
記住我










Obsessive-compulsive disorder (OCD) is a complex neuropsychiatric illness characterised by intrusive and persistent obsessive thoughts along with dysfunctional and ritualised behaviours.1 The disorder often begins in childhood, puberty, or early adulthood and thus affects a critical period of development.2 OCD can be a debilitating disease with many patients experiencing severe comorbid depressive and anxiety disorders as well as the inability to work or attend school.3 The lifetime prevalence of OCD in the general population is 1%–3%, and while 50%–70% of patients can significantly improve with conventional therapies including pharmacotherapy and cognitive–behavioural therapy with exposure and response prevention (ERP), at least 10% of patients will develop severe symptoms refractory to multimodality therapy.1 3
Well-established surgical methods to address treatment-resistant OCD (TROCD) symptoms include various forms of ablative lesioning such as anterior cingulotomy and anterior capsulotomy and have been practised since the 1950s.3 4 Over the last two decades, deep brain stimulation (DBS) has emerged as a viable method to treat TROCD, offering an adjustable and partially reversible alternative to ablative techniques, with a similar reported efficacy.5 6 The first reported case of DBS for OCD involved targeting of the anterior limb of the internal capsule (ALIC) based on the authors’ previous experiences with anterior capsulotomies.1 7 8 Since the first sham-controlled randomised trial targeting the ALIC in 2005,9 a multitude of trials have been conducted with varying surgical targets, methodologies and reported outcomes.10 DBS for TROCD at the ALIC was granted a humanitarian exemption by the US Food and Drug Administration in 2009.1 A variety of white and grey matter areas including ALIC, subthalamic nucleus (STN), ventral capsule/ventral striatum (VC/VS), bed nucleus of stria terminalis (BNST) and nucleus accumbens (NAc) have been targeted surgically, as all are theorised to share important roles in regulating mood, reward-learning and decision-making within the hypothesised cortico-striato-thalamo-cortical (CSTC) circuit.11 More recently, it has been described that the various striatal areas targeted in TROCD DBS are likely modulating similar CSTC and orbitofrontal networks and that a conserved pathway is implicated in optimal symptom improvement across targets.11 12
In the evolving field of DBS for TROCD, a better understanding of treatment efficacy across studies with varying methodological designs is desired. To date, several meta-analyses have synthesised the body of evidence on DBS for OCD.13–16 However, since the most recent publication, one novel randomised controlled trial (RCT)17 and at least six observational cohort studies have been published.18–23 In addition, previous studies have not attempted to quantitatively assess bias in outcomes reporting which may improve confidence in the reported results of variously powered and designed studies. In light of this, we present here a systematic review and meta-analysis with the objective of critically assessing the efficacy of DBS in alleviating OCD and comorbid depressive symptoms across targets in patients with TROCD.
MethodsA systematic review was completed using 2020 Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. PubMed and EMBASE databases were queried using advanced search strategies including Medical Subjet Headings (MeSH) terms in PubMed—“Deep Brain Stimulation”[Mesh] AND “Obsessive-Compulsive Disorder”[Mesh] OR ((“OCD” OR “obsessive-compulsive disorder”) AND (“DBS” OR “deep brain stimulation”))—and an exhaustive set of terms in EMBASE including (‘OCD’ OR ‘obsessive-compulsive disorder’/exp OR ‘obsessive-compulsive disorder’ OR ‘TROCD’) AND (‘DBS’ OR ‘brain depth stimulation’/exp OR ‘brain depth stimulation’ OR ‘deep brain stimulation’/exp OR ‘deep brain stimulation’). The search was completed through September 2021.
Selection criteriaStudies were included if they met the following criteria: (1) subjects were human adults (age >18 years) with a primary diagnosis of OCD according to the Diagnostic and Statistical Manual of Mental Disorders Fourth or Fifth edition (DSM-IV or DSM-V) or International Classification of Diseases criteria; (2) DBS was the primary intervention; (3) primary outcome was improvement in clinical OCD symptoms after DBS; (4) outcome was assessed using the Yale-Brown Obsessive Compulsive Scale (Y-BOCS); (5) treatment response was defined as a ≥35% reduction in Y-BOCS score; (6) published in English in peer-reviewed journals.
Studies were excluded according to several criteria: (1) reviews, meta-analyses, comments, letters and editorials lacking de novo patients; (2) single case reports; (3) studies investigating neuroimaging, neuropsychiatric, behavioural, and/or electrophysiological changes after DBS as primary outcomes; (4) animal studies; (5) studies focusing on non-OCD indications for DBS; (6) technical reports on the safety or procedural aspects of DBS for OCD.
Selection processAll search results from both PubMed and EMBASE databases were exported to a spreadsheet and duplicates were removed. Studies were excluded using automated detection tools in Excel 2016 (Microsoft Corporation, Redmond, Washington, USA). Two reviewers independently screened the title of each record retrieved. One reviewer screened the abstracts and full texts of all remaining records and reports for eligibility and final inclusion. In any case where several records reported on all or part of the same cohort of patients, the study with the most detailed dataset for the largest number of patients was selected for inclusion.
Data collection and organisationThe following data items were collected where available:
General study information including study location, first author, publication year, study design, patient inclusion and exclusion criteria, sample size, treatment response criteria, response rate, and rates of complications or adverse events.
Patient-level data including stimulation target(s), primary diagnosis, patient sex, age at onset of OCD, age at DBS surgery, comorbid psychiatric diagnoses, active medications, preoperative/baseline Y-BOCS scores, all follow-up Y-BOCS scores (with time points in months), per cent Y-BOCS score reduction at last follow-up, length of follow-up (in months), DBS stimulation parameters (amplitude, pulse width, frequency, contact configuration, polarity), quality of life outcomes, baseline depression scale (Hamilton Depression Rating Scale (HAM-D, HDRS-17, HDRS-24), Montgomery-Åsberg Depression Rating Scale (MADRS), Depression Anxiety Stress Scale-Depression (DASS-21-D) and Beck Depression Inventory (BDI)), baseline anxiety scale (Hamilton Anxiety Rating Scale (HAM-A and HARS), State-Trait Anxiety Inventory (STAI-1/X1 and STAI-2/X2), DASS-Anxiety (DASS-21-A) and Beck Anxiety Inventory), and baseline Global Assessment of Functioning (GAF) scores and all follow-up scores.
If patient-level data were not available, pooled means were collected. All data were manually recorded in a single spreadsheet by two reviewers who worked in conjunction.
Risk of bias assessmentTwo reviewers completed all risk of bias (RoB) assessments independently. For RCTs, the revised Cochrane tool for assessing risk of bias in randomised trials24 was used to critically evaluate six domains of bias: randomisation, period/carryover (for crossover trials), assignment to intervention, missing outcome, outcome measurement and selection of reported results. Non-RCTs were assessed using Cochrane’s Risk Of Bias In Non-randomized Studies-of Interventions25 which examines seven domains of bias: confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes and selection of the reported results. All bias assessments were performed by two authors who were blinded to each other’s ratings. Following individual assessment, incongruencies were mediated and results were aggregated and visualised using the RoB visualisation web app robvis.
Meta-analytical methodsMeta-analysis was performed with the meta package (RRID: SCR_019055) using R statistical computing software (R Core Team, 2021). Primary outcome measures were (1) Y-BOCS mean difference at last follow-up compared with baseline, (2) treatment effect, or Y-BOCS per cent reduction, at last follow-up, and (3) responder rate at last follow-up. Secondary outcomes included (1) standardised mean difference (SMD) in depression scale scores and (2) depression scale responder rate, defined as >50% reduction in depression scores.26 As different studies used varying scales (ie, MADRS, HDRS, BDI) to assess depression preoperatively and postoperatively, SMD was calculated using the Hedges’ g statistic, which is a commonly used method to compare depression scales,26 27 to determine a treatment effect size corrected by pooled sample variance across studies. A g of <0.2 indicates a small effect, 0.5–0.8 indicates a medium effect and >0.8 indicates a statistically large effect.27 Both fixed and random-effects models were used to synthesise primary and secondary outcomes and assess the relative effects of smaller studies compared with larger ones. The DerSimonian-Laird method was used to assess between-study variance (τ2) and I2 was used to determine the fraction of the variance due to various forms of study heterogeneity (eg, statistical, clinical, methodological).28 Funnel plot analysis was performed to evaluate small study effect biases and symmetry was quantitatively assessed using the Thompson-Sharps test for asymmetry.28 Subgroup analysis was performed on RCTs and non-RCTs to determine possible causes of outcome heterogeneity.28 Furthermore, meta-regression was performed on primary outcome measures using the model sum of square statistic (QM) covariated by reported target as well as by target grouped into striatal versus non-striatal groups as per recent nomenclature recommendations.1 In all analyses, a multicomparison-adjusted p<0.05 was considered statistically significant.
ResultsStudy selectionOur search strategy yielded a total of 3023 records (PubMed=841, EMBASE=2182) from 1986 to 2021. Thirty-four studies (n=352) from 2005 to 2021 were selected for systematic review and meta-analysis, including 9 RCTs (n=97)9 17 29–34 and 25 non-RCTs (n=255).18–23 35–53 For more information on our search and selection process, see the PRISMA flow chart (figure 1).
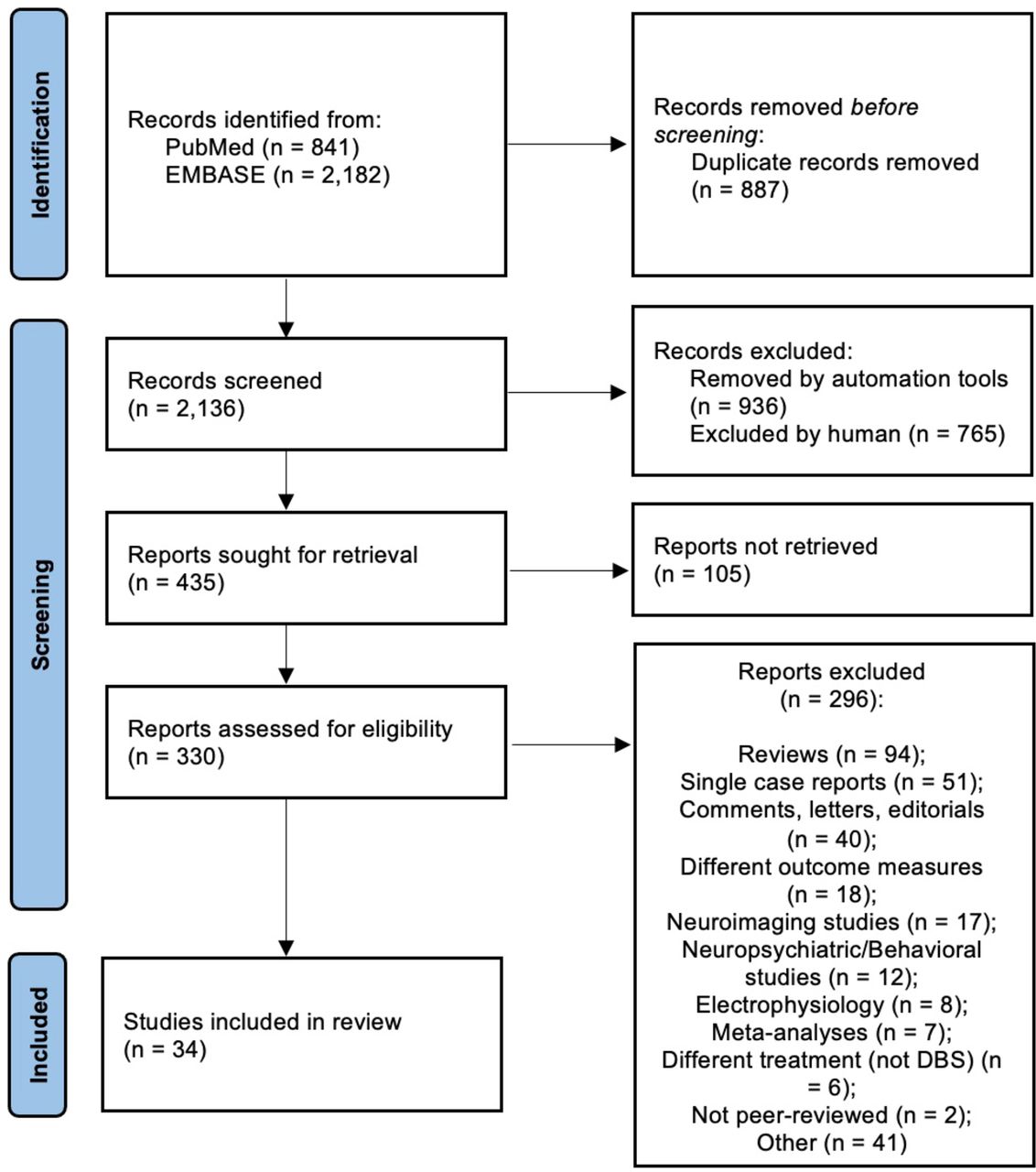 Figure 1
Figure 1 2020 PRISMA flow diagram. DBS, deep brain stimulation; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Study characteristics: demographics and inclusion criteriaAcross the 34 included studies, all 352 subjects were adults (mean age 40.8±10.8 years; range 18–64) with severe to extreme OCD (mean Y-BOCS 33.5±3.6, range 20–40) at baseline, who had completed ~3 first-line pharmacotherapy trials (range 2–6), 1 adjunctive medication trial and ~20 hours of expert ERP (range 12–45) without sustained treatment response. Additionally, in 67% (23 of 34) of studies, patients were required to have an unremitted disease duration of ≥5 years before consideration for surgery. Of the remaining 11 studies, 1 had a requirement of >10 years of disease duration and ≥2 years of unremitted disease,54 another only required ≥1 year of unremitted disease19 and 5 did not specify.9 30 35 36 53 Four studies did not report any inclusion criteria.22 39 43 44 Average disease duration was 24.3 years (±10.5; range 5–51). Psychiatric comorbidities, reported in 23 studies (n=231), included: major depressive disorder in ~55% of patients, anxiety disorder (eg, generalised anxiety disorder or panic disorder) in 10% and a personality disorder in 9.5%. The median number of participants in RCTs was 10 (IQR 7–16; range 4–16) while for non-RCTs it was 7 (IQR 4–11; range 2–54). Median follow-up was 24 months (IQR 12–32; range 6–80). For individual study characteristics, see online supplemental table 1.
Study characteristics: targets and stimulation parametersThe most common described stimulation targets were VC/VS (six studies, n=63)18 35 37 40 52 55 and NAc (six studies, 53 patients)31 32 34 41 46 48 followed by ALIC (four studies, n=100),9 30 45 51 BNST (four studies, n=28),17 21 41 46 STN (three studies, n=47)29 44 53 and ALIC/BNST (three studies, n=37).19 30 33 Other described target combinations included: NAc+VS+internal capsule (n=14),23 inferior thalamic peduncle (n=11),38 47 anteromedian STN+VC/VS (n=6),54 caudate nucleus (n=5),34 medial dorsal and ventral anterior nucleus of the thalamus (MD/VA) (n=4),42 superolateral branch of the medial forebrain bundle (n=2),43 STN+NAc (n=2),39 VS/ALIC (n=2),49 ALIC/NAc (n=2)50 and BNST/NAc (n=1).46 Leads were implanted bilaterally in all cases except in one double-blind, sham-controlled RCT, which specifically targeted the right NAc (n=10).
Study characteristics: depression, anxiety and functional outcomes reportingFourteen studies used a Hamilton depression scale (nine HAM-D and five HDRS),9 23 30 32 33 35–37 39–41 47 50 51 seven studies used BDI,19 20 31 34 42 48 49 five studies used MADRS18 21 22 29 54 and one used the DASS-D46 to assess depression preoperatively and postoperatively. Of the 16 studies that reported anxiety scores, 11 used a Hamilton anxiety scale (9 HAM-A, 2 HARS),9 22 29 30 32–35 39 50 51 4 used STAI-X1/220 31 42 48 and 1 used DASS-A.46 Seventeen studies reported GAF scores; however, seven of these studies only reported baseline scores.
Study characteristics: safetyApproximately 70% of studies (24 of 34; n=249) reported complete data on serious adverse events (SAEs), including, but not limited to: hardware-related complications, infections, seizures, suicide attempts, intracranial haemorrhage (ICH) and the development of de novo obsessions associated with stimulation. Overall, ~31% of patients (n=78) experienced at least one SAE. Incidence of device-related complications, that is, lead damage or malposition, was ~8% (n=20). There were 11 cases of postoperative infection (~4.4%)—of which 6 required explantation and/or replacement of a pulse generator—and 9 instances of postoperative seizure (~3.6%). One patient (included in both infection and seizure groups) experienced several SAEs, including a generalised tonic–clonic seizure, intracranial infection, shock and a pharmacologically induced coma.18 Additionally, there were six cases of attempted suicide (~2.4%) and one completed suicide (0.4%). Studies reported five cases of postoperative ICH (~1.6%), of which one resulted in prolonged finger palsy29 and another resulted in prolonged dysarthria.53 Finally, in two cases (0.8%), DBS therapy itself became the source of a new obsession (eg, checking settings and battery life), which contributed to worsening OCD.40 47 For a full list of reported complications and adverse events, see online supplemental file A.
RoB within studiesIn RCTs, RoB in randomisation, missing outcomes and selection of reported results was found to be low in all studies. RoB in assignment to intervention and outcome measurement was low in most studies but uncertain in several due to unblinding of investigators secondary to adverse events during the trial period. Three of the nine RCTs included dedicated washout periods from stimulation ON to stimulation OFF arms and thus incurred a low RoB in this domain.9 29 34 One study, which did not have a washout period in its design, tested specifically for carryover effects and found none, thus incurring a low RoB.32 Four others, which included neither washout periods nor any structured analyses testing for carryover effects, prompted an unclear RoB designation.30 31 33 54 The most recent RCT was a parallel-arm non-crossover study.17 Of the non-RCTs, nearly all studies demonstrated low-moderate RoB in participant selection, intervention classification, intended intervention deviation, missing data, outcome measurement and selection of reported results. Approximately one-third of studies demonstrated a low RoB due to confounding, while the other two-thirds had a moderate-high RoB due to confounding. This risk was most often related to within-study variability in target implanted, length of follow-up or baseline OCD severity/phenotype. See figure 2 for full RoB assessments of RCTs and non-RCTs.
 Figure 2
Figure 2 Risk of bias assessments. (A) Individual RCT Cochrane RoB 2 breakdown and (B) summary of RCT assessments. (C) Individual Cochrane ROBINS breakdown for non-RCTs and (D) summary of non-RCT assessments. RCT, randomised controlled trial; RoB 2, Cochrane tool for assessing risk of bias in randomised trials; ROBINS, Risk Of Bias In Non-randomized Studies.
Synthesis of resultsThe meta-analytical Y-BOCS mean difference (MD) at last follow-up was 14.28 (95% CI 12.51 to 16.05) points across 345 patients pooled from 31 studies (figure 3A). Three of the 34 studies were excluded from MD meta-analysis as they did not report individual Y-BOCS scores both preoperatively and postoperatively.39 45 49 Using available pre-disambiguated and post-disambiguated data, the meta-analytical treatment effect (TE) was found to be a 47% (95% CI 40% to 53%) reduction in Y-BOCS scores at last follow-up across 249 patients from 28 studies in which precision estimates could be gathered or measured (figure 3B). The responder rate (RR) at last follow-up was found to be 66% (95% CI 57% to 74%). Both Y-BOCS MD and TE demonstrated pooled statistical significance (p<0.01). There was, however, statistically significant between-study variance in both measures with between 70% and 84% of the variance arising due to study heterogeneity.
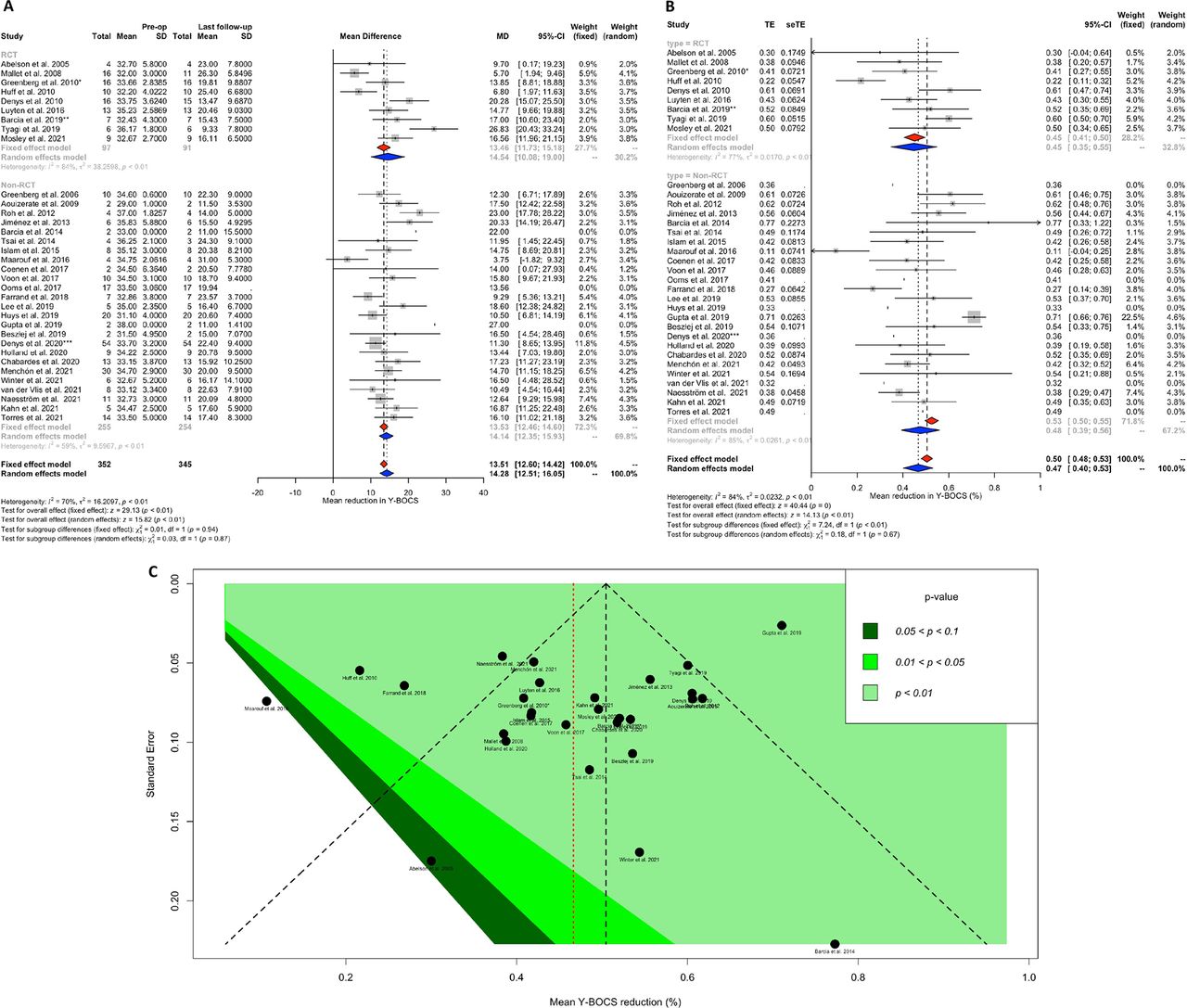 Figure 3
Figure 3 Y-BOCS forest and funnel plots across all included DBS for OCD studies. (A) Y-BOCS mean difference (MD) data summarised from 31 studies, n=345. (B) Y-BOCS treatment effect (TE) data summarised from 28 studies, n=249. (C) Funnel plot demonstrating distribution of treatment effects against SE. Relative symmetry of distribution can be seen with most studies demonstrating strong TEs by varying levels of significance (colour contoured). DBS, deep brain stimulation; OCD, obsessive-compulsive disorder; RCT, randomised controlled trial; Y-BOCS, Yale-Brown Obsessive-Compulsive Scale.
Funnel plot analysis was performed on TE data. The relative symmetry of the dispersion of SE plotted against treatment effect along with the finding that larger studies tended toward lower errors while smaller studies tended toward larger errors suggests low risk for small study effects bias (figure 3C). Twenty-seven of 28 studies achieved statistically significant TEs (p<0.05). The lone study that reported non-significant effects (p>0.1) was the only one to target MD/VA thalamus.42 Furthermore, a Thompson-Sharps test for funnel plot asymmetry demonstrated random dispersion of TE relative to SE indicating a low risk for between-study heterogeneity due to small study effects bias (t=1.11, df=19, p=0.2814) (online supplemental file B). Subgroup analysis by methodology demonstrated no significant differences between RCTs and non-RCTs in any primary outcome measure by random-effects modelling (MD p=0.87, TE p=0.67, RR p=0.61). Meta-regression of Y-BOCS outcomes by striatal versus non-striatal targets (QM(df=2)=1.92, p=0.385), as well as across various reported targets (QM(df=13)=19.99, p=0.095), demonstrated no significant difference. Interestingly, studies explicitly targeting NAc (adjusted p<0.05) and MD/VA (adjusted p<0.01) did report Y-BOCS effects of lower magnitude than other reported targets.
Raw mean reduction in depressive symptoms was 7.15 points (95% CI 4.82 to 9.47) or 40% (n=140) with HDRS, 11.89 points (95% CI 2.66 to 21.13) or 41% (n=68) with MADRS, and 8.43 points (95% CI 4.80 to 12.05) or 32% (n=57) with BDI. Using pooled mean averages and variances, overall SMD calculation yielded an approximate 1 standardised effect size (Hedges’ g) reduction in depressive scale scores (95% CI 0.67 to 1.32) (figure 4). Of note, there was a significant difference between studies using HDRS or MADRS compared with those using BDI, whereby those using the latter reported a less significant effect size (χ2=8.89, df=2, p=0.01). Using available reported data at last follow-up, we found that 47% of patients were considered full responders relative to their preoperative/baseline comorbid depression. An additional 16% of patients were considered partial responders (30%–49% reduction in pre/post-treatment depressive symptoms) and 37% were considered non-responders (<30% reduction).
 Figure 4
Figure 4 Standardised mean difference (SMD) in depression scores from studies using HDRS, MADRS and BDI scales. Overall standardised effect size (Hedges’ g) of 1 indicating a strong effect of comorbid depressive symptom reduction at last follow-up. BDI, Beck Depression Inventory; HDRS, Hamilton Depression Rating Scale; MADRS, Montgomery-Asberg Depression Rating Scale.
DiscussionWe report the largest meta-analysis of efficacy and mood response data concerning the use of DBS for TROCD to date. Our results indicate that patients with severe TROCD experience a near 50% reduction in their OCD symptoms by a median follow-up of approximately 24 months. Sixty-six per cent of patients in well-designed studies achieved response to DBS therapy, which compares with or outperforms recent estimates of treatment response with lesional procedures (36%–59%).56 A relatively recent review compiled data in order to compare the outcomes and complications of anterior capsulotomy versus DBS of the VC/VS or NAc for OCD and found that both procedures carry similar risk–benefit profiles.57 We found a strong effect of DBS for TROCD on comorbid depression, with nearly half of reported patients attaining a complete response and an additional 16% at least partially responding to therapy.
A previous meta-analysis of a smaller set of DBS for TROCD data found a correlative effect between Y-BOCS and depression response.13 A potential and intuitive explanation for the strong co-therapeutic effect seen in our and previous results is that the more a patient’s OCD symptoms improved, the more positive the effect was on their mood. The same study found that illness severity at baseline was a negative predictor of treatment response at last follow-up.13 Their results give credence to the idea that studies that enroll patients with overly variable illness severities assume a potential risk of variability in results that can be avoided by further narrowing severity inclusion criteria. Additionally, our finding that NAc targeting resulted in lower magnitude effects supports the idea that the optimal target is not grey matter (NAc/VS) but rather white matter. This observation reinforces the developing idea that optimal targeting requires engaging a network of regions via cortical white matter hubs.11 58
Of the nine RCTs included, only three had a washout period. In a crossover study, the washout period should be of sufficient duration to eliminate carryover effects (ie, the treatment effects from a stimulation ON period carrying over into a stimulation OFF period, resulting in an underestimation of the overall treatment effect). The absence of a washout period is thus a potentially significant source of bias. RCTs included in our meta-analysis had stimulation periods ranging from 2 weeks to 3 months. In the case of the study using 2-week crossover periods (ON/OFF), despite the lack of washout, the investigators found no significant carryover effects.32 One explanation for this is that 2 weeks of stimulation is likely not long enough to significantly alter the circuits implicated in OCD. On the other hand, for the four RCTs with a 3-month crossover design, the likelihood of carryover effects is much higher after a 3-month stimulation period, and so the washout period omission should be considered when interpreting results.
For non-RCTs, two-thirds of those included in our meta-analysis carried a moderate-high RoB due to confounding. The most prominent confounder in this group of studies was the deviation of inclusion criteria from strict, commonly accepted standards. For example, two non-RCTs included patients with hoarding disorder.51 52 Hoarding is a ‘phenotype’ that has lacked a pronounced response to DBS in multiple trials.59 This disorder has also recently been removed as a subtype of OCD in the DSM-V and thus will not be included in future studies. There may yet still be other phenotypes that may warrant exclusion from trials studying DBS for OCD in order to redirect therapy away from indications that will not respond. Similarly, several non-RCTs included patients with a host of typically excluded comorbid diagnoses, such as: borderline personality disorder,42 51 autism spectrum disorder,22 51 substance use disorders22 38 and bipolar 1 disorder,40 41 51 among others. While in day-to-day life, many patients with TROCD often have these and other comorbid conditions, when designing studies with the goal of reporting TE, it would be useful to reduce or control for these sources of biases. In addition, patients in non-RCTs had more variable follow-up periods (range 6–72 months) with many patients having less than 12–18 months of follow-up. Patients undergoing DBS for OCD have been shown to derive maximal symptom improvement with prolonged follow-up and this may also confound the pooled TE between studies.53 A recent follow-up study by the pioneering group from Amsterdam recapitulates this point by reporting a highly maintained response for both OCD and mood symptoms at prolonged mean follow-up (6.8±3 years) with improvement in functioning and overall well-being.60
Small study effects is a term for the phenomenon that smaller studies sometimes show different, often more pronounced, TEs than larger ones.61 One well-known potential reason for this is publication bias in which the chances of a smaller study being published increase if that study shows a stronger effect.61 A significant limitation of prior meta-analyses of the DBS for OCD literature is that none have attempted to assess these types of biases, which are known to lead to caution in interpreting medical literature.28 61 Other possible causes for small study effects include outcome reporting bias and clinical heterogeneity between patients in large and small studies. Our sensitivity analyses show that small study effects do not significantly impact the aggregate TE across studies and centres. A lack of significant differences between fixed and random-effects estimates of outcome measures is another encouraging sign that small study effects do not significantly bias the reported results.28 As most prior studies of DBS for TROCD have involved smaller sample sizes, such factors merit consideration when interpreting published outcomes available in the literature.
While these results are encouraging, it is important to remember that DBS is not without its limitations. First and foremost, it requires chronic implantation of hardware and carries the associated risk of complications. Our study shows a rate of hardware-related complications of ~8%. Additionally, we report a pooled infection rate of ~4.4%, a finding which aligns closely with a recent meta-analysis showing a surgical site infection rate of 5% in DBS all-comers and 4.5% specifically in DBS for OCD.62 Furthermore, although we report a less than 1% incidence of de novo obsessions involving the DBS patient programmer or the device itself, it remains a significant barrier to the effective implementation of DBS for OCD in certain patients; one which future studies could investigate further to define predictors of such behaviour. In addition, there is currently a need for pulse generator replacement after approximately 18 months for non-rechargeable models or up to 9 years for rechargeable models.52 Finally, successful application of DBS requires a close therapeutic alliance between patient, neurosurgical and expert psychiatrist teams in centres that specialise in implantation and programming of the device.
In sum, our findings support DBS as an effective treatment for TROCD, and the average appropriately selected patient will experience OCD symptom reduction of about 50%. Two-thirds of patients will achieve at least full response to DBS therapy with sustained follow-up. Stimulation of current limbic and non-limbic targets can provide substantial relief of comorbid depressive symptoms in TROCD. The growing evidence base reporting DBS for OCD outcomes demonstrates a predominantly low RoB across studies. Future crossover RCTs should aim to consistently include washout periods between active and sham stimulation periods, while observational and open-label clinical studies should aim to minimise potential confounders of treatment response and maintain longer follow-up protocols.
Ethics statementsPatient consent for publication
留言 (0)