
記住我

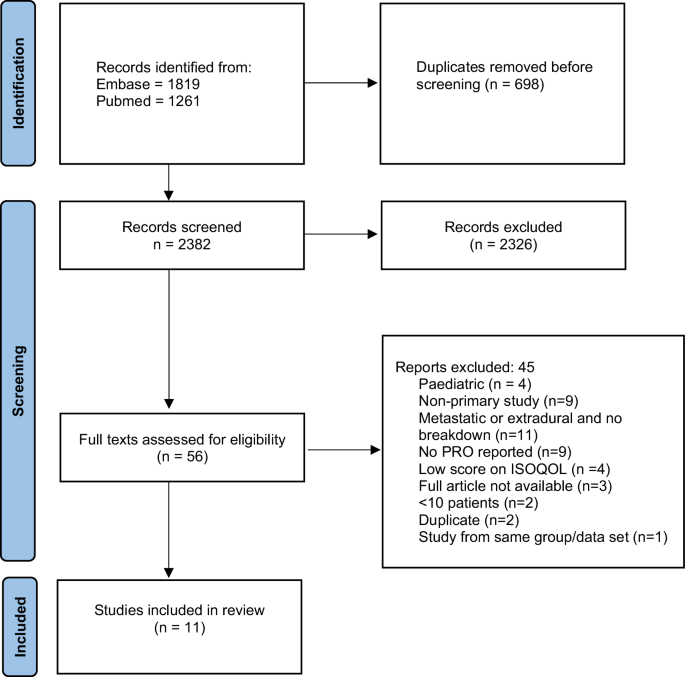


Six themes were identified from inductive thematic analysis, representing barriers and facilitators related to sexual function and satisfaction post-SCI: (1) Internalising societal views and stigmatisation; (2) Diminished sexual confidence; (3) Navigating communication; (4) Managing relationship dynamics; (5) Lack of sexual support provision; and (6) Intervention development recommendations (see Fig. 1).
Fig. 1: Qualitative Themes Identified by Thematic Analysis.
The oval demonstrates the overarching superordinate thematic context of the results. The rectangles illustrate the six qualitative inductive themes evident in the data.
Internalising societal views and stigmatisationParticipants acknowledged that they faced a major barrier as a result of result of stereotypes, societal beliefs and stigmatisation pertaining to sexuality. Sexuality whilst living with a disability was felt to be under-addressed and misunderstood both within the media and wider society.
Sexuality amongst the disabled was perceived to be ignored by the media, increasing feelings of stigmatization and separation between people considered ‘normal’ and those living with a SCI:
A lot of the stuff in the media is relating to normal people. Well, I say normal; I mean people who don’t have a disability and people who don’t live in chairs, like able-bodied people if you know what I mean. I suppose I wouldn’t really class myself in the same situation as this anymore. (Jack, complete tetraplegia)
For many, media influences created negative pressure by normalising ableist sexual imagery that was disconnected from their personal reality and experience. This impacted on levels of self-esteem and sense of attractiveness:
I think it may make you feel a bit unsexy sometimes when you look at all those skinny models and supermodels. Like when you see an advertisement for Ann Summers and all of the women advertising the outfits are tiny with lovely figures. [It] doesn’t make you feel great about yourself really, does it? (Kate, incomplete paraplegia)
Diminished sexual confidenceRebuilding one’s confidence was difficult after SCI and elicited an array of emotions, including feelings of rejection, guilt and uncertainty, which collectively negatively impacted on sexual confidence. Formative setbacks to sexual confidence were particularly memorable during the early stages of re-engagement with sexual activity:
I remember being incredibly nervous the first time I engaged in real sexual activity after my injury. I was a first-year student at university and didn’t really know what to expect at all. I knew that was able to achieve a sustainable erection, but I also knew I was unable to ejaculate. (Oliver, incomplete tetraplegia)
Moreover, reduced body confidence and lowered self-esteem due to SCI-related body changes impacted on sexual and intimate activity and perceived attractiveness:
I had body issues hugely which were even worse before my suprapubic catheter. I put on three stone in weight and got a para-belly. Whilst I feel better after losing the weight in clothes, I don’t feel better in myself out of clothes. So, it has been quite frustrating all round really (Jess, incomplete paraplegia)
Managing diminished sexual confidence often necessitated a change in perspective, moving from an emphasis on penetrative sex to encompass intimate activity more broadly:
Over the years, I’ve learnt to enjoy sex in a much wider context of the word. Foreplay, touching and being touched and just holding somebody is just as important, if not more so than the simple act of intercourse which can sometimes be overrated and comes and goes in a flash. (Oliver, incomplete tetraplegia)
Navigating communicationThe need for communication around sexual function post-injury in partner, professional and social capacities was of central importance and was thought to facilitate sexual satisfaction. Effective communication aided in the initiation of open discussion, which helped to develop, establish and sustain a sexually healthy relationship:
I think to have that openness is really important and it helps to cement that part of the relationship. It is when things start going wrong and you hide things that it all starts to go wrong. Honestly, openness is the most important thing to sustain a healthy sexual relationship. (Mike, incomplete paraplegia)
Communication acted as a barrier for those entering and establishing new relationships: “I would be nervous about having a discussion with a partner or potential partner as you don’t know how someone will react, or more importantly what the consequences will be following that discussion” (Jacob, complete tetraplegia). Participants also highlighted difficulties communicating about sex due to the fear of being judged, given that, for many, sexual function is a sensitive and confidential life domain: “I think I would be a bit reluctant to just start discussing ‘personal’ matters with someone I didn’t know” (Beth, incomplete paraplegia).
Managing relationship dynamicsIn the process of adjusting to life with SCI, partner involvement was a vital component of support and acted both as a barrier and facilitator. Worries over partner satisfaction and the impact of one’s injury on the partner were highly salient. Physical changes and obstacles in relation to sexual functioning and performance led many individuals to question whether they were able to fulfil partner needs:
I feel that my partner misses out, but she said she isn’t bothered. Is she missing out? Well, I don’t truthfully know. She says not, but she isn’t going to say she is because she knows that will hurt me too. (Robert, incomplete tetraplegia)
However, there was a prominent shift from the focus on one’s own sexual satisfaction, to instead ensuring the sexual needs and satisfaction of one’s partner were met:
I probably get more out of the satisfaction I give to her as opposed to myself. I would sooner see her with a big smile on her face rather than myself. I mean some people are selfish and want it all to themselves, but you do start to satisfy the needs of your partner more, for certain. (Mike, incomplete paraplegia)
Distinguishing care roles, reducing the caregiving impact on one’s partner and, principally, finding a balance between giving and receiving sexual satisfaction helped to maintain a sexually healthy relationship. Care provision by the partner was thought to have the potential to differentially alter relationship dynamics and opportunity for sexual connection:
So now, he has to wash me down when I have been incontinent, he has had to empty urine bags and give me enemas, all that sort of thing. So, it completely changes the way he looks at me, even though he says it doesn’t. (Jess, incomplete paraplegia)
Physical assistance provided ahead of sexual engagement by the partner was initially perceived to be ‘off-putting’, but partner reassurance limited the negative impact of this on the relationship:
The hardest thing for me is my wife having to get me on the bed first, like help me on the bed, help me get undressed and all of that. Sometimes I felt it was a bit of a put off for her, but she said it isn’t at all. (Charles, complete tetraplegia)
Consequently, attempting to separate carer from partner roles was central to retaining relational stability.
Lack of sexual support provisionAll participants highlighted the lack of sexual rehabilitative services both within the inpatient and outpatient phases of recovery. The absence of educational provision and information was found to impact on sexual preparedness and reduce feelings of sexual competence and cognitive understanding. Healthcare professionals were considered important figures in the delivery and provision of education and support, yet approachability, confidence around clinical competence, accessibility and after-care upon discharge all were barriers.
Following fruitless attempts to search for answers and information, many became disillusioned:
You try to search for anything for women after a spinal cord injury and there isn’t anything. I mean I have been told numerous times, “you have lost your function and that’s it, now you just have to accept that”. It was never discussed with me in the spinal unit. (Jess, incomplete paraplegia)
For many, upon discharge from rehabilitation, there was a complete lack of knowledge around sexual function. This left the majority doubtful, uncertain and confused, a mental state exacerbated by difficulties approaching the spinal unit for further support upon discharge:
I find it hard how you are promised things and as soon as you get out of the hospital, you are no longer their problem when you phone back up. Once you are out and discharged, you are no longer their issue. (Charles, complete tetraplegia)
There was a clear reluctance to and avoidance of initiating discussions around sex with medical professionals. Most felt that clinicians also felt awkward and uncomfortable broaching the subject. The need for further information, discussion and support was collectively emphasised:
I know it’s easy to say it, but I think sexual health, sexual function and fertility should all be better discussed and covered as part of one’s rehabilitation after a spinal-cord injury…we need to get better at realising that sexual function and sexual relationships etc is part of everyday life and people’s needs and wants should be discussed more. (Oliver, incomplete tetraplegia)
Intervention recommendationsIndividuals varied in terms of their readiness to explore sex, yet, collectively agreed that some form of increased sexual education should initially be offered during the inpatient rehabilitative phase with further readily accessible after discharge into the community. Acknowledgement of differences in needs was referenced and, given the diversity of individual requirements, a group intervention format was felt to be inappropriate:
The set-up was completely wrong, and it was males and females together. I know one-to-one might be more time consuming when you’re in hospital which is why they work the bowels and bladder workshops around groups, but for sex I just don’t think groups is the answer. (Robert, incomplete tetraplegia)
It was felt that accessible, educational support and information was a facilitator, particularly if one could access it, across both inpatient and outpatient phases of recovery. Participants felt that the development of targeted reading materials should be prioritised to maintain privacy and promote advice-seeking:
The good thing about a book, like sexual function made easy for spinal cord injury, that’s more likely to get attention that anything else. It is private too and then people could seek advice if they wanted to. (Billy, incomplete paraplegia).
留言 (0)