
記住我
KEY POINTS In obese patients, small airway and alveolar collapse tends to develop during anaesthesia and mechanical ventilation. Although the use of low/physiological tidal volume with PEEP and ARM has been largely advocated to prevent lung injury and atelectasis, the level of PEEP and the impact of ARM on respiratory, haemodynamic and oxygenation parameters remain controversial. Compared with a PEEP level of 4 cmH20, setting the PEEP at 12 cmH20 with hourly ARMs resulted in a small gain in dependent lung ventilation along with lower driving pressure and minor improvements in systemic oxygenation. At the end of each ARM, cerebral tissue oxygenation increased, whereas cardiac index and blood pressure transiently decreased.
IntroductionUp to 28% of European and 38% of American citizens are obese.1 Following major surgery, obesity is associated with prolonged hospital stay due to poor wound healing, surgical site infection, sepsis and myocardial infarction, as well as pulmonary complications.2,3 After anaesthesia induction in supine position, lung volume and oxygenation capacity are reduced, and these changes are amplified in morbidly obese patients.4 The reduced chest wall compliance results in a restrictive syndrome with heterogeneous distribution of the tidal volume (VT) that worsens during laparoscopic or robotic surgery due to abdominal gas insufflation.5 As peripheral airway closure occurs within a tidal breath, atelectasis and cyclic alveolar collapse tend to develop in the most dependent lung areas.
Application of positive end-expiratory pressure (PEEP) with periodic alveolar recruitment manoeuvres (ARMs) has been shown to be effective in preventing and reversing atelectasis formation and cyclic alveolar collapse.6–9 Thoracic electrical impedance tomography (EIT), cardiac output monitor using pulse contour analysis and near-infrared spectroscopy (NIRS) have emerged as effective and reliable tools to assess the distribution of ventilation through the lungs as well as systemic and regional oxygen delivery in anaesthetised mechanically ventilated patients.10
In a multicentre randomised clinical trial in adult obese patients undergoing elective abdominal surgery, the ‘PROBESE’ study, intra-operative ventilation with PEEP at 12 cmH2O combined with periodic ARMs was not effective in reducing postoperative pulmonary complications (PPCs) compared with a lower PEEP (4 cmH2O) without ARMs.11 It remains uncertain whether a ventilation strategy that uses higher PEEP and ARMs improves the distribution of VT without compromising cardiac output and cerebral oxygen delivery. Given the association between intra-operative cerebral oxygen desaturation and postoperative delirium, the effects of different ventilatory strategies on brain oxygenation needs to be examined.12,13 In the current substudy, therefore, we investigated the effects of the two ventilatory strategies on the distribution of ventilation in the dependent lungs, respiratory mechanics and haemodynamic parameters, as well as peripheral and cerebral oxygenation.
Materials and methods EthicsThis substudy of the PROBESE multicentre trial was conducted from January 2015 to May 2018 at the University Hospital of Geneva, Switzerland. The protocols of the parent clinical trial, and this local prospective study were approved on 12 January 2015 by the Ethics Commission for Research of the Canton of Geneva (Chairperson Prof. Bernard Hirschel, rue Gabrielle-Perret Gentil 4, CH-1211 Genève) under the number CCER 14–238. All patients were informed about the research purposes along with the practical aspects and gave written informed consent prior to inclusion.
PatientsSelection criteria for this trial included a BMI at least 35 kg per square metre, elective open or laparoscopic surgery lasting at least 120 min and an intermediate to high risk of PPCs as indicated by the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score at least 26.14 Patients with previous lung surgery, chemotherapy or radiotherapy (within last 60 days) or mechanical ventilation (within last 30 days) were excluded.
Protocol and group allocationAfter arrival in the operating room, nonpremedicated patients were connected to a multiparameter haemodynamic monitor (Philips IntelliVue X2, Amsterdam, the Netherlands) to measure mean arterial pressure (MAP), heart rate (HR) and arterial oxygen saturation (SaO2). Continuous non-invasive arterial pulse wave analysis using finger cuff technology allowed determination of stroke volume (SV; CNAP Monitor 500; CN Systems Medizintechnik AG, Graz, Austria), whereas near-infrared oximetry (Foresight device; CAS Medical Systems Inc., Branford, Connecticut, USA) allowed monitoring of cerebral tissue oxygenation (SctO2) in left and right frontal brain areas. To assess regional ventilation, a 16 electrode silicone belt of appropriate size to match chest circumference was placed at the level of the fourth or fifth intercostal space with a reference electrode on the anterior midline and connected to the EIT monitor (Pulmovista 500; Dräger Medical GmbH, Lübeck, Germany). Balanced anaesthesia was administered using desflurane or sevoflurane, low-dose opiates and muscle relaxants targeting bispectral index values between 40 and 60. Intravenous crystalloids and vasopressors were given to support blood pressure. Following orotracheal intubation, volume-controlled ventilation (Aisys CS2; GE Healthcare, Fairfield, Connecticut, USA) was provided with a VT of 7 ml kg-1 predicted body weight (PBW), respiratory rate at 12min-1 and inspiratory oxygen fraction (FIO2) set to 0.4 and adjusted to keep SaO2 at least 92%. The inspiratory to expiratory (I:E) ratio, inspiratory time and respiratory rate were adjusted to maintain end-tidal carbon dioxide partial pressure between 35 and 45 mmHg. Patients were randomly assigned to receive either a PEEP of 4 cmH2O (low PEEP group) or a PEEP of 12 cmH2O with ARMs started after endotracheal intubation and repeated hourly (high PEEP group). The randomisation process has been published elsewhere.11,15 The ARMs were achieved by stepwise increase of VT (+4 ml kg-1 of PBW) up to plateau pressure of 40 to 50 cmH2O. All patients were planned to be extubated in the operating room at the end of surgery after reversal of neuromuscular blockade.
MeasurementsRespiratory mechanical parameters were recorded from the ventilator display screen, including VT, PEEP, RR, SpO2, FIO2, end-tidal carbon dioxide fraction (FetCO2), peak inspiratory pressure and plateau pressure (PPlateau). Standard formulas were used to calculate the driving pressure (ΔP = PPlateau - PEEP), dynamic compliance (CDyn = VT/ΔP), cardiac index (CI = SV × HR/body surface area) and a pulmonary oxygenation index (SaO2/FIO2).16 Average tidal EIT-images were constructed from voltage profiles generated by cyclic injections of rotating electrical currents,17 and the impedance tidal variation (ITV) was calculated as the difference between the end-expiratory and the end-inspiratory relative impedance. Tidal EIT-images were subdivided into four horizontal regions of interest (from top to bottom: ROI I, II, III and IV) and numerical values indicated the percentage of total ventilation in each layer within 15 s time periods. Tidal EIT-images in ROI-III and ROI-IV reflected ventilation of the dependent lung region (VDL) and EIT-images in ROI-I and ROI-II reflected regional ventilation of the nondependent lung. Before anaesthesia induction, patients were prompted to breathe steadily for 3 min at a regular pace (12 to 16 cycles per minute), and over the last minute of spontaneous respiration, all EIT measurements were obtained. Intra-operatively, EIT measurements were taken when the electrocautery was not used.
All respiratory and haemodynamic parameters were recorded at four (respiratory mechanics, FetCO2) or five (oxygenation index and EIT) time points (supplemental Figure 1, https://links.lww.com/EJA/A760): before anaesthesia induction (awake), 5 min after induction and intubation (postinduction) and 1, 2 and 3 h after intubation or at the end of surgery (H1, H2 and H3, respectively). In the high-PEEP group, additional respiratory and haemodynamic measurements were done at the end of each ARM.
EndpointsThe primary endpoint was the fraction of VDL as measured by EIT; secondary endpoints included the SaO2/ FIO2 ratio, respiratory and haemodynamic parameters as well as SctO2.
Statistical analysisThe sample size calculation indicated that 72 patients per group were required to detect a relative increase of 10% in VDL in the high PEEP group, given the observed VDL values in the low PEEP group and the corresponding covariance matrix of the cohort (assuming an α = 0.05 and a power of 80%). Continuous variables were reported as means with standard deviations (SD) or 95% confidence interval (CI) or median with interquartile range [IQR], and categorical variables as frequencies (%). Continuous variables were compared using a Student's t-test or Wilcoxon rank-sum test and categorical variables using χ2 test or Fisher exact test. Standardised differences (STDs) were used to assess imbalances between baseline characteristics between the two groups. Repeated-measures mixed models were used to estimate the between and within-individual effects of high PEEP on ventilatory and haemodynamic parameters. Pairwise comparisons with Sidak-Bonferroni correction were carried out to analyse the treatment effect at each time point. The effect of ARMs on haemodynamic and ventilatory parameters in the high PEEP group was estimated using repeated-measures mixed models and paired t-tests. All analyses were performed using STATA 17 software (Stata Corp, College Station, Texas, USA).
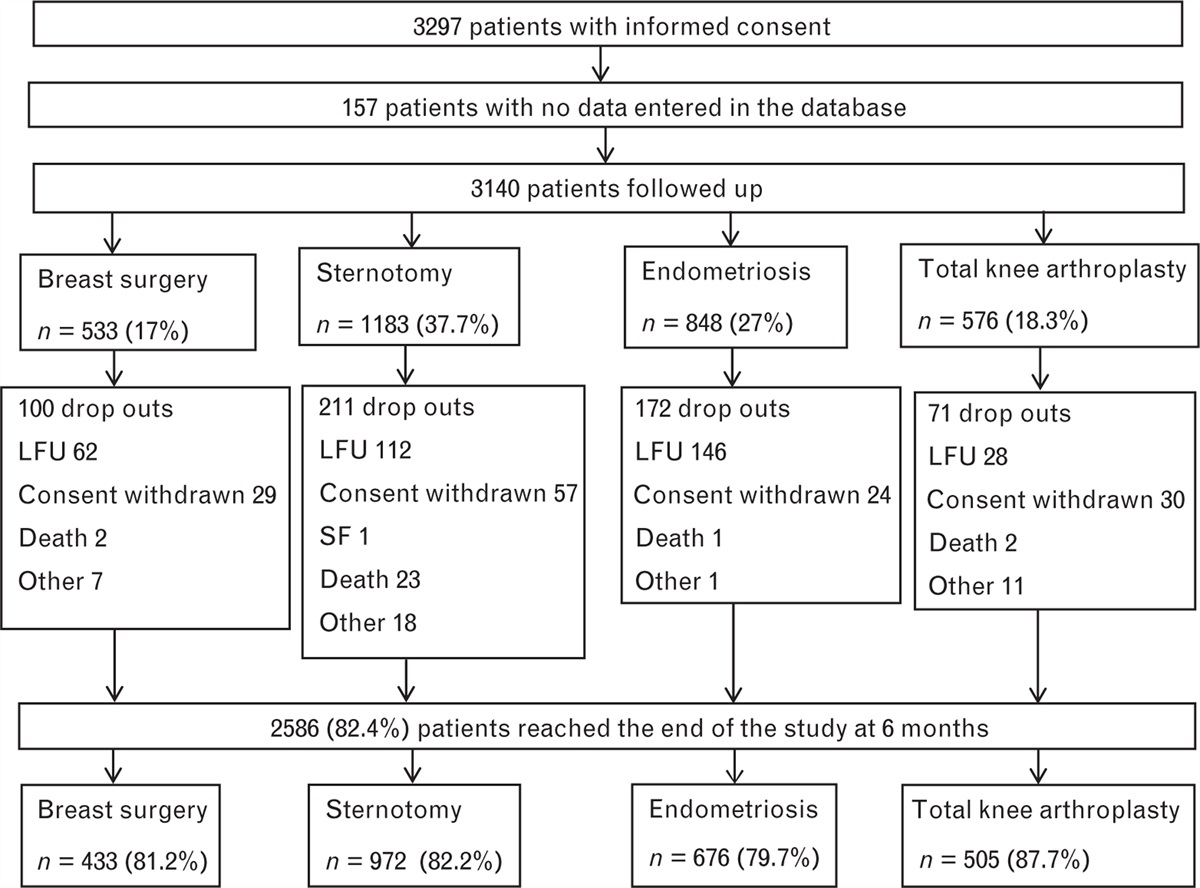
Results Study populationA total of 249 patients were enrolled and measurements of EIT, haemodynamic, respiratory and oximetric parameters were obtained in 162 patients who were included in this substudy (Fig. 1). Patient characteristics and intra-operative procedural features did not differ between the two groups (Table 1). As in the parent study, the incidence of PPCs, the need for respiratory therapy and the hospital length of stay did not differ between the two groups (supplemental Table 1, https://links.lww.com/EJA/A760). The intra-operative volume of crystalloids infused and the need for vasopressors was similar in the two groups (supplemental Table 2, https://links.lww.com/EJA/A760).
 Fig. 1:
Fig. 1: CONSORT flow diagram.
Table 1 - Pre-operative patient characteristics and intra-operative surgical data Low PEEP High PEEP Variable (n = 79) (n = 83) STD Demographics Age, years 45.4 ± 10.6 45.5 ± 11.4 −0.01134 Male, % 20 (25.3) 25 (30.1) 0.10748 BMI, kg m-2 43.5 ± 6.9 44.4 ± 8.0 −0.11999 Scores ARISCAT Score 43.6 ± 5.9 43.0 ± 6.5 0.10771 Waist-to-hip ratio 1.03 ± 0.10 1.02 ± 0.08 0.14444 ASA-PS classes III and IV 26 (32.9) 30 (36.1) 0.06804 Comorbidities, % Hypertension 68 (86.1) 72 (86.7) 0.01958 Obstructive sleep apnoea 42 (53.2) 49 (59.0) 0.11852 Chronic obstructive pulmonary disease 1 (1.3) 4 (4.8) 0.20801 Use of non-invasive ventilatory support 28 (35.4) 32 (38.6) 0.06447 Diabetes mellitus 18 (22.8) 21 (25.3) 0.05891 Gastroesophageal reflux 69 (87.3) 72 (86.7) 0.01771 Alcohol intake > 20 gday-1 9 (11.4) 10 (12.0) 0.02039 Pre-operative laboratory tests Haemoglobin, g dl-1 13.7 ± 1.4 13.5 ± 1.5 0.16404 Creatinine, mcm dl-1 68 [60 to 82] 65 [57 to 75] −0.26057 Type of anaesthesia, % Balanced general anaesthesia 77 (97.5) 82 (98.8) 0.09811 Thoracic epidural analgesia 2 (2.5) 1 (1.2) 0.09811 Patient position Head up 74 (93.7) 74 (89.2) 0.16166 Head down 1 (1.3) 4 (4.8) 0.20801 Supine position 4 (5.1) 5 (6.0) 0.04200 Surgical approach, % Open surgery 4 (5.1) 0 (0.0) 0.32660 Laparoscopic surgery 45 (57.0) 50 (60.2) 0.06661 Robotic surgery 30 (38.0) 33 (39.8) 0.03661 Intra-abdominal pressure, mmHga 14.7 ± 1.0 14.8 ± 0.7 −0.11704 Temperature at end of surgery, °C 36.9 ± 0.2 36.8 ± 0.2 0.05587 Duration of anaesthesia, min 309.5 ± 56.6 327.5 ± 78.1 −0.26442 Duration of surgery, min 229.6 ± 57.7 239.7 ± 72.3 −0.15300Data are presented as mean ± standard deviation, number (percentage) or median [interquartile range].ARISCAT, Assess Respiratory Risk in Surgical Patients in Catalonia; ASA-PS, American Society Association Physical status; SpO2, pulse oximetry; STD, standardised difference.
aIf laparoscopic or robotic surgery.
Pre-operatively, VDL under spontaneous ventilation in supine position did not differ between the two groups (49.3%; 95% CI 48.0 to 50.7 vs. 50.5%; 95% CI 49.4 to 51.7 in high-PEEP and low-PEEP groups, respectively). Following anaesthesia induction and initiation of mechanical ventilation, the reduction in VDL was smaller in the high PEEP than in the low PEEP group (-11.2%; 95% CI -8.7 to -13.7 vs. -13.9%; 95% CI -11.7 to -16.5 resulting in higher VDL (+2.7%; 95% CI 1.3 to 4.1, Fig. 2). At the end of periodic ARMs, VDL increased on average by 5.4% (95% CI 4.3 to 6.5) without reaching baseline values. After head-up positioning and gas insufflation in the abdomen, there were no changes in the distribution of VT and VDL remained stable till the end of surgery. The distribution of tidal EIT in the four ROI is illustrated in supplemental Figures 2 and 3, https://links.lww.com/EJA/A760.
 Fig. 2:
Fig. 2: Effect of intra-operative high positive end-expiratory pressure with recruitment manoeuvres vs. low PEEP on ventilation of the dependent lung part in obese patients.
Secondary endpoints and posthoc analysisCompared with baseline, SaO2/FIO2 decreased in both groups after starting mechanical ventilation (-49.6%; 95% CI -48.0 to -51.3 and -51.3%; 95% CI -49.6 to -53.1 in the high and low PEEP group, respectively) but remained slightly higher in the high PEEP group compared with the low PEEP group (+2.7%; 95% CI 1.3 to 4.1) (Fig. 3). At the end of each periodic ARM, there was a small increase in SaO2/FIO2.
 Fig. 3:
Fig. 3: Effect of intra-operative high positive end-expiratory pressure with recruitment manoeuvres vs. low PEEP on the ratio of pulsed-oxygen saturation (SaO2)/fractional inspired oxygen (FiO2) in obese patients.
As summarised in Table 2, the high PEEP group exhibited higher mean PPlateau than the low PEEP group with lower ΔP and higher CDyn. After 180 min of mechanical ventilation, CDyn decreased in the low PEEP group, whereas it remained unchanged in the high PEEP group. There was no correlation between intra-operative measurements of ΔP and VDL in the two groups (R2 = 0.0002 and 0.0074 in the low and high PEEP group, respectively) (supplemental Figure 4, https://links.lww.com/EJA/A760). Likewise, transient gains in VDL following ARMs (<10%, 10 to 25% or > 25%) were not associated with significant reductions in ΔP (supplemental Figure 5, https://links.lww.com/EJA/A760).
Table 2 - Effect of high positive end-expiratory pressure with recruitment manoeuvres vs. low positive end-expiratory pressure on respiratory parameters in obese patients Low PEEP High PEEP High PEEP Variable (n = 79) (n = 83) End recruitment P a Tidal volume ml kg-1 PBW-1 Post induction 7.2 ± 0.9 7.3 ± 0.8 14.2 ± 2.4 0.824 60 min 7.2 ± 0.9 7.3 ± 0.8 14.5 ± 2.4 0.616 120 min 7.2 ± 0.9 7.2 ± 0.8 14.3 ± 2.5 0.840 180 min 7.3 ± 0.9 7.4 ± 0.9 13.9 ± 3.0 0.462 Plateau pressure, cmH2O Post induction 24.2 ± 4.4 26.1 ± 4.0 35.0 ± 4.1 0.004 60 min 24.4 ± 4.2 26.1 ± 4.2 35.4 ± 3.8 0.012 120 min 25.1 ± 4.1 26.4 ± 4.0 35.5 ± 5.0 0.038 180 min 25.0 ± 4.3 26.7 ± 3.8 35.4 ± 4.7 0.008 Fractional inspiratory oxygen concentration, % Post induction 0.45 ± 0.06 0.44 ± 0.05 0.44 ± 0.05 0.215 60 min 0.45 ± 0.06 0.41 ± 0.02 0.41 ± 0.02 0.001 120 min 0.45 ± 0.06 0.41 ± 0.02 0.41 ± 0.02 <0.001 180 min 0.45 ± 0.06 0.41 ± 0.01 0.41 ± 0.01 <0.001 End-tidal carbon dioxide fraction, % Postinduction 5.4 ± 0.4 5.4 ± 0.4 5.0 ± 0.2 0.825 60 min 5.5 ± 0.4 5.5 ± 0.4 5.0 ± 0.3 0.945 120 min 5.6 ± 0.4 5.5 ± 0.5 4.9 ± 0.3 0.876 180 min 5.7 ± 0.3 5.6 ± 0.4 5.0 ± 0.3 0.892 Driving pressure, cmH2O Post induction 20.2 ± 4.4 14.1 ± 4.0 23.0 ± 4.1 < 0.001 60 min 20.4 ± 4.2 14.1 ± 4.2 23.4 ± 3.8 < 0.001 120 min 21.1 ± 4.1 14.5 ± 4.2 23.5 ± 5.0 < 0.001 180 min 21.0 ± 4.3 14.7 ± 3.8 23.4 ± 4.7 < 0.001 Compliance, ml cmH2O-1 Post induction 26.4 ± 7.0 31.6 ± 9.1 38.9 ± 10.6 < 0.001 60 min 25.6 ± 5.5 32.5 ± 11.2 39.0 ± 10.2 < 0.001 120 min 24.2 ± 4.5 30.8 ± 8.4 39.2 ± 10.0 < 0.001 180 min 22.8 ± 4.2 30.2 ± 7.5 39.8 ± 9.9 < 0.001Data are presented as mean ± standard deviation.PBW, predicted body weight.
aHigh PEEP vs. low PEEP.
Intra-operatively, haemodynamic parameters did not differ between the two groups (Fig. 4). ARMs transiently decreased MAP (-13.7 mmHg; 95% CI -12.5 to -14.9) and CI (-0.54 l min-1 m-2; 95% CI -0.49 to -0.59). Intra-operatively, SctO2 in the right and left sides remained unchanged in the high PEEP group and small decreases in SctO2 occurred over time in the low PEEP group (Fig. 4). Following ARMs, SctO2 increased slightly (3.0 and 3.2% on left and right front brain, respectively).
 Fig. 4:
Fig. 4: Intra-operative effects of high positive end-expiratory pressure (PEEP) with recruitment manoeuvres vs. low PEEP on mean arterial blood pressure, cardiac output as well as left and right-sided cerebral near-infrared spectroscopy (NIRS).
DiscussionIn this cohort of obese patients undergoing abdominal surgery and at risk of PPCs, a ventilatory strategy using low/physiological VT and a PEEP of 12 cmH2O with periodic ARMs compared with a PEEP of 4 cmH2O without ARMs resulted in minor redistribution of ventilation in the dependent part of the lungs, with transient further gain during ARMs; higher PPlateau with reduction in ΔP but no correlation between the fall in ΔP and improved VDL; and similar haemodynamics and minor improvements in SctO2, with transient decreases in CI and MAP during ARMs.
In this large sample of obese patients, EIT allowed real-time non-invasive imaging of regional lung aeration and it was used to compare the effects of higher to lower PEEP levels on the distribution of VT through the lungs. Analysis of tidal impedance variations has been validated in mechanically ventilated patients against spirometry for VT measurements and computed tomography to detect atelectasis formation, alveolar recruitment and overdistension.18,19 Placing the EIT belt at the fourth to fifth intercostal space generates a 5 to 10 cm wide cross-section in the thorax and represents a valuable compromise to describe the distribution of VT through the middle part of the lungs while avoiding interferences due to surgical manipulation.20 Respiratory mechanics, systemic and cerebral oxygenation variables were collected at different times during surgery as well as before and after ARMs. This made possible to explore the association between the changes in regional lung aeration, respiratory mechanical function, and haemodynamic parameters at two levels of PEEP with or without periodic ARMs.
Following anaesthesia induction, mechanical ventilation with physiological VT resulted in a moderate shift of ventilation from dependent to nondependent lung areas with reduction in pulmonary oxygen uptake reflecting greater ventilation-perfusion mismatch, as previously reported in cardiac and visceral surgery.5,21,22 In our patients, pre-operative oxygenation with FIO2 of 1.0 promoted absorption atelectasis in the dependent well perfused lung parts, whereas the reverse Trendelenburg position favoured caudal displacement of the diaphragm, along with some preservation of lung volumes in the dorso-caudal pulmonary regions.23 Compared with low PEEP at 4 cmH2O, moderate PEEP at 12 cmH2O coupled with periodic ARMs resulted in slightly higher PPlateau (+1.7 cmH2O) with a marginal gain in dorsal ventilation (+2.7%) and lesser stress on lung structures as reflected by lower driving pressure (-6.3 cmH2O) and higher CDyn (+ 6.6 ml cmH2O-1). In both obese and nonobese anesthetised patients, combining a PEEP at 8 to 10 cmH2O with periodic ARMs has been shown to be effective in increasing respiratory compliance, oxygenation and lung aeration in contrast with PEEP at 0 to 2 cmH2O and no ARMs.21,22,24–26 In our cohort, we found no correlation between the changes in ΔP and VDL in both groups. Moreover, the small improvements in dorsal lung aeration and systemic oxygenation were only transient and failed to reach pre-operative levels following each ARM. In similar obese surgical patients, it has been demonstrated that repeating ARM every 10 min in addition to setting a PEEP level at 10 cmH2O was necessary to provide consistent improvement in respiratory compliance and oxygenation.27 Altogether, lung imaging and physiological data suggest that setting a PEEP at 10 to 12 cmH2O with hourly ARM does not consistently reverse respiratory disturbances induced by anaesthesia and mechanical ventilation and that ΔP derived from ventilator circuit measurements (PPlateau - PEEP) is a poor indicator of optimal lung recruitment in obese individuals with uninjured lungs. Considering the interference of respiratory mechanical properties with patients’ characteristics (e.g. BMI, fat distribution, thoraco-abdominal anatomy), positioning and surgical approach (e.g. pneumoperitoneum, laparotomy), optimising the PEEP levels in each individual has been advocated by targeting the best compliance (PEEP titration trial) or an end-expiratory transpulmonary pressure of 0 cmH2O (oesophageal pressure) or by minimising lung collapse and overdistension (EIT lung imaging).6,8,28,29 Application of such open-lung ventilation strategy requires higher PEEP levels (∼15 to 23 cmH2O) than in our study and has been shown effective at lowering mechanical stress, increasing oxygenation and end-expiratory lung volume with more homogeneous VT distribution as evidenced by lesser collapsed and distended lung areas in obese patients during abdominal surgery.6,8,29,30 However, the intra-operative respiratory benefits of higher PEEP levels with periodic ARMs disappear shortly after anaesthesia emergence and do not translate into better clinical respiratory outcomes.8,22,31 Although current evidence suggests that the use of low/physiological tidal volume or physiological VT improves clinical outcomes,32 the role of ΔP for titrating ventilation and the optimal settings of PEEP with periodic ARMs in obese patients remain unclear and deserve further investigation.
In this study, haemodynamic parameters and cerebral oxygenation were similarly preserved at higher and lower PEEP. During ARMs, hyperventilation and limitation in venous return due to larger tidal volumes with higher intrathoracic pressure produced transient reduction in FetCO2, CI and MAP. The acute hypocapnic cerebral vasoconstriction resulting from the observed mean 0.5% reduction in FetCO2 (∼ -4 mmHg arterial CO2 pressure) was expected to lower cerebral blood flow by 8 to 12% and would be reflected by a 3 to 4% fall in SctO2 in normoxic conditions.33,34 In contrast, we observed an average 3% increase in SctO2 following ARMs, suggesting that the improved blood oxygenation (SaO2/FIO2) consequent to increased dorsal lung aeration overcompensated the hypocapnic vasoconstriction within the cerebral autoregulatory range (e.g. MAP maintained above 70 mmHg). These favourable findings differ from those reported in patients undergoing carotid endarterectomy and in mechanically ventilated patients with brain injury or acute respiratory distress syndrome, in whom ARMs are often associated with impaired systemic haemodynamic and worsened cerebral oxygenation with no improved systemic oxygenation.35–37 In summary, these results suggest that ARMs may transiently increase cerebral oxygenation in normovolaemic patients with preserved cerebrovascular autoregulation and no elevated intracranial pressure.38 Optimising oxygen delivery to the brain is clinically relevant, as avoidance of cerebral oxygen desaturation has been associated with less postoperative cognitive dysfunction.39
This study has limitations. Firstly, as designed in the original PROBESE study, we compared the effects of two levels of PEEP that were lower than those reported in individualised PEEP trials wherein larger improvements in dependent lung aeration with higher respiratory compliance were reported in anaesthetised obese patients.6–8,27,28 Secondly, different protocols of ARMs using continuous positive pressure over 30 to 60 s or stepwise increase in VT or PEEP levels could yield different haemodynamic and respiratory effects.40 Thirdly, our results obtained this single-centre substudy with obese patients undergoing laparoscopic surgery lasting on average 4 h in reverse Trendelenburg position could not be extrapolated in other type of surgery and in patients with diseased/injured lungs. Although higher (compared with lower) levels of PEEP are associated with physiological improvements and clinical benefits in critically ill patients with or without acute respiratory distress syndrome, the impact of obesity in adjusting well tolerated levels of PEEP has not been explored so far.41,42 Given the worldwide obesity epidemic, further well designed and powered studies are needed to examine the optimal ventilatory strategy in the increasing numbers of obese patients who may require emergency surgery following trauma or sepsis.
In conclusion, in obese anaesthetised patients undergoing abdominal surgery in reverse Trendelenburg position, intra-operative application of a PEEP at 12 cmH2O with periodic ARMs compared with a PEEP at 4 cmH2O without ARMs, slightly redistributed ventilation to dependent lung areas along with minor improvements in respiratory mechanics as well as peripheral and cerebral oxygenation.
Acknowledgements relating to this articleAssistance with the study: we wish to thank all the anaesthesiology and the surgical teams of University Hospital of Geneva for their support in this study. The authors thank the Steering Committee for the Protective Intraoperative Ventilation with Higher versus Lower Levels of Positive End-Expiratory Pressure in Obese Patients (PROBESE) Collaborative Group (listed below) for critical revision of important intellectual content.
Steering Committee for the PROBESE Collaborative Group: Thomas Bluth, Ilona Bobek, Jaume C. Canet, Luc de Baerdemaeker, Cesare Gregoretti, G.ran Hedenstierna, Sabrine N. T. Hemmes, Michael Hiesmayr, Markus Hollmann, Samir Jaber, John Laffey, Marc J. Licker, Klaus Markstaller, Idit Matot, Gary Mills, Jan Paul Mulier, Christian Putensen, Rolf Rossaint, Jochen Schmitt, Mert Senturk, Paolo Severgnini, Juraj Sprung, Marcos Francisco Vidal Melo, Hermann Wrigge, Ary Serpa Neto, Marcus J. Schultz, Paolo Pelosi, and Marcelo Gama de Abreu (chair).
Financial support and sponsorship: this work was supported by the Department of Anaesthesia, Pharmacology, Intensive Care and Emergency Medicine, University Hospital of Geneva.
Full protocol accessible by request to the corresponding author.
Conflicts of interest: Dr Wrigge received research funding, lecture fees, and technical support from Dräger Medical (Lübeck, Germany); funding from Pfizer (Investigator Initiated Trial Program; Berlin, Germany); funding and lecture fees from InfectoPharm (Heppenheim, Germany); lecture fees from GE Healthcare (Freiburg, Germany), Maquet (Rastatt, Germany), and MSD (Konstanz, Germany); advisory board honoraria from Liberate Medical (Crestwood, Kentucky); Dr Gama de Abreu received fees for consulting activities or contract research from Ambu (Bad Nauheim, Germany), ZOLL Me
留言 (0)