
記住我


The HCHS/SOL is a population-based cohort study of 16,415 Hispanic/Latinos aged 18–74 years living in 4 US cities (Bronx, NY; Chicago, IL; Miami, FL; and San Diego, CA). Participants were recruited by using a 2-stage probability sample design, as described elsewhere [13, 14]. The baseline examination (2008–2011) included comprehensive biological, behavioral, and socio-demographic assessments. Roughly 6 years later, 11,623 participants (70.8%) returned for a second in-clinic visit (2014–2017). Annual follow-up telephone calls ascertained information on cardiopulmonary outcomes and diabetes onset. The study was approved by the Institutional Review Boards (IRBs) at all participating institutions, and all participants gave written informed consent.
Insulin resistance and diabetes status definitionDuring both visits, blood samples were collected by a venous puncture after a fasting period ≥8 h prior to the visit. Data on fasting glucose, fasting insulin, and hemoglobin A1C (HbA1C) were collected. Study procedures included a 2 h oral glucose tolerance test (OGTT). For safety reasons, the protocol specified not administering the OGTT among individuals with fasting plasma glucose (FPG) ≥ 150 mg/dL, previous diabetes diagnosis, or medications for diabetes treatment. The assays’ methodologies/procedures are described on the HCHS/SOL website (https://sites.cscc.unc.edu/hchs/node/4055). Participants were defined as having diabetes based on self-reported physician-diagnosed diabetes, documented use of diabetes medications [15], and lab data meeting any of the following criteria: fasting plasma glucose (≥126 mg/dL), post-OGTT (≥200 mg/dL), or HbA1C (≥6.5%). For all analyses, we excluded participants with diabetes at baseline. To assess incident diabetes, we applied these same criteria to determine diabetes status at visit 2, supplemented with self-report of diabetes onset from the annual follow-up telephone calls. We used fasting insulin to measure IR. Compared to other surrogate measures (e.g., HOMA-IR), change in fasting insulin is more interpretable, and has been widely used to evaluate IR in population-based studies [16]. Change in insulin was first calculated using the difference between visit values (visit 2 − visit 1). We then categorized these differences using a change in standard deviation (SD) to reflect improved (≤ −1 SD), unchanged (−1 > SD < 1), or worsened (≥1 SD) IR status throughout the 6-year follow-up.
Dietary assessmentMethods for dietary data collection have been published [4]. Briefly, two, non-consecutive 24 h dietary recalls were administered by centrally trained bilingual registered dietitians, the first in person at the baseline visit, and the second via telephone ~5–90 days later. Dietary assessment was conducted using the multiple-pass methods described by the Nutrition Data System for Research (NDS-R) software (version 11) from the Nutrition Coordinating Center, University of Minnesota. NDSR includes Hispanic and Latino foods.
We formed 34 food groups according to previously documented methodology [10]. Briefly, food groups were based on cultural and behavioral relevance, previous work (e.g., corn-based foods, burgers, meat and vegetable stews) [10, 17, 18], and consumption patterns in the data (Supplemental Table S1). For instance, we grouped ingredients (e.g., corn tortilla, beef, onion) of mixed dishes (e.g., taco) together to reflect real eating behaviors in which foods are consumed together. Whole/non-recipe foods (e.g., chocolate) were classified based on the University of North Carolina food grouping system, which disaggregates the major US Department of Agriculture’s food groups by fat and fiber [19]. Due to low consumption of some foods in some heritage groups, we aggregated low- and high-nutrient specific food groups (e.g., high- and low-fat milk into milk). Additionally, we separated fried from non-fried foods (e.g., fried vs. grilled chicken) across food groups except for corn-based foods, which traditionally include fried/grilled corn tortillas. Food group intakes (grams/day) [20, 21] were summed in each 24 h recall and then averaged for each participant. To address skewness due to high proportions of non-consumers of episodically consumed foods, we classified food group intakes into 3-level ordinal variables (non-consumers, and below and above the median). Food groups with consumption <5% in at least one heritage group were either merged with another food group or dropped from analysis.
Alternative healthy eating index (AHEI-2010)To assess “healthfulness” of each a posteriori heritage-specific DPs, we used the AHEI-2010, a diet quality index previously linked to cardiometabolic disease risk [22]. Previously established approaches were used to construct the AHEI-2010 score, which range from 0 (lowest diet quality) to 110 (highest diet quality) [6].
Hispanic/Latino heritage and covariatesQuestionnaires were interviewer-administered at both visits in English or Spanish. Hispanic/Latino heritage was self-reported at baseline from a list of heritage groups, including Cuban, Dominican, Mexican, Puerto Rican, Central American, South American, more than one heritage, and other. Other sociodemographic data collected included age at examination (years), sex (male, female), highest education achieved (less than high school (HS) diploma, HS diploma or equivalent, beyond HS), and nativity (US-born (only includes 50 states and DC)/foreign-born)) [23]. Physical activity was collected at baseline using a modified Global Physical Activity Questionnaire, which is designed to assess average time and number of days spent on a given activity in work, travel, and leisure domains [24, 25]. Data were summarized in metabolic equivalent-minutes/day and categorized as low and moderate/vigorous [24]. Smoking status at baseline was also collected using interviewer-administered questionnaires (never, former, current, missing). Waist circumference (WC) was measured using anthropometric tape at the horizontal line just above the uppermost lateral border of the right ilium. We calculated total elapsed time (years) between visits by taking the difference between visit 1 and visit 2 dates and dividing by 365.25.
Dietary pattern analysisTo empirically derive a posteriori heritage-specific factors, or DPs, we used principal factor analysis (PFA) among individuals without baseline diabetes (Supplemental Fig. S1). Because PFA requires a large sample size for stable correlations among input variables [26], we included all subjects that met the minimum inclusion criteria (e.g. no baseline diabetes, Cuban, Dominican, Mexican, Puerto Rican, Central American, or South American heritage), and two energy-plausible 24 h recalls). This resulted in a PFA sample of 11,125 which was larger than the main analyses of IR and diabetes risk (details in next section). First, we generated matrices of polychoric correlations among the 34 food groups in each heritage group, and then performed PFA on each heritage-specific matrix with orthogonal (varimax) rotation to improve interpretability and minimize correlations of derived factors [27]. Factors emerged in decreasing order of the amount of variance explained, and factor retention was guided using a modified Delphi approach, a widely used method soliciting the opinions of experts to establish a convergence of opinion [28]. Three investigators met to reconcile differences in factor retention in each heritage group based on scree plots (Supplemental Fig. S2), factor loadings, variance explained, interpretability of factors, and consistency with the literature [29]. We generated DP scores by multiplying the scoring coefficient of each food group by the individual’s corresponding food group intake category (non-consumer, below or above the median) and summing across food groups. Consistent with previous work [10], we identified overarching DPs based on 2–3 food groups with similar high factor loadings (>0.20) [11, 30] shared by two or more heritage groups. Although we understand 2–3 dietary components do not comprehensively characterize a dietary pattern, to be clear and succinct about prominent food combinations reflected in our dietary findings, we opted for this labeling approach. Lastly, we categorized heritage-specific DP scores using unweighted quintiles and evaluated mean AHEI-2010 scores by quintiles to further characterize DPs.
Among the PFA-eligible sample, we derived 19 heritage-specific DPs (4 in Cuban; 2 in Dominican; 3 in Mexican; 4 in Puerto Rican; 3 in Central American; 3 in South American) that contributed to 5 overarching DPs based on high-loading foods shared by two or more heritage groups (Supplemental Table S3). Burgers, fries, soft drinks, and pizza had high loadings for the first factor derived in each heritage group, except among South Americans, whose second factor loaded highly on these foods. We therefore classified this factor as the “Burger, Fries, & Soft Drinks” DP, which included the same foods across heritage groups. The other DPs were more heritage-specific, as the number of foods shared by different heritage groups decreased “White Rice, Beans, & Red Meats” DP was characterized by high loadings on white rice, beans, and red meats (pork or beef) in all except the South American group. The “Fish & Whole Grain” DP was characterized by fish and whole grains in Cuban, Mexican, Puerto Rican, and South American groups. The “Cheese & Sweets” DP included cheese, sweets, noodle-based foods, and fried foods in Cuban and South American groups; and a “Stew & Corn” DP included stews and corn-based foods in Puerto Rican and Central American groups. The proportion of the variance explained by heritage-specific factors ranged from 8.1 to 26.6%.
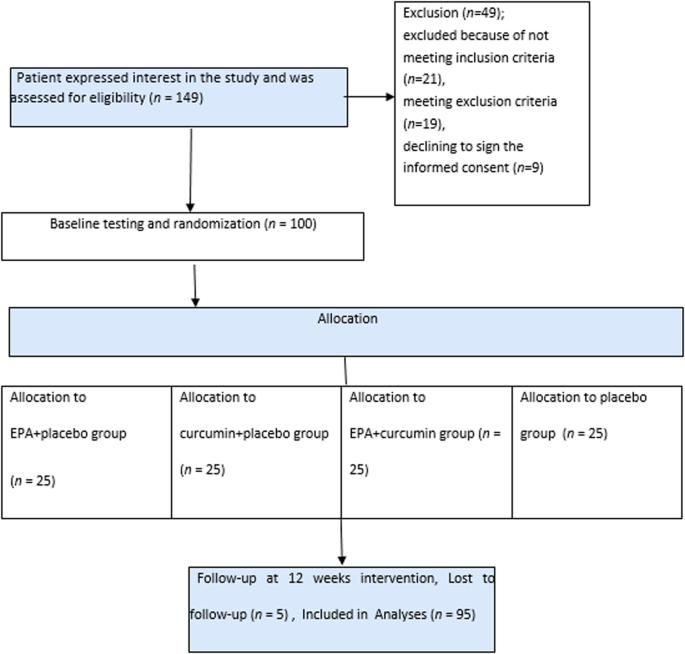
Statistical analysisAll analyses accounted for the complex survey design and sampling weights using Stata version 14.2 (Stata Corp, College Station, Texas). Of the 16,415 adults at baseline, we excluded participants with diabetes at baseline (n = 3420), no follow-up visit (n = 3913), fasted <8 h prior to either visit (n = 49), did not have two 24 h dietary recalls with plausible energy values (kcals > 500 or kcals<5000; n = 819), self-reported more than one or “other” heritage (n = 238) and had missing data on heritage (n = 7), insulin (n = 152) and other covariates (n = 43), yielding a final sample size of 7774 (Fig. 1, flowchart).
Fig. 1: Flowchart of heritage-specific analytic samples by insulin resistance status at 6 years in HCHS/SOLa.
aHispanic Community Health Survey/Study of Latinos, HCHS/SOL.
We tested differences in sociodemographic and health characteristics by heritage using analysis of variance for continuous variables and Pearson chi-square for categorical variables. We then tested mean differences in AHEI-2010 score by quintiles of each DP to assess correlations with a measure of diet “healthfulness” using linear regression, adjusting for age, sex, and education. To prospectively evaluate associations between baseline DPs and IR status, we used multivariable multinomial logistic regression to estimate 6-year log-odds (likelihood) of worsened and improved (versus unchanged) insulin levels comparing highest-to-lowest quintiles of DPs in each heritage group. We used multivariable logistic regression to assess relationships between DPs and incident diabetes (cumulative incident proportion). Model 1 adjusted for elapsed time between visits and baseline covariates, including age, sex, education, nativity, total energy intake, natural log of fasting insulin (except incident diabetes models), and physical activity. Estimates did not change when we also adjusted for smoking status, thus, it was not included in final models (data not shown). To better understand the direct contributions of diet on the outcomes independent of central adiposity, Model 2 was further adjusted for WC. Because participants with incident diabetes may have been taking antidiabetic medications at visit 2, impacting insulin levels, we performed a sensitivity analysis excluding participants taking antidiabetic medication at either visit (n = 10). Finally, to assess potential for selection bias, we conducted sensitivity analyses by testing baseline sociodemographic and AHEI-2010 score differences between our analytic sample and participants without baseline diabetes who were excluded from our analysis. Ptrend values were calculated by including the midpoint of each quintile of each dietary pattern as a continuous variable (score units). We set statistical significance at p < 0.05.
留言 (0)