
記住我










Pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH) are progressive diseases that can lead to right heart failure and death. Right ventricular dysfunction, hypertrophy and maladaptive remodelling are consequences of increased right ventricular (RV) afterload in PAH and CTEPH and are indicative of long-term outcomes. Because RV failure is the main cause of morbidity and mortality in PAH and CTEPH, successful treatments should lead to improvements in RV parameters. Riociguat is a soluble guanylate cyclase stimulator approved for the treatment of PAH and inoperable or persistent/recurrent CTEPH after pulmonary endarterectomy. This review examines the current evidence showing the effect of riociguat on the right ventricle, with particular focus on remodelling, function and structural parameters in preclinical models and patients with PAH or CTEPH.
AbstractRaymond L. Benza (@OSUWexMed) and co-authors review the current evidence showing the effect of riociguat on right ventricle remodelling, function and structural parameters in preclinical models and patients with #PAH or #CTEPH. #pulmonaryhypertension https://bit.ly/3Q9icVm
IntroductionPulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH) are progressive diseases that can lead to right heart failure and death [1]. The mechanisms underlying PAH and CTEPH involve complex and multifactorial changes in the pulmonary vasculature, which lead to increased pulmonary vascular resistance (PVR) and right ventricular (RV) remodelling, including increasing contractility to maintain coupling [1–4]. Initially compensatory, RV remodelling can become maladaptive owing to increased long-term RV afterload, a key determinant in PAH and CTEPH, resulting in RV hypertrophy, uncoupling and dysfunction [1–5]. Importantly, right heart function [6–13] and size [14–17] are prognostic factors in PAH and CTEPH. It therefore follows that any effective treatment for PAH or CTEPH must improve parameters of RV function.
Cyclic guanosine monophosphate (cGMP) signalling is directly involved in various cardiac and vascular muscle functions, including growth, relaxation and vasodilation. In the myocardium, cGMP signalling can modulate the cardiac stress response and indirectly reduce maladaptive hypertrophy [18]. Circulating cGMP is regulated by two important enzymes, soluble guanylate cyclase (sGC), which stimulates production of cGMP, and phosphodiesterase type 5 (PDE5), which catalyses its breakdown [19]. Production of sGC is stimulated by nitric oxide (NO), which is downregulated in patients with PAH [20]. Furthermore, PDE5 expression and activity are increased in the smooth muscle cells of the pulmonary artery (PA) and in the RV myocardium [21]. Thus, levels of cGMP are decreased in patients with PAH, leading to vasoconstriction and smooth muscle cell proliferation. Riociguat is an sGC stimulator approved for the treatment of PAH and inoperable or persistent/recurrent CTEPH after pulmonary endarterectomy (PEA) [22, 23]. It acts to increase cGMP levels by two separate mechanisms: first, it stabilises NO binding to sGC, and second, it directly stimulates sGC independent of NO. In the pulmonary circulation, this leads to vascular smooth muscle cell relaxation [24].
The phosphodiesterase type 5 inhibitors (PDE5i) sildenafil and tadalafil also act on the NO–sGC–cGMP pathway, increasing cGMP levels by inhibiting its breakdown [19]. Unlike sGC inhibitors, the efficacy of PDE5i requires that the NO–sGC–cGMP pathway is functional and producing intracellular cGMP. The reduced levels of NO and cGMP in patients with PAH potentially limit the efficacy of PDE5i [19]. Given that riociguat and PDE5i act on the same pathway, it is possible that these agents have an additive vasodilatory effect when used in combination. This is supported by data from the PATENT PLUS study, in which the combination of riociguat and sildenafil in patients with PAH was associated with a substantial reduction in standing systolic blood pressure (though not diastolic blood pressure or supine systolic blood pressure) compared with riociguat alone, and a high rate of discontinuation due to hypotension [25]. In the absence of a positive risk/benefit ratio, the combination of riociguat with a PDE5i is contraindicated.
The most common adverse events occurring during riociguat treatment are consistent with its mode of action and similar to those with other vasodilators, including headache, dizziness, dyspepsia, peripheral oedema, nausea, diarrhoea and vomiting [26, 27]. Vasodilation can also lead to hypotension, and vasodilators such as riociguat should therefore be used with caution in patients with underlying conditions that might be adversely affected by vasodilatory effects [23]. Riociguat should also be avoided in patients with a history of serious haemoptysis or who have previously undergone bronchial arterial embolisation. Riociguat is administered as oral tablets three times daily, which may have implications for treatment adherence compared with other oral agents for PAH that are given once or twice daily.
This review examines the current evidence showing the effects of riociguat on the right ventricle in preclinical models and patients with PAH or CTEPH (figure 1).
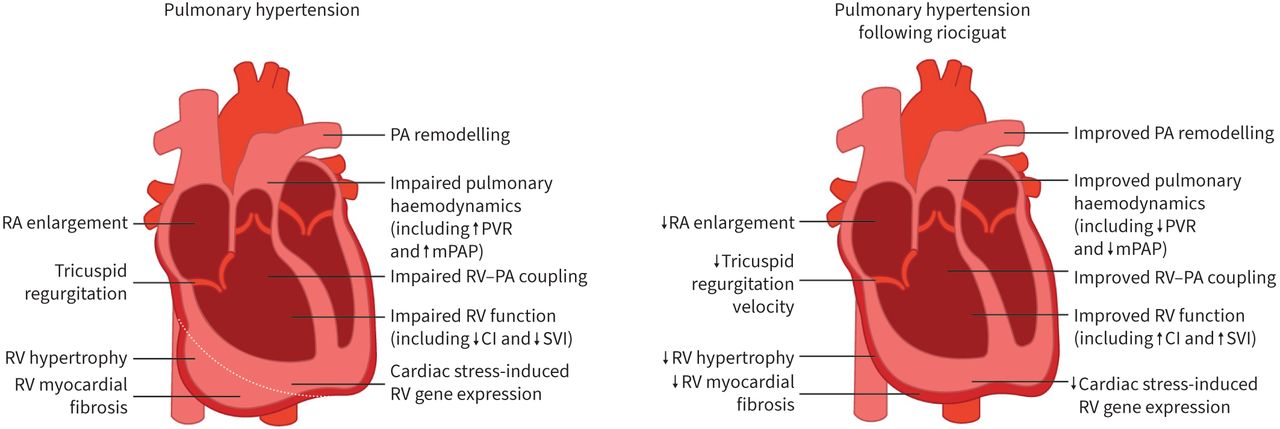 FIGURE 1
FIGURE 1 Effects of riociguat on the right ventricle in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. White dotted line indicates the position of the right ventricular (RV) wall in a healthy heart. RA: right atrium; PA: pulmonary artery; PVR: pulmonary vascular resistance; mPAP: mean pulmonary arterial pressure; CI: cardiac index; SVI: stroke volume index.
Effect of riociguat on the right ventricle in preclinical modelsRiociguat has demonstrated positive effects on the right ventricle in several preclinical models of pulmonary hypertension (PH) (supplementary table S1).
Various factors of RV function [28–32] are improved with riociguat compared with vehicle-treated controls in rodent models of PH induced by drugs, hypoxia, cigarette smoke exposure and transverse aortic constriction. Following riociguat, improvement of load-dependent parameters and a partial reversal of RV hypertrophy have been observed in several preclinical models [28–32]. Riociguat also improves vascular remodelling [28, 30–32], reduces RV fibrosis [30] and decreases cardiac stress-induced gene expression [28] compared with controls.
Several studies have compared the effects of riociguat and sildenafil in the same animal model. Both riociguat and sildenafil prevented worsening of RV function compared with controls in rodent models of drug-, smoke- or aortic constriction-induced PH [29, 30, 32]. Improvements of PH haemodynamic parameters [29, 30] and RV hypertrophy [29] with riociguat were greater than those observed with sildenafil treatment alone.
It is difficult to determine, based on the rodent models mentioned above and the available clinical literature, whether the improvements in RV size and function are due to the effects of riociguat on the right ventricle or on the pulmonary vasculature. However, results from a rodent model of pressure overload RV hypertrophy induced by PA banding have shown that riociguat is associated with right ventricle-specific effects, including significantly improved RV ejection fraction, RV end-systolic volume and RV end-diastolic volume, and a numeric improvement in RV stroke volume [33]. In the same model, both riociguat and sildenafil prevented worsening of RV function, and riociguat, but not sildenafil, also prevented RV fibrosis, with a reduction of collagen content to nearly half of that in the placebo group [33]. Sildenafil was, however, found to attenuate fibrosis in a bleomycin-induced pulmonary fibrosis model [34]. Overall, these results suggest that riociguat can have direct effects on the right ventricle.
Effect of riociguat on RV function in clinical studiesSeveral echocardiographic measurements of RV function are impaired in patients with PH, including RV ejection fraction, tricuspid annular plane systolic excursion (TAPSE), fractional area change and global longitudinal strain. Importantly, RV parameters and haemodynamic variables are associated with long-term outcomes in patients with PAH [6–10, 13] or CTEPH [11, 12]. As outlined in table 1, several studies have shown that riociguat has positive effects on RV function in patients with PAH or CTEPH.
TABLE 1Overview of the effects of riociguat on the right ventricle in clinical studies
In the prospective randomised controlled phase III trials PATENT-1 and CHEST-1, improvements in exercise capacity, serum N-terminal pro-brain natriuretic peptide levels, World Health Organization functional class and haemodynamic parameters (mean pulmonary arterial pressure (mPAP), PVR and cardiac output (CO)) were seen with riociguat treatment in patients with PAH or CTEPH, respectively [26, 27]. Following riociguat, a range of haemodynamic parameters, including PVR, cardiac index, mPAP and systemic vascular resistance, were improved in both pre-treated and treatment-naïve patients in PATENT-1 [46] and in patients with inoperable CTEPH and persistent/recurrent CTEPH post-PEA in CHEST-1 [47].
Impact of riociguat on echocardiographic parameters of RV functionA retrospective single-centre echocardiographic study of 39 patients (54% with PAH and 46% with CTEPH) who participated in PATENT-1 and CHEST-1, the long-term extension trials PATENT-2 and CHEST-2, the CTEPH Early Access Study and PATENT PLUS (which evaluated riociguat in combination with sildenafil in patients with PAH) evaluated the effect of riociguat on right heart size and function [35]. At both 6 and 12 months, TAPSE improved compared with baseline values. Tricuspid annular velocity, as measured by S’ wave tissue Doppler imaging, was also improved at 12 months. Data from right heart catheterisation showed that riociguat was also associated with a reduction in PVR, systolic pulmonary arterial pressure and mPAP, and an increase in CO and cardiac index at 3 months compared with baseline.
Similar effects on RV function assessed by echocardiography were found in a retrospective multicentre study of 71 patients (45% PAH, 55% CTEPH) from CHEST, PATENT, PATENT PLUS and the CTEPH Early Access Study [36]. The RIVER study showed that after 12 months of riociguat treatment, patients showed improvements in TAPSE, fractional area change, tricuspid regurgitation velocity and qualitatively assessed RV systolic function.
Impact of riociguat on speckle-tracking echocardiographic parametersIn addition to conventional echocardiographic parameters, the effect of riociguat on RV contractile function was assessed using speckle-tracking echocardiography in 27 patients with PH (26% PAH, 74% CTEPH) [37]. Compared with baseline, riociguat administration significantly improved RV systolic function, including RV fractional area change and RV global longitudinal strain (even after adjusting for RV afterload), although no changes were observed in TAPSE or RV S’ wave.
Similar findings with riociguat in 45 patients with PH (31% PAH, 69% CTEPH) were seen in an expanded analysis by the same investigators [38]. Additionally, improvements with riociguat were seen in patients with mild PH who had previously undergone balloon pulmonary angioplasty (BPA) or PEA for CTEPH [38].
Impact of riociguat on haemodynamic parameters of RV functionA recent post hoc analysis of haemodynamic data from PATENT-1 and CHEST-1 investigated whether riociguat improved RV function parameters, including stroke volume, stroke volume index (SVI), RV work index, RV power and cardiac efficiency [39]. Additionally, the association between RV function parameters and SVI/right atrial pressure (RAP) with long-term outcomes in PATENT-2 and CHEST-2 was determined. Riociguat improved RV function parameters in PATENT-1 and CHEST-1 compared with placebo. The Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) risk score was negatively correlated with SVI and positively correlated with RAP at baseline and follow-up in both PATENT-1 and CHEST-1. Multiple RV function parameters at baseline and follow-up were associated with survival and clinical worsening-free survival in PATENT-2 and CHEST-2 (table 1). In PATENT-2, a favourable SVI/RAP (SVI ≥31 mL·beat−1·m−2 and RAP <10 mmHg) at follow-up was significantly associated with survival and clinical worsening-free survival. In CHEST-2, favourable SVI/RAP at baseline and follow-up were significantly associated with survival and clinical worsening-free survival.
Improvement in RV haemodynamic parameters was also seen in a study of 21 patients with CTEPH who had experienced haemodynamic improvement after BPA and had subsequently received riociguat or standard of care [40]. Significant improvements were seen in CO and PVR during exercise in those who received riociguat compared with controls. In addition, the slope of the linearised mPAP–CO relationship was significantly decreased from baseline in the riociguat group but not in the control group.
Impact on RV function of switching to riociguat from PDE5i therapyThe prospective single-arm open-label RESPITE study investigated the impact of switching to riociguat to optimise treatment [48]. A post hoc analysis of haemodynamic data from the RESPITE study demonstrated improvement in several key RV parameters after 61 patients with PAH with insufficient treatment response switched to riociguat from PDE5i [41]. Improvements compared with baseline in cardiac efficiency, stroke volume and SVI were observed after switching to riociguat. Other RV parameters, including RV work, RV work index, PA elastance and RV power, were all maintained after switching [41]. At week 24, 69% of responders to riociguat treatment had achieved a favourable SVI and RAP compared with 48% of non-responders [49].
A retrospective study evaluating switching from sildenafil to riociguat in 28 patients with inoperable or persistent CTEPH after PEA found that switching resulted in improvement of several haemodynamic parameters, including reductions in PVR, systemic vascular resistance and mPAP, and an increase in CO [42]. Switching also significantly decreased the number of patients with World Health Organization functional class III/IV symptoms.
Impact of riociguat combination therapy and other PAH-targeted therapies on RV functionThe efficacy of riociguat as part of triple combination therapy with macitentan and selexipag was evaluated in 26 patients in a retrospective study conducted at a single Japanese centre [43]. Over a median observation period of 441 days, improvements of 29%, 65% and 82% were reported in mPAP, PVR and CO, respectively. Additionally, RV function parameters such as TAPSE and RV systolic excursion velocity were significantly improved from baseline to follow-up.
RV function was also improved in patients with PAH undergoing treatment with pharmacological therapies other than riociguat, including inhaled iloprost [50, 51], bosentan [52, 53], sildenafil [54, 55], ambrisentan [56] and the following combination therapies: endothelin receptor antagonist (ERA) or PDE5i plus parenteral prostanoid [57], ERA plus PDE5i [57], ambrisentan plus tadalafil [58], and ambrisentan plus tadalafil plus subcutaneous treprostinil [59]. In patients with CTEPH, RV function was improved following therapy with bosentan [60] and sildenafil [61], and surgical treatment with PEA [62, 63] and BPA [64–67].
Effect of riociguat on RV hypertrophy in clinical studiesRV wall stress, due to an increased and mismatched afterload, results in adaptive concentric hypertrophy to maintain RV diastolic volume and CO [68, 69]. If the right ventricle is not able to develop adequate hypertrophy, it starts to dilate. Right heart size parameters, such as RV enlargement, are associated with long-term outcomes in PAH [14–16] and CTEPH [17]. Several studies have shown that riociguat improves right heart hypertrophy in patients with PAH or CTEPH (table 1).
Impact of riociguat on echocardiographic parameters of RV sizeMarra et al. [35] investigated change in RV function and change of RV size with riociguat treatment using echocardiography. After 3, 6 and 12 months of therapy, mean RV area was significantly reduced compared with baseline values. Similarly, right atrial area continually decreased from 3 months and was significantly reduced at 12 months compared with baseline. Riociguat was also associated with a significant reduction in RV free wall thickness at all time points, suggesting reversed hypertrophy. Improved RV remodelling, assessed by the left ventricular eccentricity index, was also seen at 6 and 12 months.
Similar results were observed in the RIVER study [36]. Patients who completed echocardiographic assessments at baseline, 3, 6 and 12 months showed a significant reduction of right atrial and RV area at all time points (figure 2). Additionally, RV thickness and PA diameter were reduced after 12 months compared with baseline, suggesting attenuation of hypertrophy and improved remodelling. However, the RIVER study was limited by a lack of statistical comparison with the placebo control group owing to small sample sizes. In a recent retrospective analysis of patients with PAH or CTEPH, riociguat induced reverse RV remodelling, with significant decreases in several echocardiographic parameters of RV hypertrophy [38], including RV diameter, RV end-diastolic and end-systolic area indices and increased fractional area change.
 FIGURE 2
FIGURE 2 Patients with pulmonary hypertension receiving riociguat show a significant reduction in right atrial (RA) and right ventricular (RV) areas compared with baseline at all time points. Figure modified from Marra et al. [36] and redistributed under the Creative Commons Attribution 4.0 International license: https://creativecommons.org/licenses/by/4.0/legalcode. #: compared to baseline.
Impact of riociguat combination therapy and other PAH-targeted therapies on RV sizeIn a retrospective analysis of patients receiving riociguat in combination with macitentan and selexipag, significant improvements were seen in echocardiographic parameters, including fractional area change and RV end-systolic area, after a median follow-up of 441 days [43].
Sildenafil monotherapy [54], ambrisentan monotherapy [56] and combination therapies of ERA or PDE5i plus parenteral prostanoid [57], ERA plus PDE5i [57], and ambrisentan plus tadalafil plus subcutaneous treprostinil [59] have also been shown to improve RV morphology in patients with PAH. In patients with CTEPH, RV hypertrophy was reduced after PEA [70, 71] and BPA [66, 72]. In addition, RV size was positively associated with surgical success after PEA [71].
Effect of riociguat on other aspects of RV remodelling in clinical studiesAlongside RV hypertrophy, additional aspects of cardiac remodelling can be prognostic of outcome in PH [73–76]. Myocardial fibrosis occurs as a response to increased RV afterload and can be associated with RV wall stiffness, injury and inflammation [77, 78]. Coupling of RV systolic function to afterload is maintained by RV hypertrophy until dilation occurs at end-stage PH and results in uncoupling and reduced CO [4]. The maintenance of RV–PA coupling is therefore important for RV functional adaptation and is predictive of survival in patients with PH [75, 76]. Preliminary evidence suggests a beneficial effect of riociguat on cardiac remodelling in patients with CTEPH or PAH (table 1).
As shown by a significant reduction in basal RV diameter and RV end-diastolic area index, Murata et al. [37] found that RV remodelling was ameliorated in patients with PH after riociguat administration. The effect of riociguat on RV remodelling was also assessed in a prospective study of six patients with CTEPH [44]. Six months of riociguat treatment was associated with a significant increase of RV SVI and a nonsignificant trend of RV ejection fraction improvement compared with baseline. Myocardial fibrosis was reduced, as indicated by the volume and mass of myocardium exhibiting late gadolinium enhancement, in five out of six patients. After 1 year of riociguat treatment, all six patients were clinically stable and showed no decline in RV function, RV size, tricuspid regurgitation or pulmonary pressures.
A pilot study of 20 patients with PAH (12 patients who were treatment-naïve and eight patients who switched from sildenafil to riociguat therapy) evaluated the effect of riociguat on right heart remodelling and RV–PA coupling [45]. Following 12 weeks of riociguat treatment, a reduction in RV basal diameter compared with baseline was observed in treatment-naïve patients. RV–PA coupling decreased in both the treatment-naïve and treatment-switch subgroups due to a decrease in PA effective arterial elastance and an increase in RV end-systolic elastance. Improvements in RV end-systolic volume and RV fractional area change were also observed following riociguat treatment.
RV remodelling also improves in patients with CTEPH following PEA [63, 70, 79], BPA [67, 72] and bosentan treatment [60] and in patients with PAH following ambrisentan, tadalafil and subcutaneous treprostinil combination therapy [59]. The degree of remodelling varies between therapies, with a generally greater improvement seen following surgical treatment compared with drug therapy; however, due to differences in end-points and methodologies between these studies it is difficult to determine the level of remodelling required for therapeutic significance.
Points for clinical practice• Right heart function and size are prognostic factors in both PAH and CTEPH.
• Clinical data suggest that riociguat exerts beneficial effects on RV remodelling.
• Inclusion of RV imaging in PH trial end-points could be valuable.
ConclusionsMaladaptive remodelling and RV dysfunction are consequences of increased long-term RV afterload in PAH and CTEPH [1–3], with associated parameters indicative of long-term outcomes [6–9, 11, 12, 14–17, 73]. Because RV failure is the main cause of morbidity and mortality in PAH and CTEPH, successful treatments should lead to improvements in RV parameters. In both preclinical and clinical studies, riociguat has demonstrated a beneficial impact on RV structure and function. It should be noted that several of the clinical studies discussed in this review were retrospective analyses [35–37, 39, 41] or small pilot studies that were not randomised or placebo-controlled [44, 45]. Further large-scale randomised controlled studies are therefore needed to confirm these findings. In addition, it is difficult to distinguish the effects of riociguat on the right ventricle independent of its pulmonary vascular effects. While clinical studies do not reveal whether riociguat has direct beneficial effects on the right ventricle, animal studies strongly suggest that this is the case.
Supplementary materialSupplementary MaterialPlease note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material err-0061-2022.supplement
AcknowledgementsMedical writing services were provided by Rachael Powis, PhD, of Adelphi Communications Ltd (Macclesfield, UK) funded by Bayer AG (Berlin, Germany) in accordance with Good Publications Practice (GPP3).
FootnotesProvenance: Submitted article, peer reviewed.
Conflict of interest: R.L. Benza reports receiving grants from Actelion, Bayer AG, Bellerophon Therapeutics and Eiger Biopharmaceuticals.
Conflict of interest: D. Langleben reports receiving honoraria, consultation fees, research support and/or travel expenses from Acceleron Pharma, Actelion, Arena Pharmaceuticals, Bayer AG, Northern Therapeutics, PhaseBio and United Therapeutics outside the submitted work.
Conflict of interest: A.R. Hemnes has received grants from the NIH and CMREF. She has served as a consultant to Acceleron Pharma, Bayer, Gossamer Bio, Janssen Pharmaceuticals and United Therapeutics. She holds stock in Tenax Therapeutics.
Conflict of interest: A. Vonk Noordegraaf is supported by the Netherlands CardioVascular Research Initiative (CVON-2012-08 PHAEDRA, CVON-2017-10 DOLPHIN-GENESIS) and the Netherlands Organization for Scientific Research (NWO-VICI: 918.16.610), has received speaker fees from Ferrer and Johnson & Johnson in the past 3 years and has served as a member of the scientific advisory board of Morphogen-XI.
Conflict of interest: S. Rosenkranz reports remunerations for lectures and/or consultancy from Abbott, Acceleron Pharma, Actelion, Arena Pharmaceuticals, Bayer AG, Bristol Myers Squibb, Ferrer, GlaxoSmithKline, Janssen Pharmaceuticals, Merck Sharp & Dohme Corp., Novartis, Pfizer and United Therapeutics; and research support to his institution from Actelion, Bayer, Novartis, Pfizer and United Therapeutics outside the submitted work.
Conflict of interest: T. Thenappan reports consultation fees from Actelion and United Therapeutics outside the submitted work.
Conflict of interest: P.M. Hassoun is serving on a scientific advisory board for Merck & Co.
Conflict of interest: I.R. Preston reports grants and personal fees from Actelion, Arena Pharmaceuticals, Bayer AG, Gilead Sciences and United Therapeutics; grants from Liquidia; and personal fees from Pfizer and Reata Pharmaceuticals outside the submitted work.
Conflict of interest: S. Ghio has nothing to disclose.
Conflict of interest: R. Badagliacca reports grants from Bayer, Dompè, Merck Sharp & Dohme Corp., Ferrer, Galenica, GlaxoSmithKline, Janssen Pharmaceuticals and United Therapeutics.
Conflict of interest: C.D. Vizza reports fees for lectures and/or consultations from Acceleron Pharma, Actelion, Bayer, GlaxoSmithKline, Merck Sharp & Dohme Corp. and United Therapeutics outside the submitted work.
Conflict of interest: I.M. Lang has served as a steering committee member for Actelion and has received speaker fees and grants from Actelion, AOP Orphan Pharmaceuticals, Ferrer and United Therapeutics outside the submitted work.
Conflict of interest: C. Meier is an employee of Bayer AG.
Conflict of interest: E. Grünig reports fees for lectures and/or consultations from Actelion, Bayer AG, GlaxoSmithKline, Merck Sharp & Dohme Corp., Pfizer and United Therapeutics outside the submitted work.
Support statement: The PATENT, CHEST and RIVER studies were funded by Bayer AG (Berlin, Germany) and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc. (Rahway, NJ, USA). Funding information for this article has been deposited with the Crossref Funder Registry.
Received April 8, 2022.Accepted July 22, 2022.Copyright ©The authors 2022http://creativecommons.org/licenses/by-nc/4.0/This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissionsersnet.org
留言 (0)