Visual and aberrometric changes
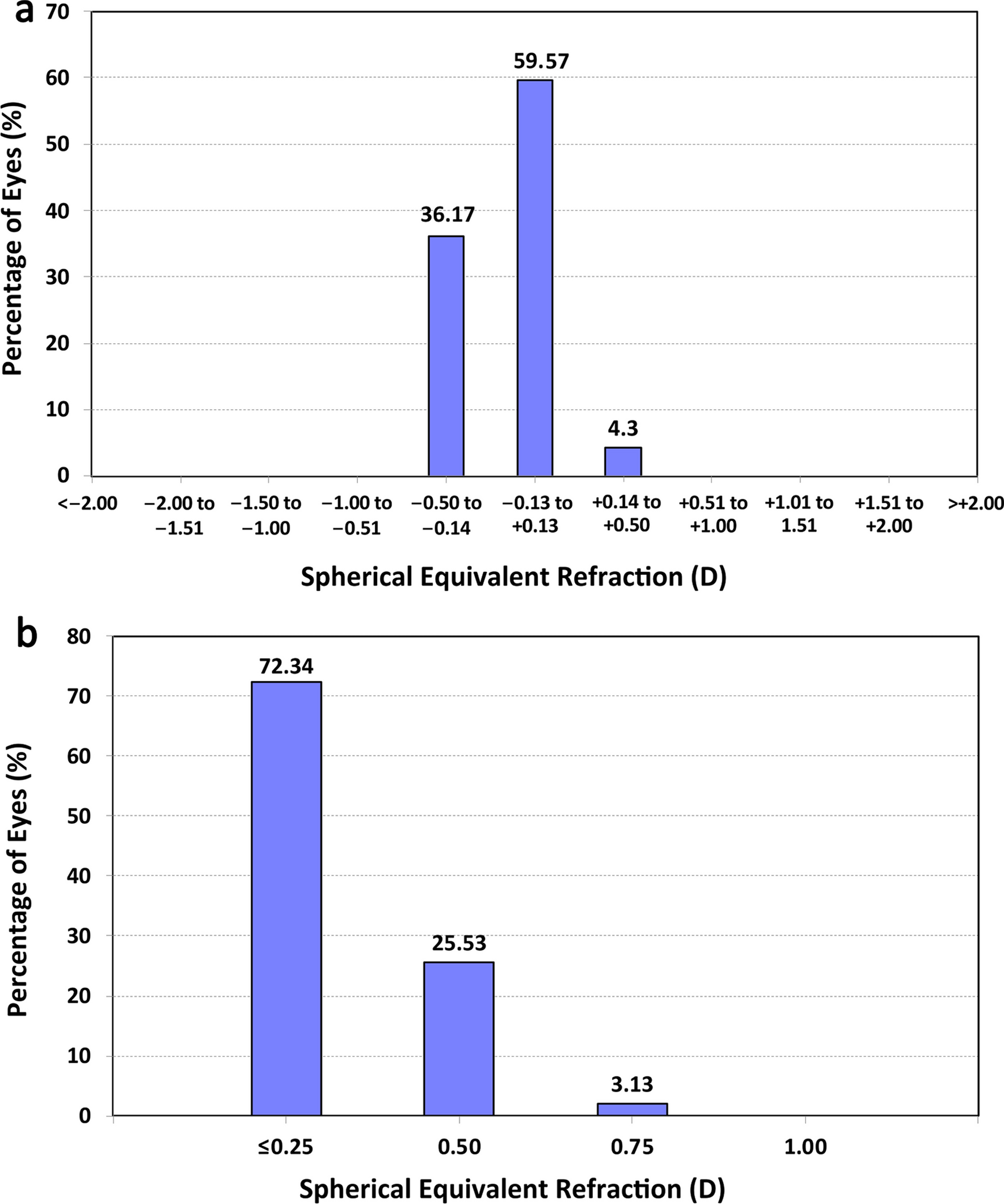
In this study, changes occurring with the fitting of a specific model of SCL in corneas with KC were observed over a 3-month period. Factors correlating with visual improvement and a model to predict any improvement were investigated. A statistically significant improvement in VA has been observed in our sample of KC eyes, which is consistent with the results of previous clinical studies [6, 16, 22, 26, 27]. This good efficacy in terms of visual rehabilitation with the SCL was consistent with the efficacy in terms of optical correction, with mean ORx close to 0.00 D during the entire follow-up. Suarez et al. [6]. evaluated the efficacy and safety of the same SCL used in the current study, reporting a mean SLVA of 0.16 ± 0.25 logMAR and an improvement in VA of 2 or more lines in 56% of the eyes. This finding is consistent with those obtained in the current series in which mean SLVA was 0.10 ± 0.04 logMAR and 44.76% of the eyes reached an improvement in VA of 2 or more lines. This percentage was lower than that reported in the study by Suarez et al. [6] This can be explained by the fact that these authors started from a worse mean baseline VA (0.44 ± 0.45 logMAR), which is, according to our analysis, an advantageous situation for VA improvement. It should be remembered that a negative correlation between VA change and pre-fitting CDVA was found, which implies that subjects with worse pre-fitting CDVA experienced more improvement in VA with the SCL evaluated. Regarding VA changes between 1 and 3 months of CL wear, they were small in magnitude and not statistically significant, suggesting a stability of the VA during this period. This stability should be also confirmed in the long term.
The improvement in VA observed in our sample was associated with a significant change in ocular HOAs. Specifically, a significant decrease was observed with the CL in HOA and primary coma RMS, confirming the ability of this type of CL to minimize the aberrations that are present in KC eyes and to improve the ocular optical quality. However, the residual aberrations through SCLs were not always within the normative data for age and pupil size, which would have been the ideal situation [28, 29]. This was not always possible due to the presence of a not fully optimized meniscus in all cases in spite of adjusting most SCL parameters (it should be considered that no quadrant-specific designs were used), and even some patients could have some level of amblyopia associated. Furthermore, anterior corneal aberrations can be neutralized with the meniscus, but not always aberrations arising from the posterior corneal surface. Indeed, mean VA with the SCL was 0.10 ± 0.04 logMAR at the end of the follow-up and not all eyes reached the standard “20/20 or better VA”. This is consistent with previous series reporting that a great portion of KC patients fitted with SCLs do not reach normative levels for aberrations [30]. Additionally, a significant correlation was found between the decrease in comatic aberration and the improvement in VA (r = − 0.775, P = 0.041). In this way, eyes with higher amounts of coma improved more after SCL fitting than eyes with lower levels of coma. In our series, there were 31% of eyes that did not improve VA after the SCL fitting and this was largely due to the presence of low amounts of coma aberrations as the KC was central or was incipient. This should be considered when fitting SCLs, as those eyes with less visual loss and lower levels of visual quality are expected to show minimal or limited improvements. Montalt et al. [27] also showed a decrease in ocular coma and HOAs with the use of a SCL, with a 55% decrease of total HOAs. These authors commented that despite this reduction, the aberration values with the SCL in KC were still higher than in normal corneas, suggesting that despite masking the irregularities of the corneal surface, aberrations on the posterior surface of the cornea and internal aberrations are not compensated [27]. Alipour et al. [18] also observed a statistically significant reduction in coma and trefoil aberrations with the use of SCLs in eyes with KC implanted with intracorneal ring segments.
Concerning the correlations of pre-fitting variables with the VA change achieved with the SCL evaluated, they were statistically significant for spectacle CDVA, anterior and posterior corneal astigmatism, posterior keratometry, MCT, anterior and posterior HOAs and the power of the CL. This confirms that the VA change achievable with the SCL evaluated in KC corneas can be predicted using all these variables, although the level of accuracy is not similar for all of them. The strongest correlation was found between the VA change and the pre-fitting CDVA value and it was negative. This means that patients with the worst initial VA were those who presented the greatest visual improvement with the fitting of the SCL. Considering that those eyes with worse VA are normally KC eyes with more aberrated corneas, it is normal that better VA would be expected as more ocular optical quality can be induced [16]. Indeed, the rest of significant correlations detected revealed that more VA improvement could be achieved in those eyes with more significant signs associated to moderate to severe stages of KC, such as higher levels of anterior and posterior corneal astigmatism, higher amounts of HOAs, greater curvature of the posterior corneal surface and lower MCT [31, 32].
Post-lens meniscus characterization
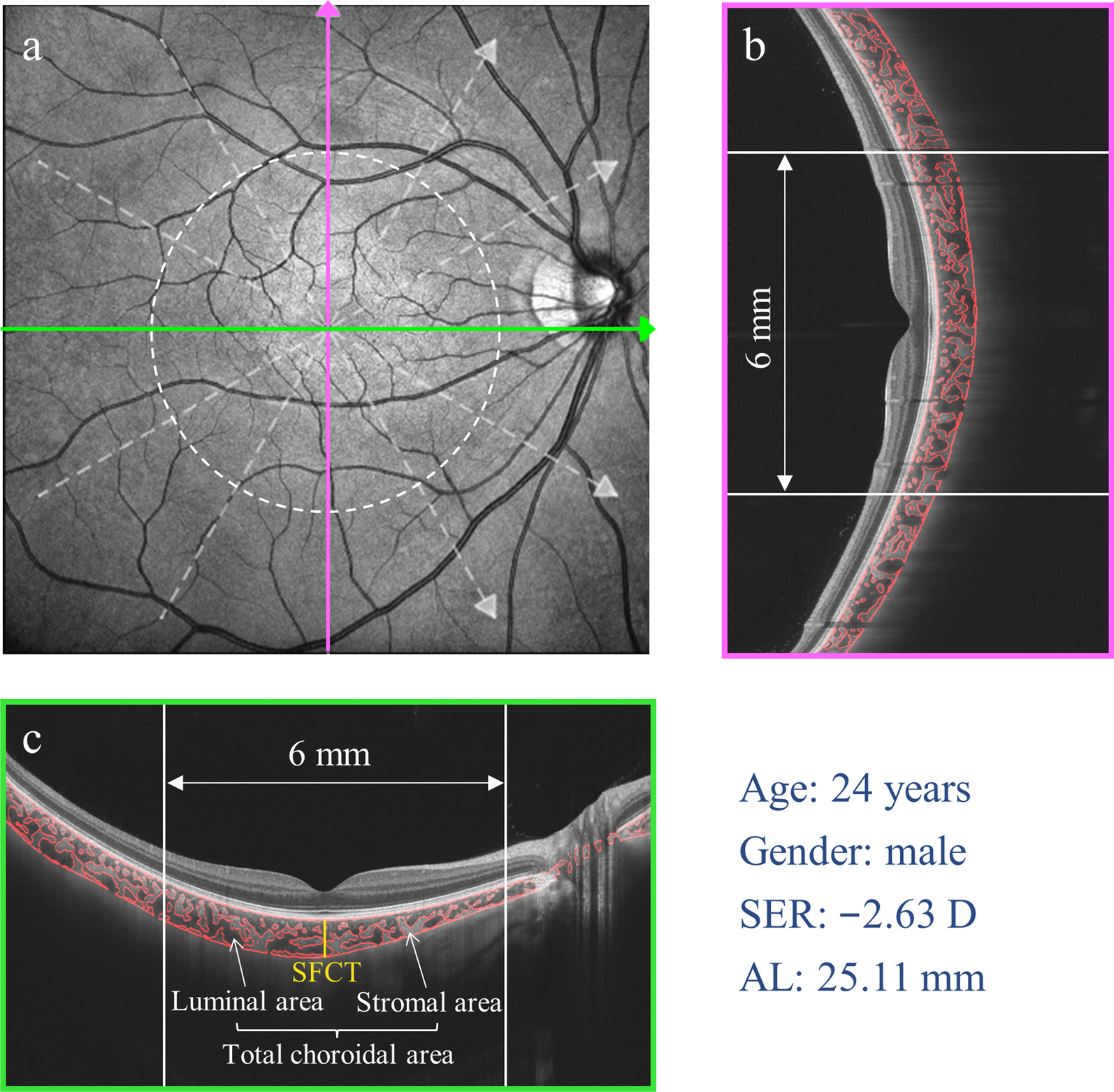
The characterization of the post-lens meniscus by OCT showed that the central, nasal, and temporal vaults decreased significantly after 1 month of SCL wear. This is the result of the progressive indentation of the periphery of SCL into the conjunctival tissue [33]. Vincent et al. [34] found that the central vault of the ICD16.50 SCL significantly decreased an average of 76 ± 8 μm after 8 h of use. Furthermore, they observed that 50% of the reduction occurred in the first 45 min, 75% in 2 h and after 4 h of use the decrease was not statistically significant [34]. Likewise, these authors found a statistically significant but not clinically relevant change associated in ORx [34]. Similarly, a reduction of the vault has been reported with other SCL designs. Bray et al. showed a decrease in the vault of 83 ± 22 μm after 6–8 h of CL use, with statistically significant changes in ORx associated [35]. Rathi et al. [36] observed a decrease in the central vault in 90% of their sample after 4 h of use of a SCL, ranging from an initial value of 680 ± 421 μm to 589 ± 355 μm. Courey and Michaud [37] showed a decrease in the central vault of 70 ± 9.8 μm after 6 h of use of a specific model of SCL. Otchere et al. [38] evaluated the decrease in the central vault of 3 different types of SCLs, obtaining a mean value of 34 ± 48 μm after 1 h of use. Furthermore, these authors observed that the vault loss depended on the initial magnitude of the vault. These mean decreases reported in previous studies were close to those obtained in our sample after 1 month of CL wear. Furthermore, previous studies indicate that most changes in SCL vault occurred in the initial period of CL wear, no significant changes were found in our sample in the characterization of horizontal post-lens meniscus between the first and third months of CL wear.
A significant difference between the nasal and temporal vault was found in our sample during the initial post-fitting period which could be due to a temporal decentration of the SCL, a greater indentation in the nasal area or a decentered CL position as a consequence of the asymmetry of the corneal surface in KC [39]. Courey and Michaud [37] showed a smaller vault on the nasal side than on the temporal that was attributed by the authors to the toric nature of the sclera. Concerning the difference in nasal-temporal vault in our study over time, it was not statistically significant after 3 months of CL use, which could indicate that the SCL stabilizes over time. This may be related to some level of conjunctival molding with the use of the SCL over time, as has been demonstrated using Fourier-domain profilometry to characterize the corneo-scleral profile [33].
Considering the distribution of the sagittal heights of the SCL fitted that were needed in the sample and that most eyes had a KC grade I and II, it can be concluded that a trial lens with a sagittal height between 4000 and 4400 µm is needed. This can be used for fitting recommendations when specific instruments for measuring the ocular sagittal heights are unavailable. According to this, sagittal heights of 4600 µm or higher would be needed for the trial lens when fitting the SCL evaluated in advanced KC.
Corneal tomographic changes
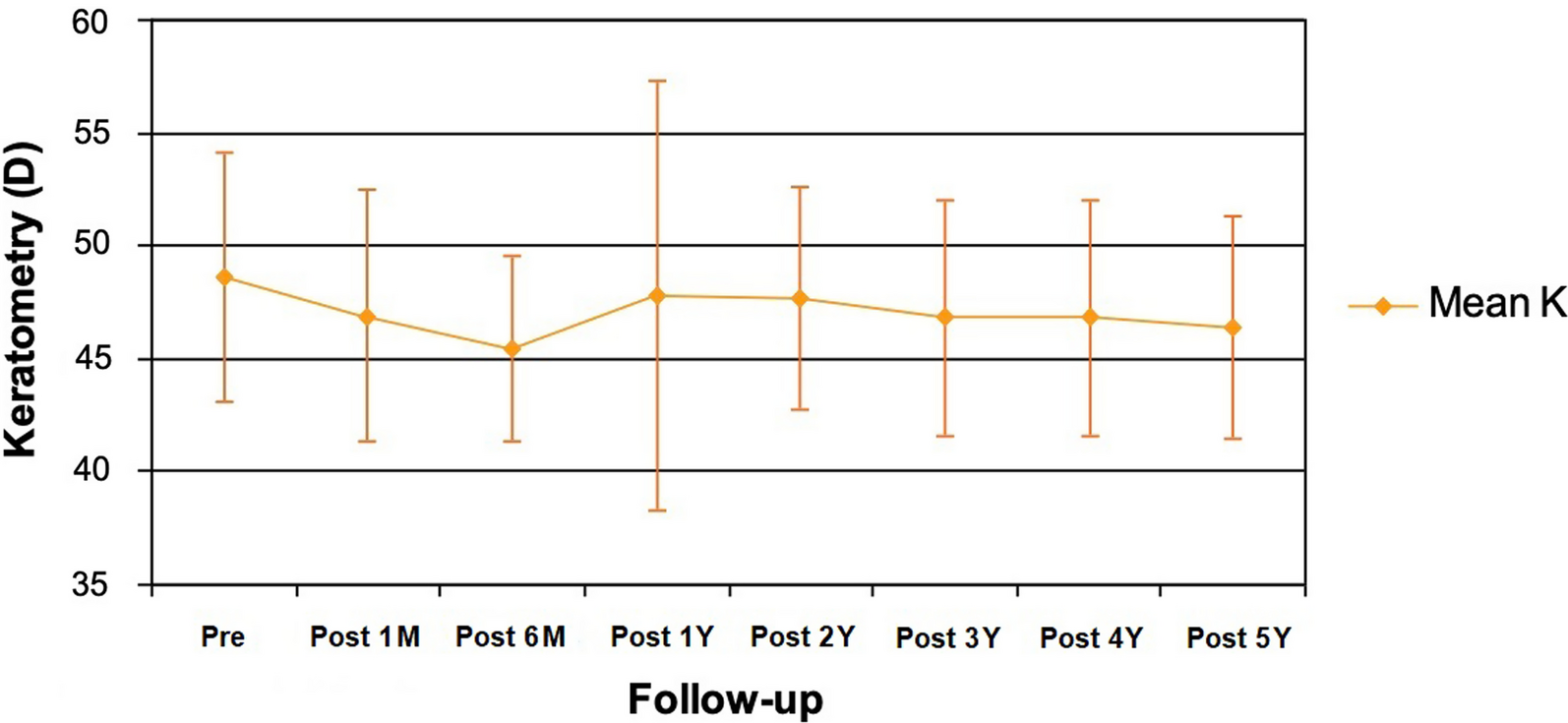
Concerning the evaluation of corneal tomographic changes, these did not reach statistical significance. This finding is in contrary to other studies that have reported significant changes in corneal shape and thickness in the short term [23, 24]. Serramito et al. [24] showed that there was a statistically significant corneal thinning in the inferior region of KC eyes fitted also with the ICD16.50 SCL and in the superior region of KC eyes implanted with intracorneal ring segments. A downward trend in MCT and CCT was observed in our series, but both did not reach statistical significance. Vincent et al. [40] reported a small and statistically significant amount of edema after 8 h of use of the ICD16.50 SCL in healthy adults. Specifically, a mean increase of 10.23 ± 5.77 μm in corneal thickness was observed which corresponded to 2% edema [40]. In another study, these same authors investigated the variation of edema over time, observing that the corneal thickness swelled after 15 min of CL use, stabilizing 45 min after CL insertion, reaching its maximum point after 90 min with a 1.18 ± 0.20% of edema, and gradually thinning after 2 h of use [41]. Possibly, in our sample, changes in corneal thickness associated to the initial use of the lens had been already stabilized when they were evaluated after 1 and 3 months of CL use. Similarly, minimal and no significant changes in anterior and posterior corneal shape and aberrations (6-mm pupil) were found, confirming the stability of the cornea with the use of the SCL during the first three months. Serramito et al. [23, 24] only found significant changes in anterior and posterior spherical aberrations after 8 h of SCL use, although more HOAs changed significantly when intracorneal ring segments had been implanted. In any case, a high variability was observed in corneal tomographic changes in the sample evaluated in the current study, confirming that the impact of the SCL on the cornea may vary between KC individuals.
Prediction model of visual change with the SCL
Finally, a multiple linear regression equation was obtained to predict the final VA through a series of initial data. This equation proposes the prediction of the VA change with the SCL evaluated from three variables (pre-fitting spectacle CDVA, lens power, and lens sagittal height) that can be obtained in the pre-fitting and first trial visits. Therefore, more VA improvement can be expected when fitting this SCL in those eyes with worse pre-fitting VA and fitted with SCL with lower sagittal heights and optical power. According to this, the ideal candidate for optimizing the visual quality with this type of SCL would be an advanced KC eye requiring a moderate to high myopic correction using a moderate to low sagittal height of the lens. The combination of the aberrometric profile of a negative powered SCL with a low sagittal height potentially associated to a low central vault (lower optical contribution of the post-lens meniscus as it would be thinner) may be associated to a potentially better optical quality and consequently may explain the contribution of these two factors to the predicting equation. This should be investigated in future investigations analyzing the optical profile of these SCLs as well as the optical impact of the post-lens meniscus. This prediction model has been verified and fulfilled the requirements to ensure its validity. The equation was able to predict the VA of the patients in the sample with very good results where only 10.3% of cases in which the error would be greater than 0.1 logMAR.
Limitations
Our study had several limitations. First, the study conducted was retrospective in nature. Second, a larger sample size especially for the development of predicting models would be more useful. Therefore, the current version of this model should only be considered preliminary and could be refined including data from larger samples. Furthermore, the measurements of the meniscus with the OCT were done by a single person manually so biases may have been present.


留言 (0)