
記住我





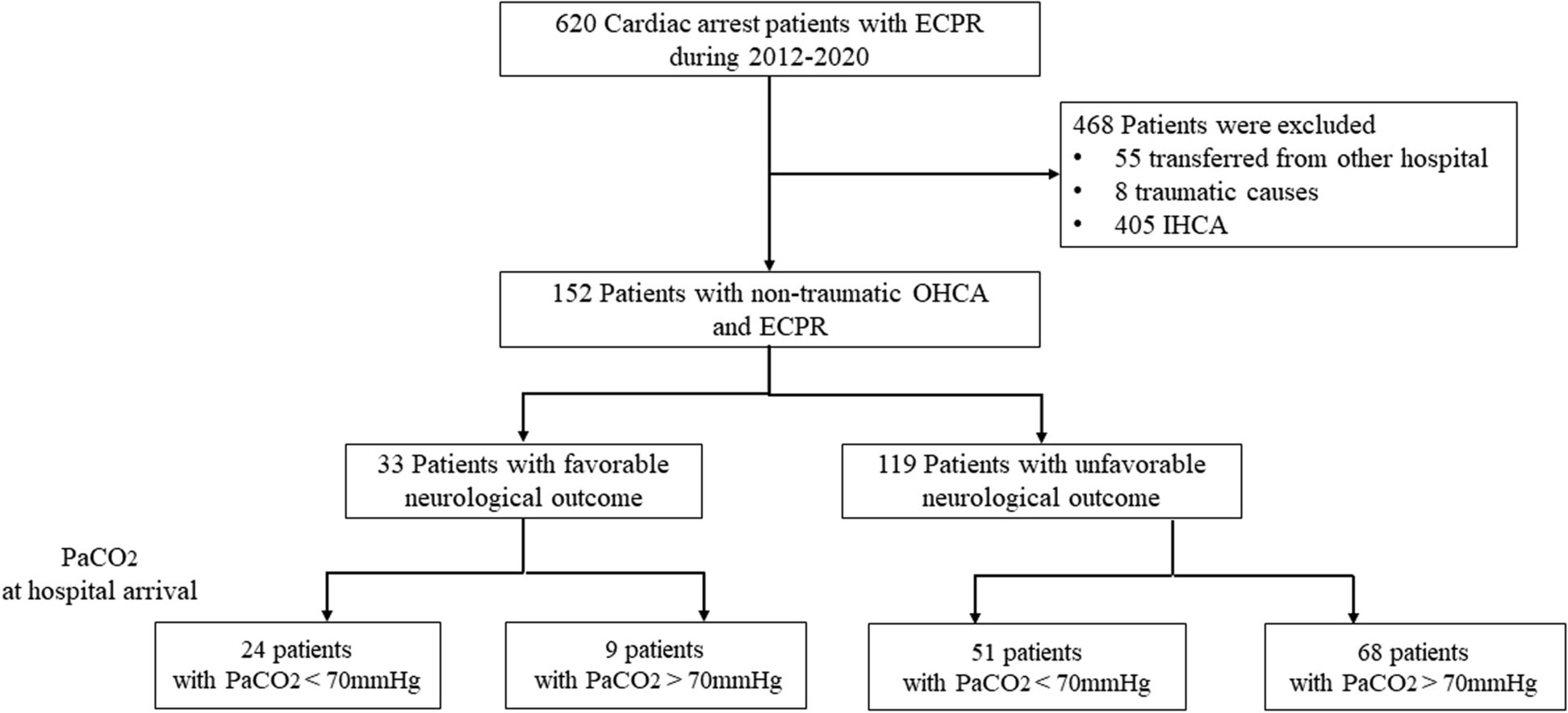

During the study period, ambulances were dispatched 177,109 times, of which 82,253 were with lights and sirens. The RRVs were dispatched 19,539 times simultaneously with the ambulance as primary response and secondarily on ambulance request in 2340 cases. Thus, rendezvous was activated in 1.3% of all ambulance tasks, corresponding to 10.7% of all RRV dispatches. Data showed that ambulance crews requested rendezvous in 2370 cases. Of these, 30 were excluded (7 duplicates and 23 interhospital transfers) (Fig. 1).
Fig. 1
Flowchart of inclusion and exclusion resulting in 1947 included cases
Thus, the study group reviewed 2340 potential rendezvous cases. Prehospital electronic patient records were then obtained and extracted for evaluation. Rendezvous failed in 330 cases, RRVs were unavailable in 7 cases, cancelled by the ambulance crew 5 times, and 51 had missing data. In total, 393 cases were excluded; thus, rendezvous was achieved, and data available in 1947 of 2340 requested rendezvous cases (83.2%).
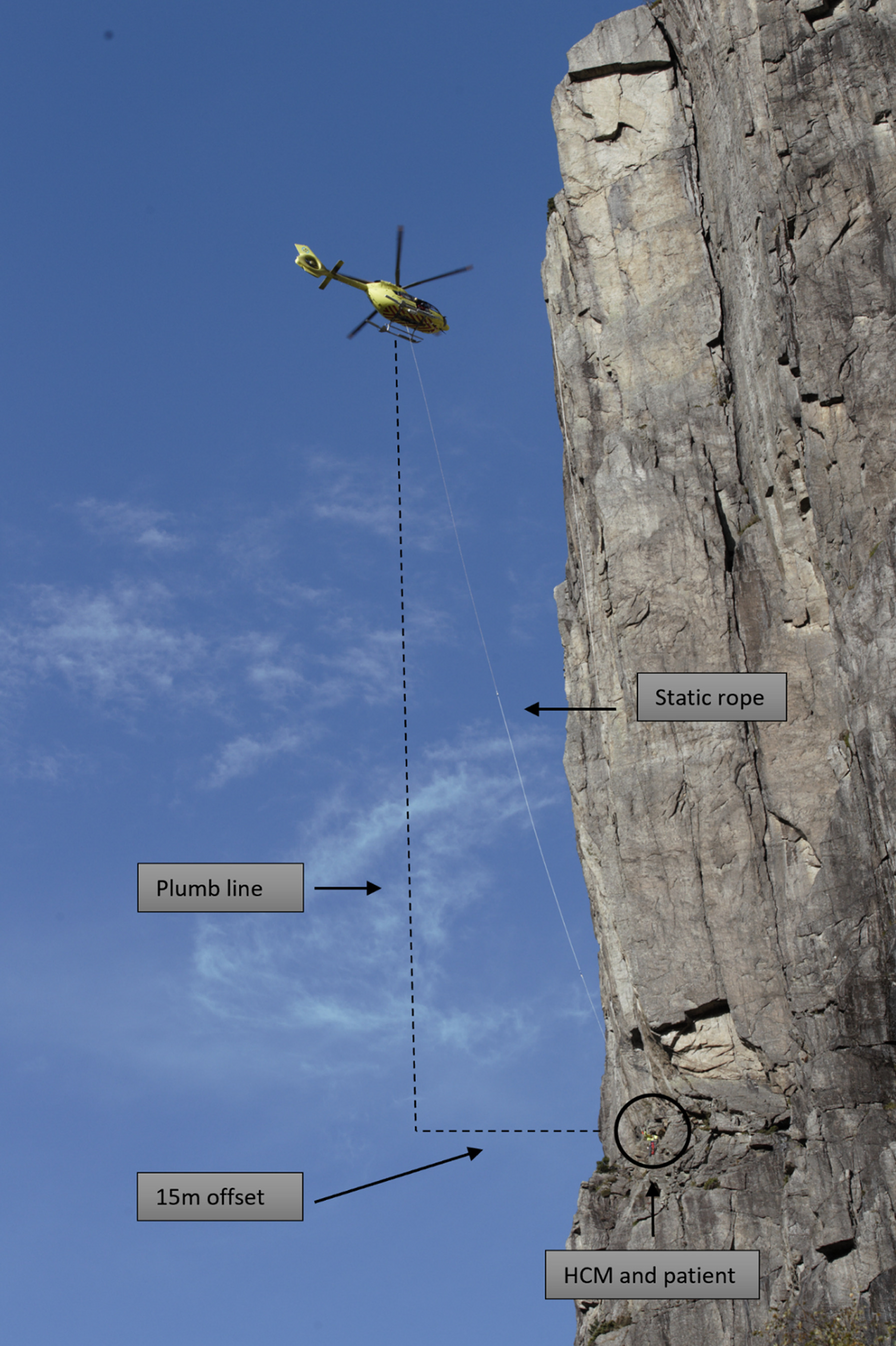
DemographicA total of 1947 cases involving 1947 patients included 780 females (40.1%),1153 males (59.2%) and 14 cases with missing data (0.7%). The median age was 61 years (IQR 50–77) (Fig. 2).
Fig. 2
Patient age and sex in rendezvous cases. Missing data: sex n = 14, age n = 18
Dispatch criteriaThe included cases were categorised by the emergency medical dispatchers’ dispatch criteria, including the category other [10] containing fever, gynaecology, burn injury, consultation, social help, urinary tract complications, prescription and ear, nose and throat problems (Table 1).
Table 1 Dispatch criteria from a total of 1947 rendezvous casesThe criterion most frequently used by the dispatchers, resulting in rendezvous, was unclear problem, which amounted to n = 561 (28.8%), followed by cardiovascular n = 439 (22.5%), neurological n = 392 (20.1%), respiratory n = 242 (12.4%), trauma/injury n = 179 (9.2%), alcohol, drugs and poisoning n = 49 (2.5%), abdominal pain n = 32 (1.6%), psychiatry n = 20 (1.0%), paediatrics n = 13 (0.7%) and other n = 20 (1.0%).
On-scene assessment by the RRV physicianCases categorised as unclear problem were further reviewed for on-scene assessment and diagnosis given by the physician. The most frequent diagnoses were cardiovascular (52.2%), followed by neurological (18.5%), respiratory (11.9%), alcohol, drugs, and poisoning (5.0%), trauma/injury (4.3%), psychiatry (4.3%), and abdominal pain (1.1%). The group Other (2.7%) included burn injury, ear, nose and throat problems and gynaecology. Thus, accounting for a similar distribution pattern of criteria given by the dispatchers for the total rendezvous population. These on-scene assessments revealed critical medical conditions, including cardiac arrest, other critical heart diseases, critical neurological conditions and respiratory distress (Table 2).
Table 2 Diagnoses in the category unclear problem based on physician on-scene assessmentRRV interventionsIn total, 1081 technical interventions and 263 non-technical interventions were registered. More than one type of intervention could be registered per patient. The most frequent technical interventions were administration of medicine n = 760 (39.0%), advanced airway management including intubation n = 161 (8.3%) and ultrasound n = 86 (4.4%). The non-technical interventions were team leading during advanced life n = 152 (7.8%), decision to end futile treatment and death certificate issuance n = 73 (3.7%), admission to a mental institution n = 26 (1.3%) and medical on-scene commander coordinating with police and fire department n = 12 (0.6%) (Table 3).
Table 3 Technical and non-technical interventions performed by the RRV physician in rendezvous cases. Percentage of all rendezvous casesMedicineMedicine was administrated by the ambulance crew or the RRV physicians. A physician administered medication in 760 (39.0%) cases. More than one type of medicine could be registered per patient. The medication most frequently administrated after RRV arrival was fentanyl n = 239 (12.3%), ondansetron n = 125 (6.4%), nitroglycerin n = 81 (4.2%), adrenaline n = 74 (3.8%), propofol n = 73 (3.7%), suxamethonium n = 48 (2.5%) and adenosine n = 44 (2.3%). Apart from propofol and suxamethonium, used for endotracheal intubation, adenosine was the most used drug not available to the ambulance crew (Table 4).
Table 4 Medicine administered by the RRV physician in rendezvous cases. Percentage of total medicine administrations
留言 (0)