translucent, orange or yellowish-orange structureless areas which may be focal or diffuse along with well-focused vessels of different morphologies.5
In conclusion, we have reported a rare case of auricular granuloma annulare. Dermoscopy is a useful, non-invasive adjunctive diagnostic tool for auricular granuloma annulare, while histopathology is confirmatory. The dermoscopic findings include a daisy pattern, yellowish-orange structureless area and unfocused multiform vessels.
留言 (0)