
記住我
A randomized, controlled, assessor-blind, parallel groups, multi-center, phase III, non-inferiority trial comparing follitropin delta in its individualized fixed-dose regimen with follitropin alfa in a conventional adjustable dose regimen was conducted at 1009 Asian patients in mainland China, South Korea, Taiwan and Vietnam (number NCT03296527). A detailed description of the elements of the trial design was described previously [14]. This was a subgroup analysis based on 759 patients (75.2%) recruited in mainland China. All women provided written, informed consent.
Study participantsChinese pre-menopausal women, aged 20–40 years, with a BMI between 17.5 and 32.0 kg/m2 and undergoing their first ovarian stimulation cycle for IVF/ intracytoplasmic sperm injection (ICSI), diagnosed with tubal infertility, unexplained infertility, endometriosis stage I/II or with partners diagnosed with male factor infertility were eligible for the study. The main exclusion criteria were women with endometriosis stage III/IV, history of recurrent miscarriage and with one or more follicles ≥ 10 mm observed before randomization. The full characterization of inclusion and exclusion criteria has been provided as supplementary table in published study (GRAPE trial) [14].
Study proceduresWomen were randomized in a 1:1 ratio to follitropin delta (Rekovelle, Ferring Pharmaceuticals) or follitropin alfa (Gonal-f; Merck Serono, Geneva, Switzerland) (Additional Fig. 1). The individualized follitropin delta (72 μg/2.16 ml) dose was determined by their serum AMH level at screening and body weight at randomization (AMH < 15 pmol/L, 12 μg/d; AMH ≥ 15 pmol/L, 0.19–0.10 μg/kg/d, minimum 6 μg/d and maximum 12 μg/d). Women randomized to follitropin alfa (900 IU/1.5 ml) started with a dose of 150 IU (11 µg) [16, 17] for the first 5 stimulation days, thereafter, the dose was adjusted by ± 75 IU based on individual response, with a maximum daily dose of 450 IU. FSH was initiated on days 2–3 of the menstrual cycle and a gonadotropin-releasing hormone (GnRH) antagonist (cetrorelix acetate, Cetrotide; Merck Serono, Geneva, Switzerland) 0.25 mg/d was initiated on day 6 and continued throughout the simulation period.
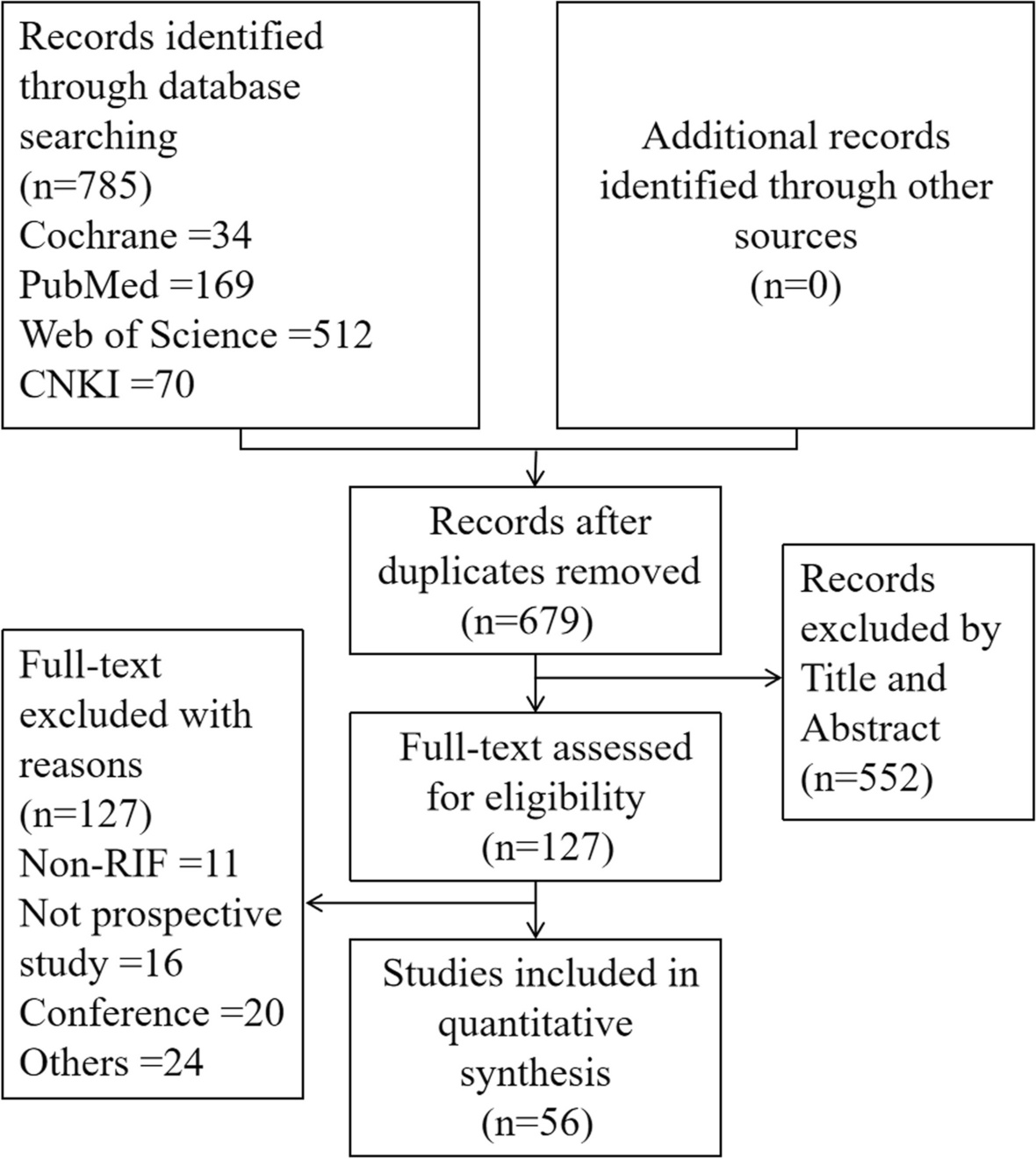
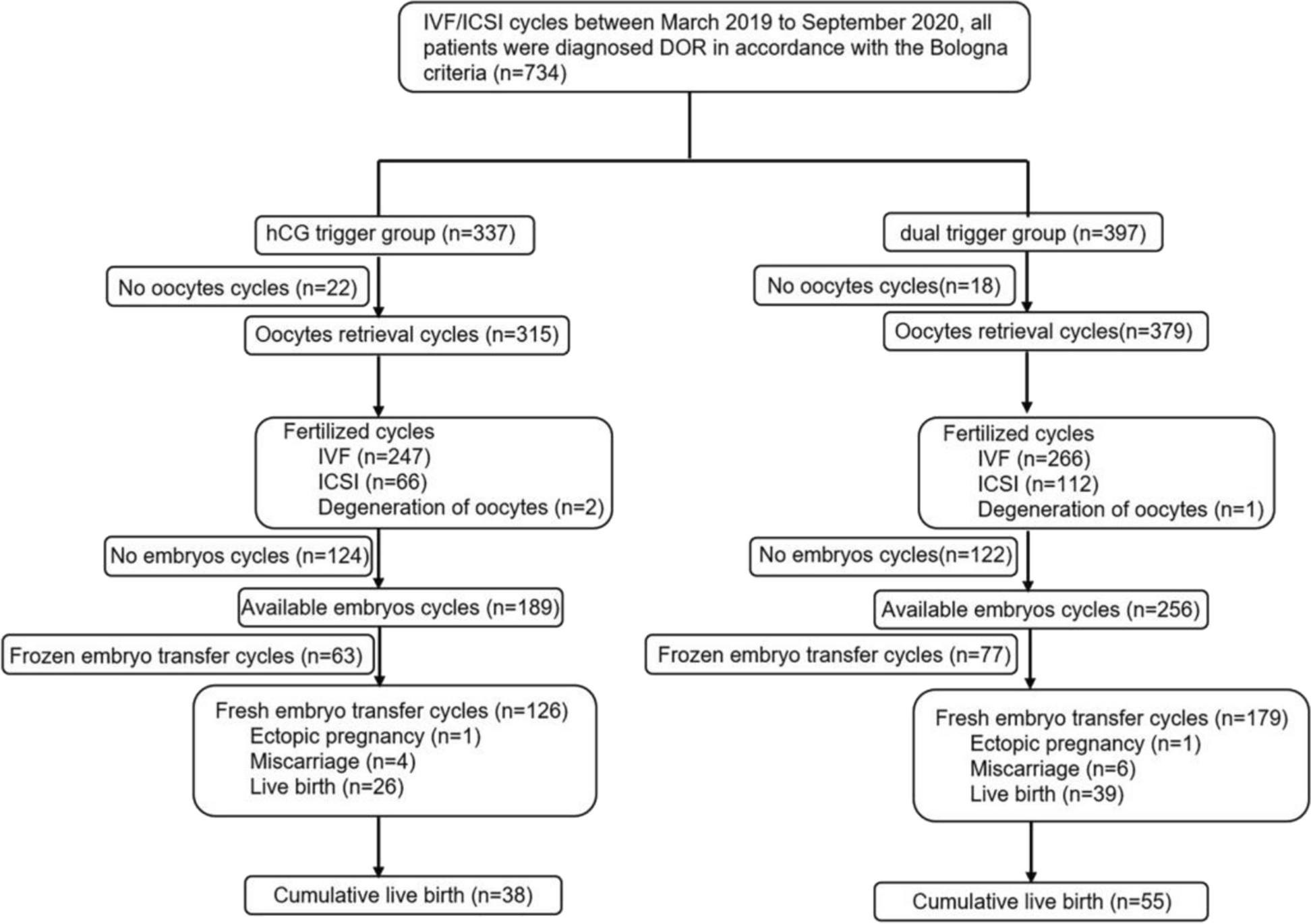
Fig. 1
Flow chart showing the number of women at each stage of the clinical trial. Note: AMH, anti-Müllerian hormone; GnRH, gonadotropin-releasing hormone; hCG: human chorionic gonadotrophin
Details of the study procedure including human chorionic gonadotrophin (hCG) triggering, oocyte retrieval, embryo transfer, vaginal progesterone gel administration, timeline of βhCG test, clinical pregnancy, ongoing pregnancy, live-birth follow-up have been published previously [14].
Study outcomesThe delivery of a healthy baby was the ultimate treatment success in this trial. The primary endpoint was ongoing pregnancy (defined as at least one intrauterine viable fetus 10–11 weeks after transfer). Secondary outcomes included other pregnancy outcomes, daily/total gonadotropin dose and duration of stimulation, oocytes and embryo development, and safety outcomes.
Other pregnancy outcomes included positive βhCG (defined as serum βhCG qualitative test performed 13–15 days after transfer), clinical pregnancy (defined as at least one gestational sac 5–6 weeks after transfer), vital pregnancy (defined as at least one intrauterine gestational sac with fetal heart 5–6 weeks after transfer), live birth (the birth of at least one live neonate) and live birth at 4 weeks (the presence of at least one live neonate 4 weeks after birth). The targeted ovarian response was defined as 8–14 oocytes retrieved.
Of the safety parameters, OHSS was an adverse event of special interest during controlled ovarian stimulation. Investigators recorded OHSS symptoms and used Golan’s classification system (1989) [18] to grade each OHSS case as mild (grade 1 and 2), moderate (grade 3) or as severe (grade 4 or 5). The criteria of OHSS were identical to those described previously by Qiao et al. [14] and in each detail by Višnová et al. [17].
Safety outcomes included adverse events such as early OHSS with onset ≤ 9 days after triggering of final follicular maturation and, preventive interventions for early OHSS defined as cycle cancellation due to excessive ovarian response or triggering of final follicular maturation with GnRH agonist with a single dose of 0.2 mg triptorelin.
In addition to the overall comparison between follitropin delta and follitropin alfa, the two treatment strategies were also compared within the two subgroups defined by AMH (< 15 pmol/l or ≥ 15 pmol/l).
Estimation of the dose equivalence factor of follitropin delta (ug) to follitropin alfa (IU) in terms of ovarian stimulation response was conducted post-hoc and compared to previously published data [16].
Statistical analysisAll analyses are based on the subgroup of women recruited in China. The mean difference in ongoing pregnancy rates (follitropin delta—follitropin alfa) was estimated using the Mantel–Haenszel method, combining risk differences across age strata, and the 95% confidence interval (CI) calculated for the full analysis set. The non-inferiority margin was -10.0%. The Mantel–Haenszel method was also used to compare the two treatment groups on positive βhCG, clinical pregnancy, vital pregnancy and live birth rates.
The FSH dose (average daily dose and total dose), duration of stimulation, number of oocytes retrieved, fertilization rate, the number and quality of embryos on day 3 were compared between the follitropin delta group and the follitropin alfa group using the van Elteren test adjusted for AMH group (< 15 pmol/l or ≥ 15 pmol/l) and using the Wilcoxon’s test to compare treatments within each AMH group. A logistic regression model with treatment and AMH group as fixed factors was used to compare proportions of women that meet the targeted response (8–14 oocytes), excessive response and early OHSS and/or preventive interventions between treatment groups. The difference between follitropin delta and follitropin alfa was reported as an odds ratio (OR) including associated 95% CI and P-value based on the likelihood ratio test. In addition, the Fisher’s exact test was provided for the treatment comparisons within AMH group.
Analyses were made post-hoc to estimate the dose equivalence factor for the follitropin delta μg dose corresponding to 150 IU of follitropin alfa for endpoints related to ovarian response. Ovarian response parameters included number of oocytes retrieved, number of follicles with a diameter of 12 mm or more at the end of stimulation, and serum concentrations of oestradiol at the end of stimulation. The individualized follitropin delta dose was calculated for all women and the relationship between the follitropin delta dose and the ovarian response was approximated with a linear function (log-dose versus response) [16] for each treatment group. The point where the two regression lines intersect was the follitropin delta dose estimated to correspond to a starting dose of 150 IU/day follitropin alfa. The intersection point was estimated from the model parameters and the 95% CI for the estimate was derived and transformed to the linear scale using the delta method. The linear approximations were illustrated in figures including estimated means and 95% CI for each dose and the dose equivalence factor.
All statistical analyses were performed in SAS (SAS Institute Inc, version 9.4, Cary, NC, USA). A level of P < 0.05 was considered as statistically significant.
留言 (0)