
記住我








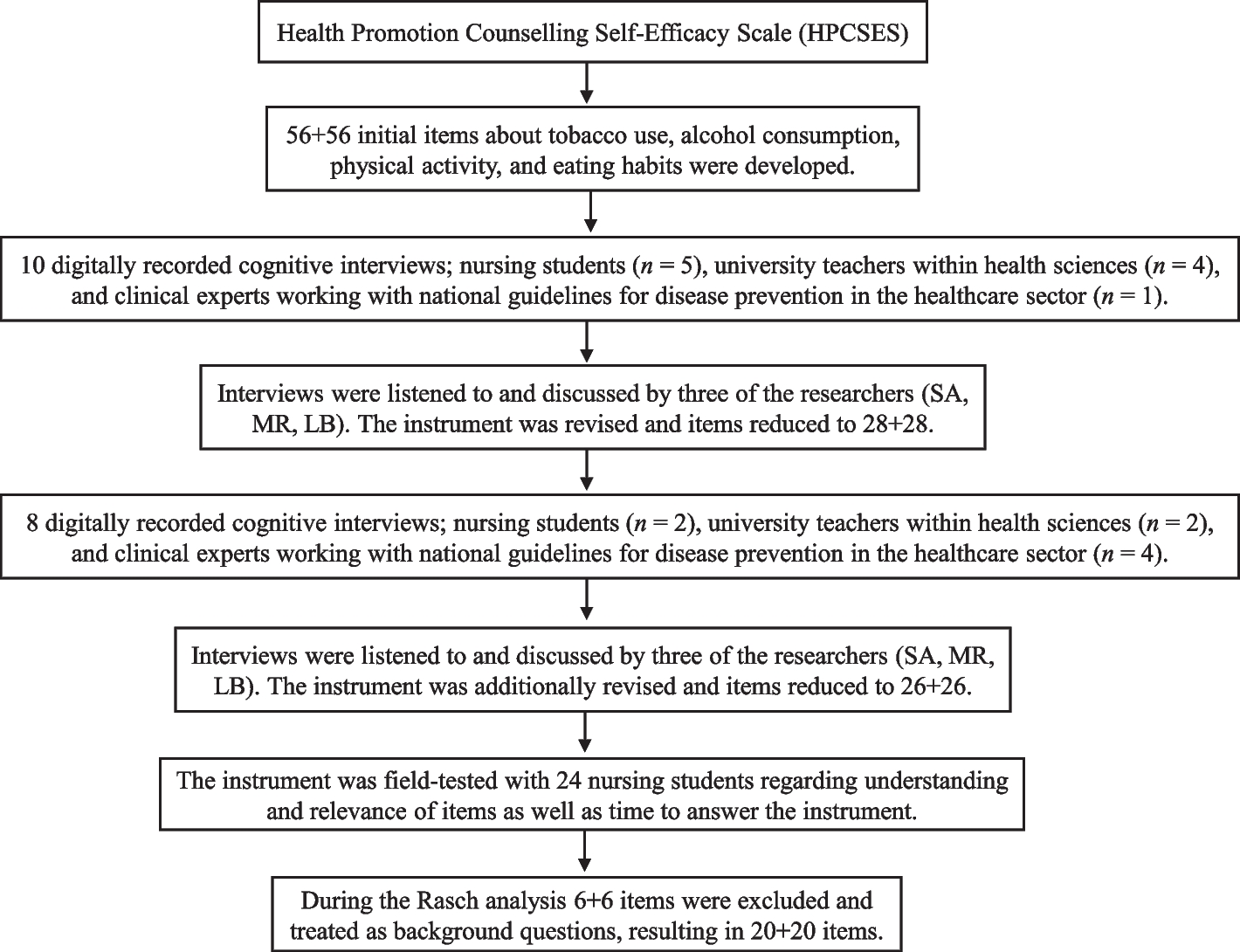
For the present cross-sectional questionnaire study conducted between January 2019 and March 2020, adult pwCF attending a CF specialist center were recruited. Each subject completed a questionnaire on CS/therapy adherence and HRQoL during a routine visit to the outpatient clinic or during an inpatient stay. Additionally, demographical and clinical data were assessed by the treating physician during the visit/stay (Fig. 1).
Fig. 1 Participants
ParticipantsAll adult pwCF attending the CF center at Ruhrlandklinik, Universitätsmedizin Essen, Germany, were considered eligible for the study. The inclusion criteria were a confirmed diagnosis of CF according to the Cystic Fibrosis Foundation guidelines [12], an age of 18 years or older, and the ability to complete the questionnaires without help. Patients with CF after lung transplantation were excluded.
MeasuresDisease statusObjective measurements of disease status included ppFEV1, BMI, genotype, Pseudomonas aeruginosa colonization status, pancreatic function status, and the presence of CF-related diabetes mellitus.
Health-related Quality of LifeHRQoL was measured using the revised 'Cystic Fibrosis Questionnaire for adolescents and adults over 14 years old (CFQ-R + 14)', which has previously been validated and shows good psychometric properties for the German version for adolescents and adults with CF [13]. The CFQ-R + 14 measures daily functioning from the patient's perspective over the previous two weeks and consists of 50 items across the following 12 domains: physical functioning, role, vitality, emotional functioning, social, body image, eating disturbances, treatment burden, health perceptions, weight, respiratory symptoms, and digestive symptoms. Each domain is standardized on a 0–100 scale; higher scores indicate better HRQoL.
CS, therapy adherence, diagnosis disclosureData on CS, therapy adherence, and diagnosis disclosure were collected with a self-report questionnaire developed by the research team (Additional file 1: Table S1). The survey includes 12 items that measure participants' assessment of future health perspectives (one item), cough frequency and sputum quantity (two items), CS (one item), therapy adherence (three items), and diagnosis disclosure (four items, Additional file 1: Table S1). In addition, the participants were asked to specify their educational, employment, and marital status.
Statistical analysesData handling and statistical analyses were performed with SPSS 27.0 (IBM Corp., Armonk, NY). H1-4 were assessed by two-tailed testing, and the results were considered significant at p < 0.05. All other analyses were deemed exploratory, or the results were corrected for multiple comparisons controlling the two-tailed false-discovery-rate (FDR) at q < 0.05 [14] as indicated below. Effect size calculations relied on SPSS (semipartial correlation (sr)—small ≥ 0.1, medium ≥ 0.24, large ≥ 0.37) or an online calculator (d—small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8) [15].
Correlation and multiple regression analysisCategories of CS were collapsed into 3 categories (category 1: ‘never’ and ‘seldom’; category 2: ‘occasionally’; category 3: ‘frequently’ and ‘always’), and the 4 categories of sputum quantity were reclassified into 2 categories (category 1: ‘no’ and ‘little’; category 2: ‘moderate’ and ‘substantial’). The variable therapy adherence was coded by summing scores on the items self-administered physical therapy (none = 0, ≤ 1x/week = 1, 2-3x/week = 2; every day = 3), supervised physical therapy (none = 0, < 1x/week = 1, 1x/week = 2, > 1x/week = 3), and exercise (none = 0, < 1x/week = 1, 1x/week = 2, > 1x/week = 3) as a measure of adherence. Prior to analysis, all categorical variables were dummy coded.
Considering the sample size of the present study and a large number of potential covariates (age, genotype, cough frequency, sputum quantity, diabetes, exocrine pancreatic insufficiency, Pseudomonas colonization status, therapy adherence, employment status, marital status), an analysis-specific subset of covariates with a significant correlation with CS and the outcome measure of interest (ppFEV1, BMI, CFQ-R overall and subscale scores, or perspectives) was selected [16].
The linear relationship between ppFEV1, BMI, and CFQ-R (overall and subscale) scores (dependent variables) and CS (independent variable) was assessed by multiple linear regression considering covariates identified by the previous step of analysis. The interaction between CS and sex was modelled by multiplying both dummy-coded variables (2 dummy variables for CS, 1 dummy variable for sex). The results regarding the subscales of the CFQ-R were FDR-corrected for multiple comparisons. Considering the scale of measurement of the outcome perspectives, its relationship with CS was determined by ordinal logistic regression relying on a probit function, likewise accounting for important covariates.
Testing of the assumptions regarding the respective statistical procedure is detailed in the Additional file 1.
留言 (0)