In normal patients, we typically observe a greater systolic arterial pressure (SAP) in peripheral arteries than in the aorta, while the mean arterial pressure (MAP) is the same in peripheral arteries and in the aorta.1 Nevertheless, after cardiopulmonary bypass (CPB), this relationship is completely altered, and the radial artery SAP becomes significantly lower compared with the central aortic pressure. Several other investigators from the USA,2,3 Chile,4 Australia,5 Israel,6 Belgium,7 and Canada8,9,10 have reported similar observations. Those observations have led several cardiac centres to abandon radial artery pressure monitoring in cardiac surgery or to combine radial monitoring with more central arterial access such as the brachial3 or the femoral artery.11 An alternative approach would be selective monitoring of central blood pressures if known risk factors for an attenuated radial blood pressure post-CPB were present in a particular patient. The question then becomes: what are these risk factors?
In this issue of the Journal, An Ran Oh et al.12 address this issue by reporting the largest cohort to date of cardiac surgical patients with simultaneous measurements of both peripheral and central blood pressure. They included 2,019 patients in whom values of the radial-to-femoral arterial pressure gradient (RFAPG) were documented in the 30-min period following CPB. Using electronic records, the authors observed that a significant RFAPG (defined as a difference of ≥ 25 mm Hg for SAP or ≥ 10 mm Hg for MAP, lasting ≥ five minutes) occurred in 34% of patients. This percentage is identical to that of a study in 2018 that included 435 patients9 and very similar to the 35% reported recently by Bouchard-Deschene et al.10 Nevertheless, in these latter two studies, the RFAPG was measured from the beginning to the end of cardiac surgery. Since these abnormal RFAPG occur in one third of patients, can we predict who will develop such gradients?
In the study by An Ran Oh et al.,12 predictors of an RFAPG were age, body surface area, aortic cross-clamp time, and intraoperative epinephrine use. Several of those risk factors were also reported in previous studies. Nakayama et al.13 reported in 34 patients that higher RFAPGs were associated with longer CPB time and norepinephrine concentration. Abnormal RFAPGs were also reported in critically ill patients with high doses of norepinephrine.14 Nevertheless, some studies did not report such an association with vasoactive agents7 as an independent risk factor.9 Other investigators have also reported that small patients are predisposed to developing an RFAPG.8,9 This could be related to a smaller radial artery.8,15 Indeed, a radial artery diameter of less than 1.8 mm has been associated with 48% risk of an RFAPG.10 Those gradients have been reported not only in cardiac surgery but also in cardiac arrest,16 septic shock,14,17,18 liver transplantation,19,20,21 critically ill patients,22,23 and severe vasodilator intoxications.24 How can we explain these gradients?
Inaccurate arterial pressure values may be secondary to positioning the catheter tip against the vascular wall, partial canula occlusion or kinking, external compression, miscalibration, or subclavian stenosis.25 Pathophysiologically, there have been two major mechanisms proposed to explain the RFAPG observed in cardiac surgery: first, excess vasodilation in the peripheral vascular bed and second, arterial vasoconstriction or physical obstruction of medium-sized arteries8,9,13 (Figure, Panel A).
During and after CPB, vasoplegic syndrome is thought to be largely the result of a severe inflammatory response.26 Many factors and pathways are involved including extrinsic and intrinsic coagulation pathways, contact system activation, complement system activation, and cytokine release with endothelial cell activation and vasoactive substance release, including nitric oxide and prostacyclin.27 Arguments supporting this hypothesis are that risk factors for vasoplegia are similar to those associated with the RFAPG. Indeed, patients developing an RFAPG not only received more vasoactive agents such as epinephrine in the current study but also had a longer hospital stay.9 To support the second mechanism, Pauca et al.2,28 managed to restore arterial pressure by compressing the radial artery beyond the catheter insertion in patients with a significant RFAPG. Nevertheless, this technique did not modify the radial arterial pressure of patients without a gradient. They hypothesized that excess vasodilatation in the hand is partly responsible for a local drop of vascular resistance explaining the reduction in arterial pressure at the radial site. Maruyama also observed an increased RFAPG in cardiac surgical patients exposed to vasodilators29 and significant RFAPGs have been reported in vasodilator overdose.24
The second potential mechanism is excess proximal vasoconstriction. Under normal conditions, the resistive effects of medium-sized arteries are very low and the MAP all along medium-sized arteries is essentially equal. In a context of a significant gradient, it has been hypothesized that an excess of norepinephrine may exert a vasoconstrictive effect on the brachial artery. Kanazawa et al.30 studied different sites of measurement along the radial, brachial, and subclavian arteries. They found a strong correlation between the distance from the aorta to the site of measurement and the pressure drop from the aorta to the site of measurement.30 The reduction in diameter of the radial artery in patients in proportion to the severity of the RFAPG is another point that supports the idea of excess vasoconstriction in medium-diameter arteries.15
If the radial artery is not reliable, are there any risks of using the femoral artery? The safety of using the femoral artery has been reported by other authors.11,31,32,33 An Ran Oh et al.12 also examined carefully the safety of using a femoral artery catheter. Interestingly they used a very small 20G, 8-cm catheter, basically the same size as a typical adult radial artery catheter. They were able to document a comparable safety profile to that of radial catheters but did not specify whether ultrasound guidance was used for insertion.
There are still unanswered questions. For instance, what are the consequences of just using a radial artery catheter in cardiac surgery (which is still commonly done in many centres). One observational study has explored this issue and showed a reduced use of vasoactive agents in patients monitored using both radial and femoral artery catheters.10 Is the femoral artery always more accurate than the radial artery? What about pediatric patients with very small radial arteries? The presence of a significant gradient has been reported in cardiac surgery34 with the same risk factors as in adults.35 Is it safe in this population? Is the brachial artery a reliable alternative? Brachial and femoral artery pressure monitoring have been compared in terms of reliability in only one study and the brachial artery was found to be less reliable.5 Finally, if we are still using a radial site for arterial pressure monitoring, when should we suspect a falsely low radial artery pressure reading?
In addition to the identification of risk factors, there are several methods that can be used at the bedside when there is a doubt about the reliability of a radial arterial pressure. In cardiac surgery during open chest conditions, if significant vasoactive support is present, inserting a subcutaneous needle in the aorta connected to a pressure transducer is a rapid way to directly assess aortic pressure. Alternatively, if the aortic cannula is still in place but not being used, it can be transduced directly to obtain a reflected aortic pressure. If a significant RFAPG between the aortic and radial artery pressures is present, the clinician can insert a femoral artery catheter at that point to continuously assess central arterial pressure.
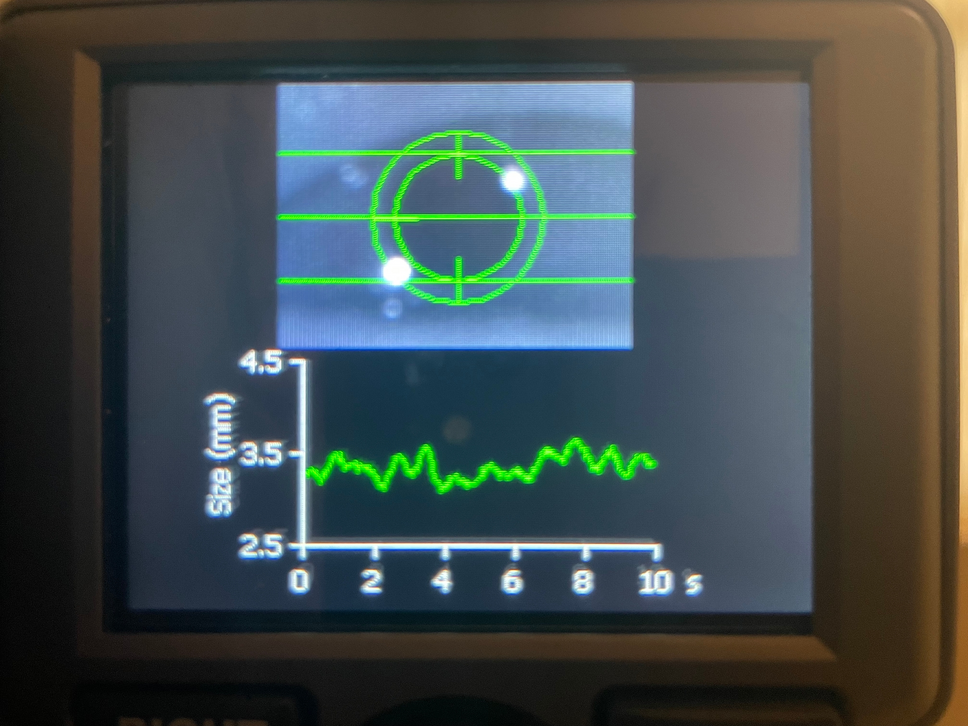
Bedside ultrasound can potentially be used to anticipate the risk of an RFAPG (Figure, Panel B). For instance, if the radial artery diameter is < 1.8 mm10 or if an abnormal (i.e., nontriphasic) radial or brachial arterial Doppler signal is present,36 then other arterial sites should likely be used. Doppler interrogation of the femoral artery should also be considered before using the femoral site, particularly in patients with vascular disease. If a patient has mitral regurgitation (MR), the peak systolic gradient should not exceed the radial arterial pressure18 in the absence of valvular, subvalvular, or peripheral stenosis. In addition, the MR change in pressure over time (dP/dt) should be similar to the arterial dP/dt. It is important to analyze the arterial pressure waveform. In the presence of an RFAPG, pulsus tardus is often present in a patient with a normal left ventricle and no aortic stenosis. With an RFAPG, the radial dP/dt is typically lower than the femoral value6,13,16 and also lower than the estimated dP/dt based on the MR Doppler signal if available.18
Noninvasive measurement of blood pressure in the upper extremity using a blood pressure cuff can also be used to detect such gradients. In the intensive care unit, Jacquet-Lagrèze et al.23 were able to identify significant RFAPG with a specificity of 92% (95% confidence interval [CI], 67 to 100) and a sensitivity of 100% (95% CI, 83 to 100). A simple method to potentially confirm an RFAPG is to compress the radial artery or the wrist distal to the point of insertion of the catheter.28,37 This excludes the vasodilated territory of the hand and enables evaluation of aortic arterial pressure. Nevertheless, the accuracy of this proposed test has not been systematically evaluated in large populations. Finally, an RFAPG leading to pseudo-radial artery hypotension should be suspected in the presence of normal direct measurement or estimation of cardiac output, or evidence of adequate tissue perfusion using, for instance, capnography or near-infrared spectroscopy values.38
In summary, the underestimation of arterial pressure by radial measurement in cardiac surgery and potentially in other types of surgery19,20,21,39,40,41 and in the intensive care unit14,17,18,24 could lead to inappropriate therapeutic interventions and excessive doses of vasopressors or fluids.10,18,24 There are risk factors for an elevated RFAPG, but our ability in terms of prediction remains somewhat limited. Since the hazard of inaccurate monitoring is to give too much vasopressors or fluids because of a systematic underestimation of arterial pressure, a pragmatic approach could be to insert a femoral catheter when high doses of norepinephrine or fluid seem likely to be necessary to maintain the arterial pressure. In that case, the beneficial effect will be greater than in a patient who does not need vasopressors or fluids during the intra- and postoperative periods. Nonetheless, the risk of femoral artery catheterization using a 20G 8-cm catheter reported by An Ran Oh et al.12 was negligible; it was similar to or lower than that reported for radial artery catheterization. Furthermore, unnecessary excessive vasopressor administration is hazardous and potentially detrimental to patients. Therefore, based on the evidence presented, the routine use of a more central site than the radial artery should be considered for arterial pressure monitoring in cardiac surgery. Some current literature suggests the superiority of the femoral site over the brachial artery; however, more studies are required to confirm this finding.
Chez les patients normaux, nous observons habituellement une pression artérielle systolique (PAS) plus élevée dans les artères périphériques que dans l'aorte, tandis que la pression artérielle moyenne (PAM) est la même dans les artères périphériques et dans l'aorte.1 Toutefois, cette relation est totalement modifiée après une circulation extracorporelle (CEC) et la PAS de l'artère radiale devient significativement inférieure à la pression aortique centrale. Plusieurs autres investigateurs, aux États-Unis,2,3 au Chili,4 en Australie,5 en Israël,6 en Belgique7 et au Canada8,9,10 ont publié des observations comparables. Ces observations ont conduit plusieurs centres hospitaliers à substituer la surveillance de la pression de l'artère radiale en chirurgie cardiaque par un site différent ou à combiner simultanément la mesure de la pression radiale avec un accès artériel plus central, comme l'artère brachiale3 ou l'artère fémorale.11 Une approche possible serait de suivre de manière sélective les pressions artérielles centrales si des facteurs de risque connus d'atténuation de la PA radiale après CEC étaient présents chez un patient donné. La question qui se pose est alors quels sont ces facteurs de risque?

留言 (0)