
記住我

We reviewed the medical records for patients who underwent IVF/intracytoplasmic sperm injection (ICSI)-ET treatment between January 2014 and December 2018 in the Reproductive Medical Center of Jiangxi Provincial Maternal and Child Health Hospital. The inclusion criterion was IVF/ICSI-ET treatment with the GnRH-a prolonged protocol; the exclusion criteria were cycle cancellation before oocyte pick-up (OPU); lack of oocyte retrieval after OPU; oocyte donation, sharing, and cryopreservation; frozen oocyte thawing; and preimplantation genetic testing. We excluded patients with the following current conditions: uncontrolled diabetes; hepatic or renal dysfunction without a definite clinical diagnosis; history of deep-vein thrombosis; history of pulmonary embolism; history of cerebrovascular events; uncontrolled hypertension; heart disease; suspicion of cervical, endometrial, or breast cancer; or unexplained vaginal bleeding.
We collected data from the clinical records for the following demographic and clinical characteristics: age; body mass index (BMI); antral follicle count (AFC); duration, type, and cause of infertility; basic hormone levels; Gn dose; days of ovarian stimulation; the number of oocytes retrieved; type of insemination; two-pronuclear zygote fertilization rate; the number of embryos transferred in the fresh-ET cycle; the number of transferable embryos; rate of moderate-to-severe OHSS; cycle cancellation rate; embryo implantation and abortion rates; and LBR and CLBR. The primary outcome was the number of oocytes retrieved.
Treatment protocolGnRH-a prlonged and embryo freezing protocolWe performed COS using an GnRH-a prlonged protocol. Patients received a single dose s.c. injection of 3.75 mg GnRH-a (long-term-acting disheveling; Beaufour Ipsen, Dreux, France) on Day 2 ~ 3 of the cycle, after the ultrasound scan confirmed ovarian quiescence and the presence of a thin endometrium (< 5 mm). When complete pituitary desensitization was achieved (28 days after the initiation of GnRH-a), with a low plasma E2 level of ≤ 30 pg/ml and an LH level of ≤ 2 IU/l, COS was started. For every individual, we selected the dosage of stimulating Gn based on age, AFC, basal FSH, BMI, and previous ovarian response [30, 31]. During stimulation, we monitored the ovarian response through assessments of serum E2, progesterone (P), and LH, as well as serial transvaginal ultrasonographic examinations. We would adjust the Gn doses when needed.
On identification of at least one follicle with a diameter ≥ 19 mm or two follicles with diameters ≥ 18 mm, we administered 250 μg of recombinant human choriogonadotropin (hCG [Ovitrelle]; Merck Serono, Corsier-sur-Vevey, Switzerland) subcutaneously. We performed oocyte retrieval 36 h after injection of hCG using a transvaginal ultrasonography-guided puncture of the follicles. Semen was produced by masturbation, and motile spermatozoa were prepared by density gradient centrifugation and the swim-up procedure. We initiated luteal support after OPU using intramuscular injection of P (80 mg/day). Type of insemination included IVF, ICSI, and early-rescue ICSI. All the oocytes were inseminated 4–5 h after collection, fertilization was initially assessed 5 h after IVF insemination, and if the oocytes had not been fertilized at this point, early-rescue ICSI was performed immediately.
We selected the highest quality embryos, consisting of 7–9 blastomeres of uniform size and with a fragment proportion < 20% [32], for embryo transfer or cryopreservation on Day 3 after fertilization. We evaluated individuals with ≥ 15 retrieved oocytes on the day of embryo transfer for ovarian diameter ≥ 7 cm and/or reported abdominal distension or bloating, which are indications for embryo cryopreservation, to avoid moderate-to-severe OHSS. All these embryos were cryopreserved by vitrification using the Cryotop system [33].
The preparation of the endometriumAll FET cycle individuals were divided into three groups, the natural cycle, the HRT cycle, and the GnRHa-HRT cycle, for the preparation of the endometrium. The natural cycle was suitable for individuals who have regular menstrual cycles and can ovulate normally. According to the length of the patient's menstrual cycle (21–35 days), the follicle and endometrium are monitored by B-ultrasonography from the middle follicular phase. When the diameter of the follicle reaches 14-15 mm, the B-ultrasonography and serum LH and E2 levels are monitored every day until the day of ovulation. The natural cycle recommends LH peak + 4d (D3 cleavage-stage embryo) or LH peak + 6d (D5 blastocyst) as the timing of embryo transfer. To improve the natural cycle, when the diameter of the dominant follicle is more than 16 mm and the intima thickness exceeds 7-8 mm, hCG can be used clinically to replace the endogenous LH peak to induce ovulation, and then arrange the timing of embryo transfer. It is recommended that hCG injection day + 5 days (D3 cleavage stage embryos) or HCG injection day + 7 days (D5 blastocysts) as the timing of embryo transfer. The HRT cycle was suitable for individuals with ovulation disorders or irregular menstruation. It can also be used for patients with regular menstruation but periodic monitoring of anovulation, or patients who are inconvenient for frequent trips to the hospital to monitor ovulation. The Estrogen was begun to use at 2–3 days later of menstrual cramps. The estrogen administration route of administration includes oral, vaginal suppository, and transdermal absorption. A fixed regimen (oral dose 6 mg/d) or incremental regimen (usually 1–4 days, 4 mg/d; 5–8 days, 6 mg/d; 9th day, monitor the endometrial thickness, if > 7 mm, maintain 6 mg/d, if < 7 mm, increase the amount to 8 mg/d) can be used. The GnRHa-HRT cycle was used for endometriosis, adenomyosis, thin endometrium, unexplained repeated implantation failure, polycystic ovary syndrome, pelvic surgery history, or menstrual high progesterone. GnRH-a (3.75 mg) was used on individuals every 28 days starting on the 2-3th day of menstruation. According to the individuals’ specific situation can be injected 1–6 times, 28 days after the last injection to review endocrine hormone levels and transvaginal B-ultrasonography, blood hormone levels reached the standard after entering the cycle, estrogen supplement with HRT cycle.
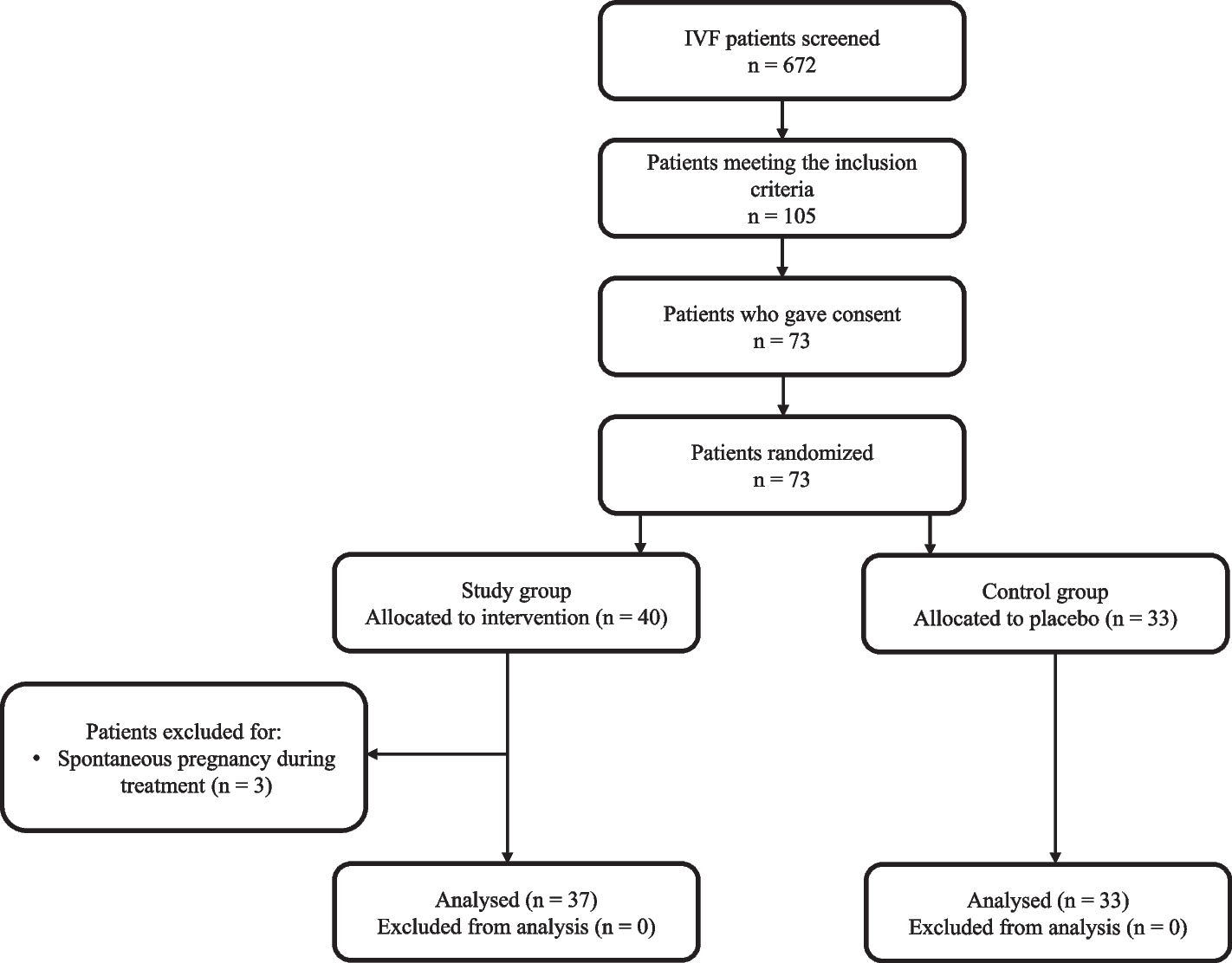
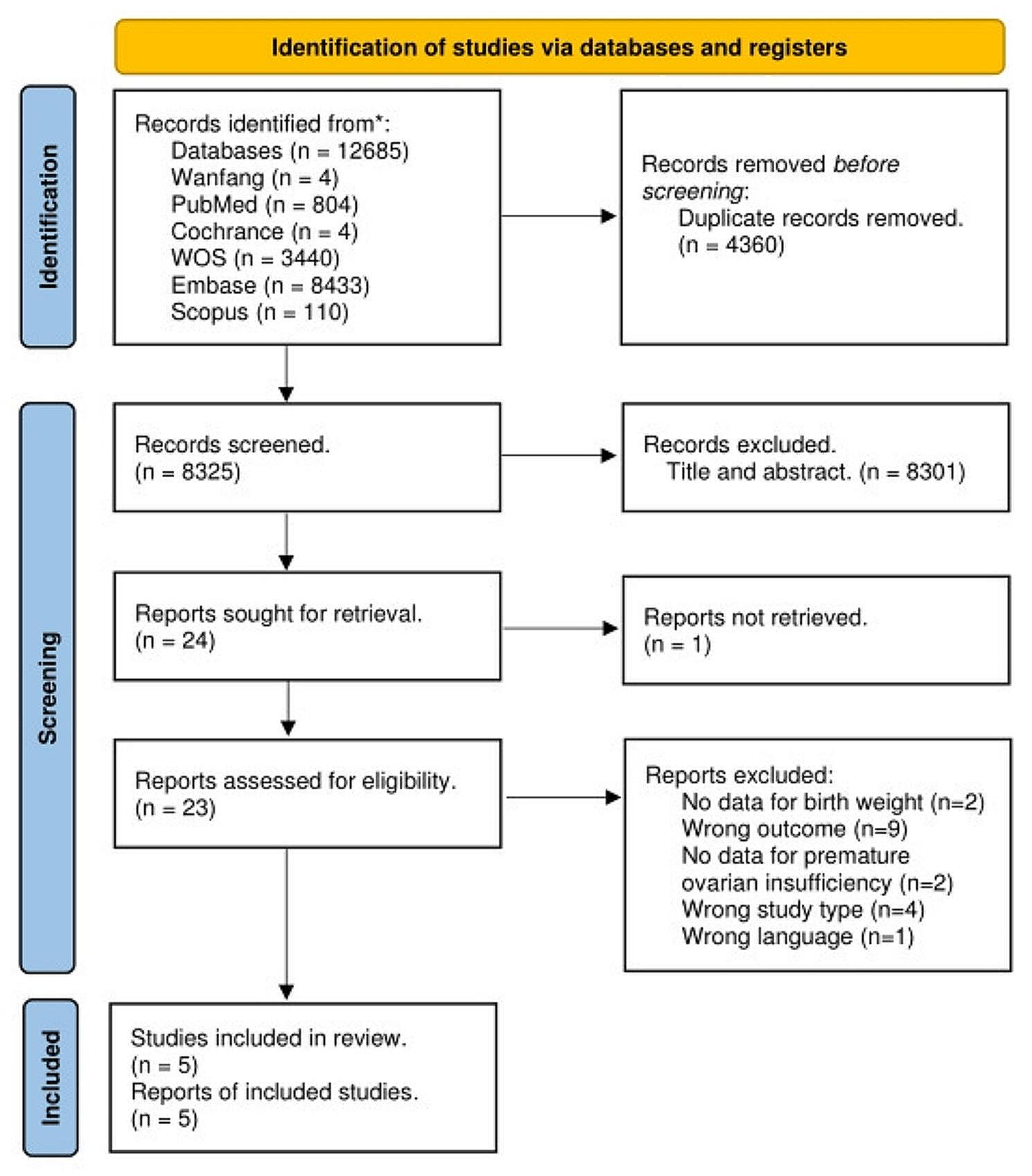
Embryos transferThe number of embryos transferred (≤ 2 per patient) complied with the national regulations in China and conformed to individual patient requests. We evaluated individuals with ≥ 15 retrieved oocytes on the day of embryo transfer for ovarian diameter ≥ 7 cm and/or reported abdominal distension or bloating, which are indications for embryo cryopreservation, to avoid moderate-to-severe OHSS. In the few patients who had indications for blastocyst transfer [34], we performed embryo transfer on Day 5. We categorized blastocyst quality as excellent (AA), good (AB, BA, BB), fair (BC, CB), or poor (CC) based on trophectoderm and inner-cell-mass quality scores [35]. We supported the luteal phase through the daily intravaginal administration of 90 mg of P gel (Crinone gel 8%; Merck Serono) and of 20 mg dydrogesterone (Duphaston 10 mg/tablet; Solvay Pharma, Weesp, Netherlands) after embryo transfer. We assessed reproductive outcome 2 weeks after embryo transfer testing for hCG; then at gestational Weeks 7–9, when a positive assessment was deemed a clinical pregnancy; and finally at delivery, when the measured outcome was live birth. We defined positive hCG as plasma hCG > 5 IU/L and clinical pregnancy as detection of a gestational sac and a heartbeat, verifying a living fetus using ultrasonography. We defined live birth as at least one living child from the fresh ET, irrespective of the duration of gestation. The CLBR corresponded to the results of all treatments from one complete cycle, including all fresh and frozen-thawed ET cycles from one oocyte retrieval, over 2 years. The follow-up period was 2 years. We maintained luteal support until 10 weeks of pregnancy. We recorded pregnancy complications, as well as neonatal birth weight and complications at delivery. A flow chart of the consecutive analysis steps is depicted in Fig. 3.
Fig. 3
The flow chart of the consecutive analysis steps
Statistical analysisWe analyzed the data using the statistical software SAS, version 9.4 (SAS Institute, Cary, NC, USA). We compared continuous variables using analysis of variance (ANOVA), summarizing them as mean ± standard deviation (x̄ ± SD). We summarized the data that did not fit a normal distribution by the median (interquartile range [IQR]). We determined the count data adoption rate (%) using a chi-square test. We used logistic regression for multivariate analysis, setting the test level α to 0.05 and considering P-values < 0.05 as statistically significant.
留言 (0)