
記住我
The potential contribution of the epidermis and in particular of keratinocytes to the pathogenesis of dermal fibrosis has been neglected for long time. Recent work, however, has shown that the homeostatic relationships normally regulating the crosstalk between epidermal and dermal cell constituents is altered in scleroderma, thus reinforcing the concept that keratinocytes may take part to scleroderma pathogenesis. Previous work, exploring physiological conditions, demonstrated that keratinocytes stimulate fibroblasts, mainly through the production of interleukin (IL)-1, inducing in fibroblasts the production of keratinocyte growth factor (KGF) also known as fibroblast growth factor 7. In turn, fibroblasts affect keratinocyte viability, proliferation, and differentiation mainly by producing KGF. This inter-relationship is modulated by a variety of other factors which participate to homeostatic crosstalk between keratinocytes and fibroblasts reviewed in [1]. Importantly, healthy keratinocytes were known to affect extracellular matrix (ECM) deposition and resorption by influencing fibroblasts, favoring resorption over deposition. Under this perspective, previous work addressing SSc-specific epidermal alterations showed that compared to healthy donor (HD), SSc keratinocytes conditioned media increase type-I collagen (Col-I) production by enhanced oncostatin M (OSM) production [2], an effect independent from transforming growth factor (TGF)-β [3], favoring enhanced IL-1-dependent gel contraction in which both TGF-β and endothelin-1 (ET-1) were needed [4]. By enhanced connective tissue growth factor (CTGF) and S100A9 production, SSc keratinocyte could also favor fibroblast production of Col-1 as well as fibroblast migration and proliferation [5]. Interestingly, SSc fibroblasts were reported to respond to keratinocyte conditioned medium with higher production of Col-I and a similar production of matrix metalloproteinase-1 (MMP-1), resulting in an increased ratio of col-I over MMP-1, suggestive of decreased ECM turnover [6].
 Box 1:
Box 1: no caption available
PROGRESS IN RECONSTITUTED SKIN MODELSWhen addressing the role of the epidermis and dermis in SSc pathogenesis, it has to be taken into consideration that these anatomical structures are not faithfully reproduced in in vitro systems in which both keratinocytes and fibroblasts are cultured in 2D systems and when the respective conditioned media are used to stimulate the cell counterpart. Although a method for isolating and culturing skin cells, including endothelial cells, fibroblasts, keratinocytes, and melanocytes from small SSc skin biopsies has been published [7], increased efforts in the field of tissue engineering have recently led to the development of 3D human models with improved intercellular interactions and tissue microenvironment observed in skin fibrosis [8]. Self-assembled or scaffold-based models exploit the ability of fibroblasts to generate 3D dermal-like constructs, producing their own ECM. The addition of TGF-β or other pro-fibrotic regulators is a simple mean of inducing fibrotic shift [9]. Incorporation of SSc fibroblasts results in a model with altered collagen structure, characterized by a more mature and aligned fibrillar structure, leading to increased stromal rigidity and upregulation of innate immune signaling genes [10]. The layering of keratinocytes on overlapping sheets of self-assembled fibroblasts, followed by exposure to air–liquid interphase, leads to the formation of a fully stratified epidermis (i.e. containing basal, spinous, granular and corneal layers), making these models appropriate for mimicking the interaction between the dermal and epidermal compartments [11]. Of interest, immune cells may be included within self-assembled skin (saS) models. Thus, peripheral blood monocytes incorporated in skin equivalents – generated from SSc fibroblasts and SSc keratinocytes – differentiated into M2-like cells and resulted in increased thickness and stromal rigidity. Of interest, greater numbers of M2-like macrophages populated SSc-saS compared with HD-saS, thus suggesting a reciprocal activation between macrophages and fibroblasts resulting in increased tissue thickness and stiffness [12▪▪]. Decellularization of living tissue is also a promising approach and a porcine, decellularized, intestine scaffold has been exploited to reconstruct human skin equivalent by the sequential seeding of endothelial cells, fibroblasts and keratinocytes resulting in a fully polarized epidermis, dermis and a functional vasculature. This model recapitulated key features of SSc skin upon TGF-β stimulation, including the transdifferentiation of fibroblasts into myofibroblasts and excess ECM deposition and was sensitive to nintedanib treatment [13]. Additional models have been established in the recent past. One consisted on human skin equivalents fully generated from healthy or SSc donor skin cells in vitro then grafted onto SCID mice. This model allowed the replication of the fibrotic phenotype when grafted tissues were of SSc origin. Interestingly, in this in vivo model the generated skin from healthy donors acquired bona fide SSc characteristics when humanized monoclonal antibodies specific for the platelet derived growth factor (PDGF) receptor were injected into the graft [14]. An additional model was based on the organotypic culture of healthy, full, human skin obtained by esthetic surgery which showed enhanced collagen and reduced MMP-1 production under the influence of TGF-β. In this model, the exposure to IL-17 resulted in enhanced production of MMPs counteracting the profibrotic activity of TGF-β [6]. Future expected developments in tissue engineering potentially useful to address pathophysiological aspects of skin fibrosis including the influence of keratinocytes on the development or resolution of dermal fibrosis could be based on the use of induced pluripotent stem cells (iPSCs) [15] or organ-in-chip technologies [16]. Thus, future efforts will help in investigating the subtle modification governing and altering the crosstalk between epidermis and dermis in fibrotic conditions.
KERATINOCYTES IN DERMAL FIBROSISA powerful method to test whether ex vivo SSc may differ from HD keratinocytes would be the study of differentially expressed genes detected by gene arrays or RNA sequencing in bioptic tissues or single cell preparations. However, such studies have principally focused on fibroblast, endothelial cells, and inflammatory infiltrating cells rather than on keratinocytes. This notwithstanding by comparing genes differentially expressed in full skin biopsies from 61 SSc from the Genetics vs. Environment in Scleroderma Outcome Study cohort to 36 HD, it was found among others that enriched pathways included ‘keratinocyte differentiation’ in the subgroup of SSc individuals positive for anticentromere antibodies [17]. In another study, by comparing the signature scores in early vs. late diffuse disease, the keratinocyte signature was higher in late disease [18]. When performing consensus clustering and meta-analysis on three genome-wide datasets, a community containing modules enriched for keratinocyte-specific processes was found to make contact with the inflammatory module [19]. Thus, while sparse, unbiased analytical approaches based on gene expression are hinting to keratinocyte alterations in SSc. Future keratinocyte-centered studies should provide stronger evidence of their potentially dysregulated genes in SSc epidermis.
Systemic sclerosis epidermal equivalentsEngineered epidermal equivalents (EE) were used by us to investigate whether keratinocyte activation and differentiation as well as gene expression could distinguish EE generated by using primary SSc keratinocytes from their HD counterpart [20▪▪]. Interestingly, SSc-EE exhibited aberrant differentiation, enhanced expression of activation markers, and a lower rate of basal keratinocyte mitosis, reproducing most of the abnormalities histologically detected in SSc epidermis. RNA sequencing analysis revealed that, compared to HD-EE, SSc-EE were characterized by lower expression of homeobox gene family members. Using the Hallmark gene set from the Molecular Signatures Database both metabolic and oxidative stress molecular pathways resulted to be enhanced in SSc-EE. This is in agreement with previous abundant experimental data supporting a role of oxidative stress in the pathogenesis of SSc [21]. We went further and could demonstrate that conditioned medium generated from EE enhanced the production of IL-6, IL-8, MMP-1, Col-I, and fibronectin by fibroblasts. Notably, this effect was two-fold higher in the presence of conditioned medium generated form SSc EEs (with the exception for Col-I and fibronectin). These data support the notion that SSc keratinocytes have an intrinsically altered differentiation program, which is maintained when keratinocytes adapt to in vitro conditions, while proliferating and generating a stratified epidermis in the absence of cues derived from other cell types or from structured dermis [20▪▪]. Further work should test whether epigenetic mechanisms may be involved.
Less is moreThe interesting, understudied possibility that the relative lack rather than the excess of a particular soluble mediator of inflammation could be involved in the pathogenesis of scleroderma received recent attention. Starting from the hypothesis that IL-25 (member of the IL-17 family, known also as IL-17E), acknowledged for being produced by epithelial cells, could be involved in fibrotic processes, we assessed its presence in SSc skin and found that its expression was reduced in SSc compared to HD epidermis. In EE generated using primary HD keratinocytes IL-25 regulated several molecular pathways related to wound healing and ECM remodeling and the conditioned medium from IL-25-primed keratinocytes enhanced the fibroblast production of MMP-1, IL-6, IL-8, but not of Col-I nor fibronectin. However, IL-25 significantly reduced the production of Col-I when applied directly to fibroblasts. This evidence was supportive for the role of IL-25 in participating to skin homeostasis and its decreased expression in SSc could contribute to skin fibrosis by favoring ECM deposition over degradation [22▪]. Similarly, from the functional point of view, the EBI3 (constituting IL-35 in conjunction with p35) expression was found by others to be decreased in keratinocytes of the SSc epidermis compared to HD. Of interest, the injection of EBI3 in the skin of mice enhanced fibrosis. Indeed, EBI3 was able to downregulate the protein and mRNA expression of type I or type III collagen, in the presence or absence of TGF-β, by reducing collagen mRNA stability [23]. Thus, the keratinocyte-specific decrease of two distinct cytokines characterizes SSc epidermis. This decreased expression appears to have functional consequences in homeostatic processes regulating dermal ECM turnover favoring fibrosis. Future studies should address the therapeutic potential of targeted therapies aiming at increasing the keratinocyte production of such cytokines.
Keratinocytes in additional models of skin fibrosisThere are some similarities between SSc and the sclerodermatous chronic form of the graft versus host disease (cGVHD) in terms of skin fibrosis. A major difference may be due to the mechanism of damage of the epidermis which may be mediated by allogenic CD8+ T cells in cGVHD. In this respect, a recent publication reports an increased production of TGF-β by epidermal cells, especially of the basal cell layer, in samples from patients with cGVHD compared to acute GVHD and HD. By establishing a model of cGVHD-like sclerodermatous changes in genetically modified mice transferred with cytotoxic CD8 T cells specifically targeting keratinocytes, these authors observed reduced fibrosis when CD8 T cells were interferon-gamma (IFN-γ) deficient. The reduced fibrotic reaction correlated to a lower expression of TGF-β by keratinocytes undergoing apoptosis. These results indicate that keratinocytes produce higher amounts of TGF-β1 in the presence of IFN-γ when undergoing apoptosis, thus participating to sclerodermatous changes [24].
Taking advantage from the integration of single-cell and bulk transcriptome data among the dysfunctional cell types expressed in hypertrophic scars, a fibroproliferative skin disorder characterized by excessive ECM deposition, the proportion of a particular subtype of keratinocytes named by the authors KC-2 was reduced when compared to healthy skin. Cell-cell communication analysis revealed intercellular contacts between some fibroblast types and KC-2. Interestingly, syndecan 4 (SDC4), a receptor expressed also in KC-2 which could bind multiple ligands, was downregulated in hypertrophic scars, suggesting that the reduced proportion of KC-2 and apoptotic phenotype of KC-2 might be associated with the downregulation of SDC4 [25]. In summary, evidence gathered in experimental models of fibrotic skin diseases highlight the role of keratinocytes and their involvement in processes associated to dermal fibrosis.
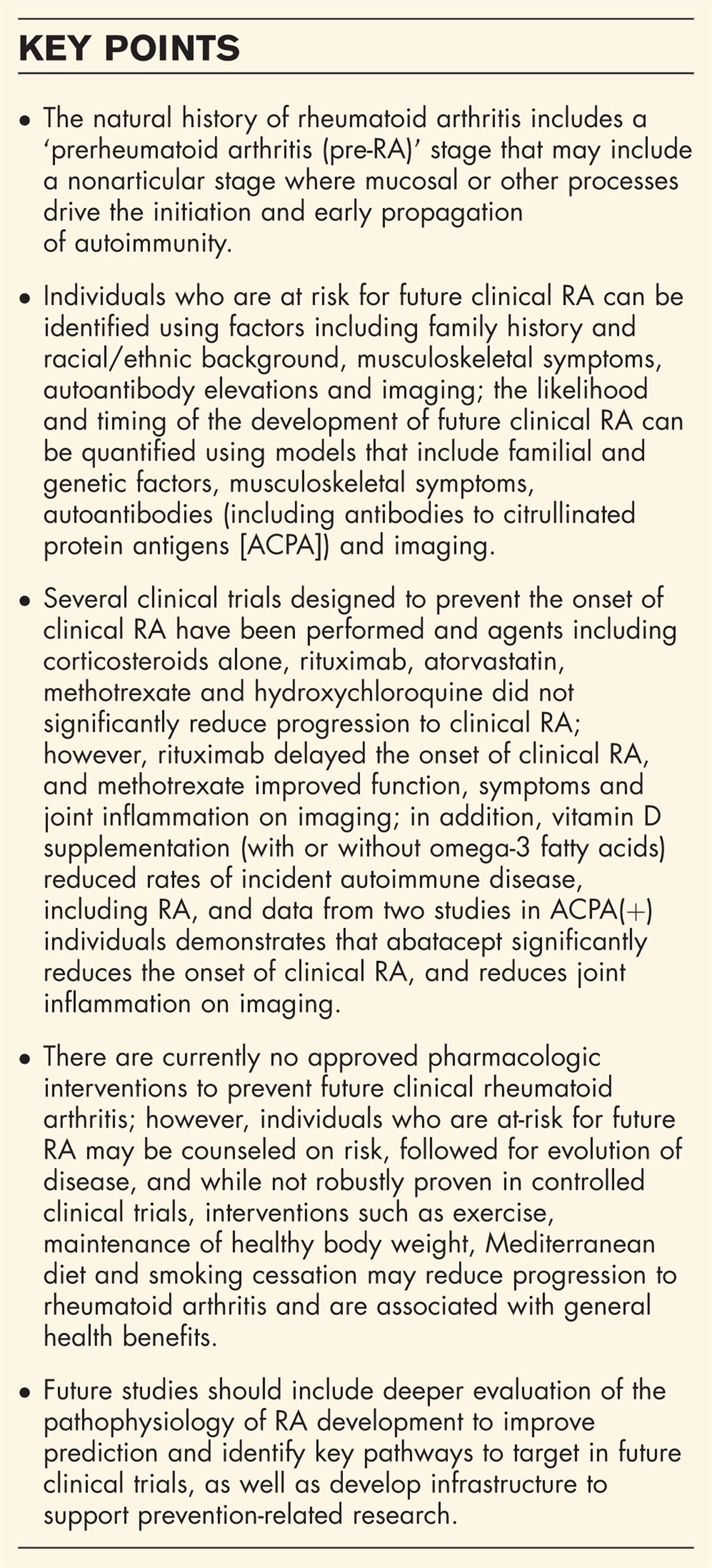
ARE ABNORMALITIES IN SYSTEMIC SCLEROSIS KERATINOCYTES PRIMARY OR SECONDARY?The question arises whether the morphological and functional alterations described in SSc keratinocytes and skin are secondary to pathological events arising elsewhere, in particular in the dermis or whether they are not the consequence but rather the cause of other pathologic features, including increased ECM deposition (Fig. 1). Or as a further possibility whether these abnormalities arise in parallel under the influence of factors driving keratinocyte, fibroblast, and other cell types altered activities. No firm answer is available to this question at the time being. Nonetheless, we would like to stress evidence generated in animal models which may support the contention of a primary role of keratinocytes in the cascade of pathogenic events leading to SSc.
 FIGURE 1:
FIGURE 1: Potential interactions relevant to keratinocyte and fibroblast dysregulation in SSc. (a) Keratinocyte precedes and modulates fibroblast dysregulation. (b) Fibroblast precedes and modulates keratinocyte dysregulation. Dashed lines indicate processes. The changes in the color of the nuclei indicate differential gene expression programs.
The first report addressing this issue took advantage from gene silencing of the transcription factor Friend leukemia virus integration 1 (Fli1) in keratinocytes [26]. Fli1 was known to be constitutively suppressed in dermal fibroblasts, dermal microvascular endothelial cells, and perivascular inflammatory cells in lesional and nonlesional SSc skin, therefore implicated in SSc pathogenesis. The authors generated keratin 14 (K14) – expressing epithelial cell-specific Fli1 knockout mice, which spontaneously developed dermal and esophageal fibrosis with epithelial activation. Furthermore, these mice developed autoimmunity and interstitial lung disease, thus demonstrating the potential instructive role of “altered” keratinocytes in SSc pathogenesis. As a note of caution in interpretating these findings, the authors were able to demonstrate that Fli1 directly regulated AIRE expression in epithelial cells including in the thymus and its absence resulted in down-regulation of autoimmune regulator (AIRE), a transcription factor involved in central tolerance. This leaves open the door on whether thymic abnormalities were also mechanistically responsible of the scleroderma-like phenotype developing in keratinocyte Fli1 KO mice [26].
Second, a manuscript recently deposited in bioRxiv shows that the transcription factor Snail is overexpressed in the epidermis of SSc patients and a transgenic mouse in which Snail is specifically hyper-expressed in keratinocytes under the K14 promoter is sufficient to induce several features of human SSc. Mechanistically, the authors show that the matricellular protein Mindin is produced by Snail transgenic skin keratinocytes and favor fibrogenesis by inducing inflammatory cytokines and collagen production in resident dermal fibroblasts [27].
Additional work should clearly provide further data in favor of an instructive role of keratinocytes in directing dermal fibrosis. Nonetheless, the evidence here summarized provides ground to address this interesting question.
CONCLUDING REMARKSThe observations that SSc epidermis has an abnormally increased number of stratified keratinocytes, that the expression of several keratinocyte products distinguish SSc from HD, that epidermal equivalents generated from primary SSc keratinocytes display a distinct gene expression program compared to the HD counterpart, that primary SSc keratinocytes cultured in vitro respond differently to exogenous stimuli compared to HD are all pieces of evidence indicating that SSc-specific molecular cues characterize keratinocytes and epidermis. These peculiarities may be primarily or secondarily part of wider SSc dysfunctions resulting, among others, in abnormal ECM deposition and fibrosis. Future work should address the question whether cell-autonomous keratinocyte abnormalities may drive secondary abnormalities in cells populating the dermis or whether they respond to cues generated in the SSc-dermis whether due to cell signals or structural constrains associated with fibrosis and increased dermal stiffness. Single cell gene expression studies investigating SSc in comparison to HD epidermis as well as improved methods of epidermis and skin in vitro engineering using primary cell lines generated from individuals affected by various clinical forms of early or late SSc should bring solid answers to these questions. In any case, it remains an attractive perspective the possibility of targeting keratinocyte abnormalities to harness clinical scleroderma, which continues to be an incurable disease.
AcknowledgementsNone.
Financial support and sponsorshipWork supported in part by grant 310030–159999 from the Swiss National Science Foundation (SNSF) to C.C.
Conflicts of interestC.C. has received honoraria from Boehringer Ingelheim and CSL Behring. Other authors declare no conflicts of interest in relationship to this manuscript.
REFERENCES AND RECOMMENDED READINGPapers of particular interest, published within the annual period of review, have been highlighted as:
▪ of special interest
▪▪ of outstanding interest
REFERENCES 1. Russo B, Brembilla NC, Chizzolini C. Interplay between keratinocytes and fibroblasts: a systematic review providing a new angle for understanding skin fibrotic disorders. Front Immunol 2020; 11:648. 2. Canady J, Arndt S, Karrer S, et al. Increased KGF expression promotes fibroblast activation in a double paracrine manner resulting in cutaneous fibrosis. J Invest Dermatol 2013; 133:647–657. 3. McCoy SS, Reed TJ, Berthier CC, et al. Scleroderma keratinocytes promote fibroblast activation independent of transforming growth factor beta. Rheumatology (Oxford) 2017; 56:1970–1981. 4. Aden N, Nuttall A, Shiwen X, et al. Epithelial cells promote fibroblast activation via IL-1alpha in systemic sclerosis. J Invest Dermatol 2010; 130:2191–2200. 5. Nikitorowicz-Buniak J, Shiwen X, Denton CP, et al. Abnormally differentiating keratinocytes in the epidermis of systemic sclerosis patients show enhanced secretion of CCN2 and S100A9. J Invest Dermatol 2014; 134:2693–2702. 6. Dufour AM, Borowczyk-Michalowska J, Alvarez M, et al. IL-17A dissociates inflammation from fibrogenesis in systemic sclerosis (scleroderma). J Invest Dermatol 2020; 140:026. 7. Henrot P, Laurent P, Levionnois E, et al. A method for isolating and culturing skin cells: application to endothelial cells, fibroblasts, keratinocytes, and melanocytes from punch biopsies in systemic sclerosis skin. Front Immunol 2020; 11:566607. 8. De Pieri A, Korman BD, Jungel A, et al. Engineering advanced in vitro models of systemic sclerosis for drug discovery and development. Adv Biol 2021; 5:e2000168. 9. Alsharabasy AM, Pandit A. Protocol for in vitro skin fibrosis model to screen the biological effects of antifibrotic compounds. STAR Protoc 2021; 2:100387. 10. Huang M, Cai G, Baugh LM, et al. Systemic sclerosis dermal fibroblasts induce cutaneous fibrosis through lysyl oxidase-like 4: new evidence from three-dimensional skin-like tissues. Arthritis Rheumatol 2020; 72:791–801. 11. Wang X, Liu Y, Deng Z, et al. Inhibition of dermal fibrosis in self-assembled skin equivalents by undifferentiated keratinocytes. J Dermatol Sci 2009; 53:103–111. 12▪▪. Huang M, Smith A, Watson M, et al. Self-assembled human skin equivalents model macrophage activation of cutaneous fibrogenesis in systemic sclerosis. Arthritis Rheumatol 2022; 74:1245–1256. 13. Matei AE, Chen CW, Kiesewetter L, et al. Vascularised human skin equivalents as a novel in vitro model of skin fibrosis and platform for testing of antifibrotic drugs. Ann Rheum Dis 2019; 78:1686–1692. 14. Luchetti MM, Moroncini G, Jose Escamez M, et al. Induction of scleroderma fibrosis in skin-humanized mice by administration of anti-platelet-derived growth factor receptor agonistic autoantibodies. ArthritisRheumatol 2016; 68:2263–2273. 15. Vijayaraj P, Minasyan A, Durra A, et al. Modeling progressive fibrosis with pluripotent stem cells identifies an antifibrotic small molecule. Cell Rep 2019; 29:3488.e9–3505.e9. 16. Ingber DE. Human organs-on-chips for disease modelling, drug development and personalized medicine. Nat Rev Genet 2022; 23:467–491. 17. Inamo J. Association of differentially expressed genes and autoantibody type in patients with systemic sclerosis. Rheumatology (Oxford) 2021; 60:929–939. 18. Skaug B, Khanna D, Swindell WR, et al. Global skin gene expression analysis of early diffuse cutaneous systemic sclerosis shows a prominent innate and adaptive inflammatory profile. Ann Rheum Dis 2020; 79:379–386. 19. Mahoney JM, Taroni J, Martyanov V, et al. Systems level analysis of systemic sclerosis shows a network of immune and profibrotic pathways connected with genetic polymorphisms. PLoS Comput Biol 2015; 11:e1004005. 20▪▪. Russo B, Borowczyk J, Boehncke WH, et al. Dysfunctional keratinocytes increase dermal inflammation in systemic sclerosis. Results from tissue-engineered scleroderma epidermis. Arthritis Rheumatol 2021; 73:1311–1317. 21. Truchetet ME, Brembilla NC, Chizzolini C. Current concepts on the pathogenesis of systemic sclerosis. Clin Rev Allergy Immunol 2021; doi: 10.1007/s12016-021-08889-8. [Online ahead of print]. 22▪. Russo B, Borowczyk J, Cacialli P, et al. IL-25 participates in keratinocyte-driven dermal matrix turnover and is reduced in Systemic Sclerosis epidermis. Rheumatology (Oxford) 2022; keac044doi: 10.1093/rheumatology/keac044. [Online ahead of print]. 23. Kudo H, Wang Z, Jinnin M, et al. EBI3 downregulation contributes to type i collagen overexpression in scleroderma skin. J Immunol 2015; 195:3565–3573. 24. Saito A, Ichimura Y, Kubota N, et al. IFN-γ-stimulated apoptotic keratinocytes promote sclerodermatous changes in chronic graft-versus-host disease. J Invest Dermatol 2021; 141:1473.e4–1481.e4. 25. Zhang S, Zhang Y, Min P. Single-cell and bulk transcriptome data integration reveals dysfunctional cell types and aberrantly expressed genes in hypertrophic scar. Front Genet 2021; 12:806740. 26. Takahashi T, Asano Y, Sugawara K, et al. Epithelial Fli1 deficiency drives systemic autoimmunity and fibrosis: possible roles in scleroderma. J Exp Med 2017; 214:1129–1151. 27. Rana I, Kataria S, Tan TL, et al. Mindin is essential for cutaneous fibrogenesis in a new mouse model of systemic sclerosis. bioRxiv 2022; https://doi.org/10.1101/2022.01.26.477822
留言 (0)