
記住我








Although pathophysiological mechanisms underlying the hypertension-depression link are complex and still not fully understood, there has been strong and clear evidence on the elevated risk of depressive symptoms and disorders in hypertensive patients (1–4). For example, in China the prevalence rates of depressive symptoms and DSM-IV depressive disorders among outpatients with essential hypertension in large tertiary general hospitals are 47.6 and 16.6%, which are three and ten times as high as those in the general Chinese population, respectively (5, 6). The co-occurring depression has been associated with prolonged duration of hypertension, poor compliance with antihypertensive agents, and failure of adherence to lifestyle interventions, which in turn, complicates the management of hypertension and increases risk of cardiovascular complications (7–9). In this context, expanding our knowledge on the etiology and mechanisms of depression in hypertensive patients is clinically relevant, which may facilitate the effective management of hypertension and the prevention of hypertension-related complications.
The cause of depression in the general population is multifactorial in nature, which involves biological, psychological, and social factors and their interplays (10–12) and, accordingly, the cause of depression in hypertensive patients is no exception. In the literature, a range of factors associated with depression in hypertensive patients have been reported by many clinical studies in China and many other countries, including female sex, advanced age, a low level of educational attainment, marital status of divorced and widowed, low income, living alone, smoking, alcohol consumption, inadequate social support, a long duration of hypertension, and coexistence of major medical conditions (5, 6, 13–20). Nevertheless, nearly all the available studies focused on the main effects of these factors but none paid attention to how the factors work together to determine the depression risk, which may reveal the mechanisms of the mutual cross-talk between factors and how the combination of factors influences the risk of depression, and, in turn, inform the planning of mental health services. For example, if the influence of living alone on depression is conditional on the sex of an individual: statistically significant association of living alone with depression is evident only in women, providing mental health services to women who were living alone would be more cost-effective. In addition, a further limitation of the prior studies is no findings on the relative contributions of the identified factors to the risk of depression, because the statistical method adopted by previous studies, multiple logistic regression model, is often used to identify statistically significant correlates of depression, not clinically important correlates (21).
Because of the higher prevalence of hypertension in older adults than middle-aged and younger adults, older adults with hypertension are the main target population of interest of many previous studies examining depression in hypertension (13–15, 19, 20). These studies used a variety of self-rating scales of depressive symptoms (i.e., nine-item Patient Health Questionnaire and Zung’s Self-rating Depression Scale) and reported a wide range of prevalence rates of depressive symptoms (12.8–61.0%) in hypertensive older adults (14, 19). However, because of no rigorous psychiatric interviews, the proportion of hypertensive older adults whose depressive symptoms are severe enough to meet the clinical diagnostic criteria of depressive disorders remains unknown (22).
To advance the literature in this area, this study was set out to investigate the prevalence of depressive disorders in older Chinese adults with hypertension, and, adopted classification tree analysis (CTA) to examine the major correlates of depressive disorders and identify the interaction between correlates. Unlike traditional binary logistic regression, CTA is a robust algorithm to identify clinically important factors associated with the outcome of interest and effectively detect factor interactions (23). Furthermore, another strength of CTA is its user-friendly way to show findings on factors associated with the outcome and their interactions, which can be easily applied to routine clinical and primary care practice by healthcare workers with limited statistical understanding (24).
Materials and methods SampleThe study sample was 374 hypertensive older adults from a large-scale multi-center cross-sectional survey that examined mental health and quality of life among a representative sample of older adults receiving primary care in seven urban and six rural primary care centers in Wuhan, China, between October 2015 and November 2016. Older primary care patients who were 65 years or older, voluntary to join the study, and diagnosed with essential hypertension or taking antihypertensive medications were included in the current analysis. Details of the sampling and the recruitment of respondents have been published elsewhere (25–29).
The Ethics Committee of Wuhan Mental Health Center approved the study proposal before the formal survey (approval number WMHC-IRB-S065). All respondents and their guardians (when necessary) provided written informed consent form before the interview.
Instruments and proceduresThe study instrument was a questionnaire, which was administered in a face-to-face format by trained primary care physicians (PCPs). The validated Chinese version of the Mini-international Neuropsychiatric Interview (MINI) 5.0 was used to assess the presence of DSM-IV depressive disorders within the past month, including major depressive disorder, dysthymic disorder, and minor depressive disorder (30).
The demographic variables in the questionnaire were sex, age, education, marital status, self-rated financial status, and residence place. Social factors included living arrangement (alone or not alone), self-rated relationship with family members (good, fair, poor), and self-rated relationship with non-family associates (good, fair, poor). Lifestyle factor was currently smoking, which was defined as smoking 5 days per week or more within the last month (27). Psychological factor was feelings of loneliness, which was assessed with a single-item question: “How often do you feel lonely?” with five answer options: always, often, sometimes, seldom, and never. Participants who felt lonely “sometimes,” “often,” and “always” were those having feelings of loneliness (28). Clinical factors were the comorbid major medical conditions, which was assessed with a checklist and included diabetes mellitus, heart disease, cerebrovascular disease, chronic obstructive pulmonary disease, chronic gastric ulcer, and arthritis.
Statistical analysisIBM SPSS statistics software, version 24 (SPSS Inc., Chicago, IL, USA) was used to perform all the analyses. Two-sided P < 0.05 was statistically significant. Prevalence rates of depressive disorders and their three subtypes were calculated. By using Chi-square test, we compared the characteristics between respondents with and without depressive disorders to characterize respondents with depressive disorders.
To identify major correlates of depressive disorders and their potential interactions, the exhaustive Chi-squared automatic interaction detection (exhaustive CHAID) growing approach was used to perform the CTA. The target category of the outcome in the CTA was the presence of depressive disorders, and all demographic, social, lifestyle, psychological, and clinical variables were included as input variables. We set the maximum number of layers of growth beneath the root node at three and the minimum node sizes at 50 for parent nodes and 25 for child nodes. The CTA divided the study sample into branch-like segments by comparing Chi-square statistics of all possible categories in relation to depressive disorders and this process continued recursively until the tree was fully grown. These segments consisted of an inverted tree with a root node, internal nodes, and end nodes. Accordingly, the classification tree automatically identified correlates of depressive disorders from the root nodes to endnotes, in the order of importance, as well as the interactions between these correlates (23, 31).
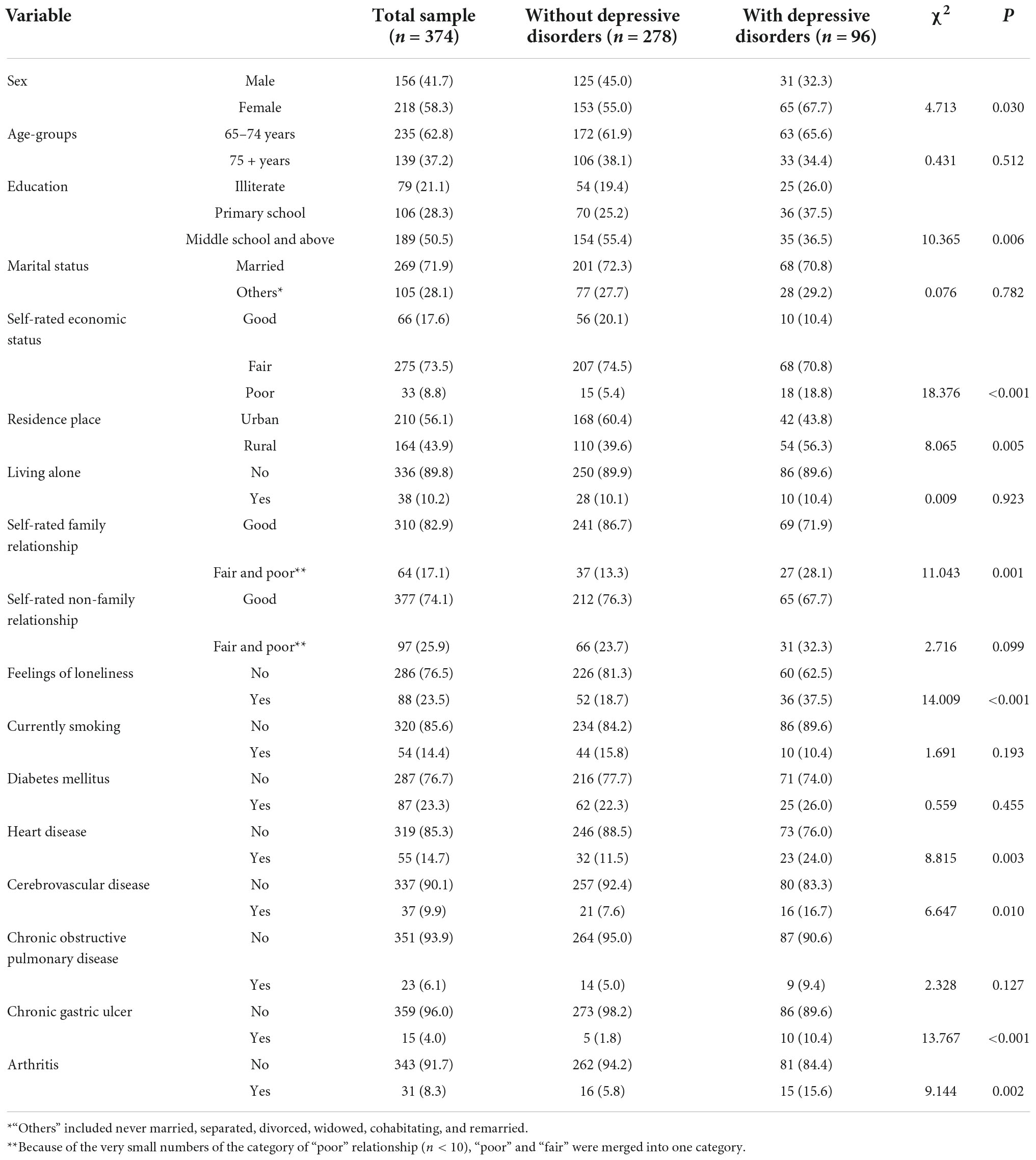
ResultsThe average age of the 374 hypertensive older adults was 72.9 years (standard deviation [SD]: 5.8, range: 65–93) and 41.7% were men. Table 1 shows the characteristics of the whole sample and respondents with and without depressive disorders.
TABLE 1
Table 1. Characteristics of hypertensive older Chinese adults, split by the presence and absence of depressive disorders, n (%).
The 1-month prevalence rate of depressive disorders was 25.7%. The corresponding rates for major depressive disorder, dysthymic disorder, and minor depressive disorder were 13.6, 6.1, and 5.9%, respectively.
As displayed in Table 1, compared to respondents without depressive disorders, depressed respondents were more likely to be women, have an educational attainment of illiterate and primary school, rate their economic status as “poor,” dwell in rural areas, rate their relationship with family members as “fair and poor,” feel lonely, suffer from heart disease, suffer from cerebrovascular disease, suffer from chronic gastric ulcer, and suffer from arthritis (P ≤ 0.030).
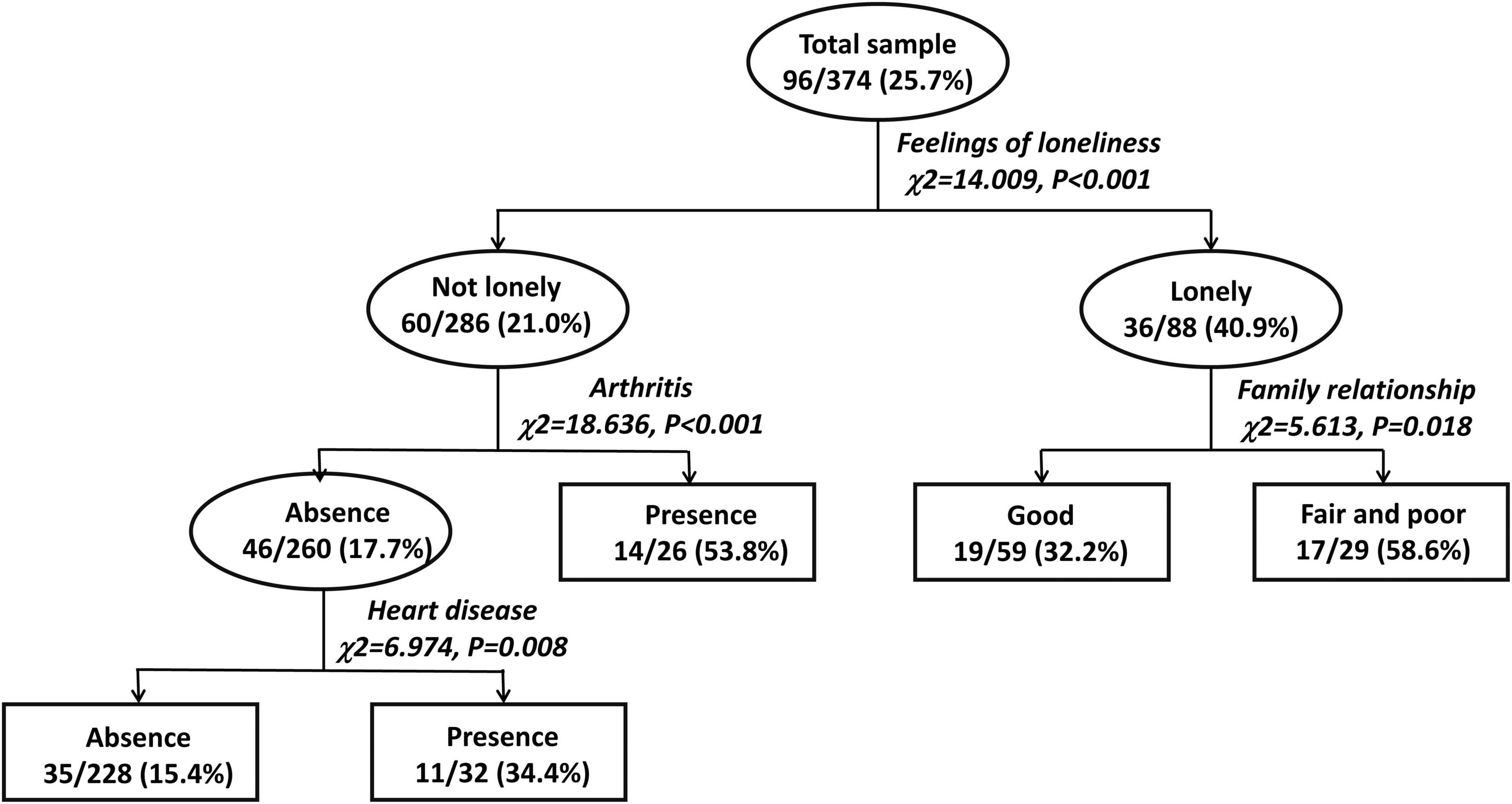
As shown in Figure 1, the CTA model had three layers of eight nodes, including five end nodes. Four major correlates of depressive disorders were identified: loneliness was the most salient, followed by arthritis, family relationship, and heart disease. Compared to respondents who were not lonely, lonely respondents were 1.9-fold more likely to have depressive disorders (40.9 vs. 21.0%, P < 0.001). Among the lonely respondents, relative to those who had good family relationship, those having fair and poor relationship were 1.8-fold more likely to have depressive disorders (58.6 vs. 32.2%, P = 0.018). Among respondents who were not lonely, relative to those having no arthritis, those having arthritis were 3.0-fold more likely to have depressive disorders (53.8 vs. 17.7%, P < 0.001). Among respondents who were not lonely and did not suffer from arthritis, relative to those having no heart disease, those having heart disease were 2.2-fold more likely to have depressive disorders (34.4 vs. 15.4%, P = 0.008). There were statistically significant interactions between loneliness and arthritis, loneliness and family relationship, and arthritis and heart disease.
FIGURE 1
Figure 1. Classification tree analysis for major correlates of depressive disorders and the interactions of factors in older Chinese adults with hypertension.
DiscussionIn China, both hypertension and depressive disorders occur predominantly in the elderly population, and the comorbidity of depression further significantly contributes to the vulnerability of the elderly to hypertension (32). In the context of rapid aging in China, disentangling the complex relationship between factors associated with depression in hypertension may help illuminate the pathways involved in the pathogenesis of the comorbidity of depression, potentially leading the way for effective management of hypertension and effective public health interventions to reduce the disease burden of hypertension (33–37). The present study fills the knowledge gaps by providing empirical data on the prevalence rates of depressive disorders and their subtypes in the elderly population with hypertension and demonstrating major factors associated with depressive disorders and the interactions between these factors. To the best of our knowledge, this is the first study in China examining depressive disorders and testing the interplays between factors associated with depression in older adults with hypertension.
The main findings of this study are the 25.7% prevalence of depressive disorders in hypertensive older adults with major depressive disorder being the most common, four major correlates of depressive disorders with loneliness being the most prominent, and the significant interactions between loneliness and arthritis, loneliness and family relationship, and arthritis and heart disease.
In community-residing older Chinese adults, the 1-month prevalence rates of depressive disorders, major depressive disorder, dysthymic disorder, and mood disorder not otherwise specified (minor depressive disorder is a subtype of this category) were 5.5, 3.8–5.9, 3.9, and 3.0%, respectively (38–40). In older Chinese adults seeking treatment in primary care settings, the 1-month prevalence rates of depressive disorders, major depressive disorder, dysthymic disorder, and minor depressive disorder were 20.3, 10.2–11.3, 4.8, and 5.3%, respectively (26, 41). Therefore, in comparison to these prevalence estimates in older Chinese adults in both community and primary care settings, we found the higher risk of depressive disorders and their subtypes in Chinese patients with hypertension. In the literature, possible explanations for how hypertension results in or exacerbates depression include the mental health burden of suffering from hypertension and its negative impact on a person’s quality of life, a low sense of self-worth, low self-esteem, and a loss of locus of control due to the negative psychological effect of hypertension, and structural changes in brain areas related to emotion as a result of pathophysiologic effects of hypertension on central nervous system (42).
Our findings on possible factors associated with depressive disorders in hypertensive older adults (Table 1) are largely consistent with those from previous studies (5, 6, 13–20). Nevertheless, only four of these factors were finally identified as major correlates of depression in the CTA, suggesting the considerable contributions of loneliness, arthritis, fair and poor family relationship, and heart disease to the elevated risk of depression.
Evidence from longitudinal studies has confirmed the vicious circle between loneliness and depression, that is, loneliness triggers depressive emotions, which create feelings of isolation and alienation and, in turn, result in loneliness (43–45). Accordingly, we replicated the significant loneliness-depression association in hypertensive older adults. In a population-based study of middle-aged adults, Dunlop and colleagues found that both arthritis and heart disease were significantly associated with major depression and the functional limitation caused by the two chronic illnesses can explain their associations with major depression (46). Similar to this study, we also found the significant association of depression with arthritis and heart disease in hypertensive older adults. We also speculate the functional limitation associated with the two major medical conditions might be the primary cause of depressive disorders. Unlike older adults in western countries, family harmony and intergenerational relationship play a pivotal role in the mental well-being of older Chinese adults due to the influence of Confucian culture (47, 48). In accordance with this perspective, fair and poor family relationship was significantly associated with depression in hypertensive older adults.
The three significant interactions between the four major correlates suggest that the factor per se not only directly contributes to the risk of depression but also magnifies the negative effects of other factors on the risk of depression. The four factors work together may substantially increase the risk of depression in hypertensive older adults.
This study has several limitations. First, this is a cross-sectional study, so longitudinal studies are warranted to further ascertain the causal relationships between the four identified major correlates and depressive disorders. Second, our CTA is exploratory without evidence of external validity. More studies are needed to validate the findings in other cohorts of older adults with hypertension. Third, the sample size of this study is relatively small. Further, the sample of hypertensive older adults was recruited from primary care settings in Wuhan China. Hypertensive older adults from large general hospitals and other cities in China were not included. Therefore, there might be selection bias in our study sample. Fourth, other factors potentially associated with depression in hypertensive older adults such as personality, physical pain, blood pressure control status, stage of hypertension, and type of antihypertensive drugs were not measured.
In summary, over one out of every four older Chinese adults with hypertension suffer from depressive disorders, suggesting the high risk of depressive disorders in hypertensive older adults. Considering many negative outcomes associated with depression, mental health services for this patient population are urgently needed, which should include psychosocial support, periodic screening for depressive symptoms to ensure early recognition of older adults with depressive disorders, and early initiation of antidepressant treatment when necessary. Our findings on the four major correlates of depressive disorders are clinically interesting because feelings of loneliness, family relationship, arthritis, and heart disease are all potentially modifiable or treatable. The significant interplays between the four major factors further indicate the clinical needs for collaborative multidisciplinary management services for reducing the burden of depression in hypertension, which integrate social work outreach services to promote family relationship, mental health services to relive loneliness, and primary care services to manage arthritis and heart disease.
Data availability statementThe original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving human participants were reviewed and approved by the Ethics Committee of Wuhan Mental Health Center. The patients/participants provided their written informed consent to participate in this study.
Author contributionsJR: acquisition and analysis of data for the study, drafting the manuscript, and interpretation of data for the study. JR and Y-MX: design and acquisition of data for the study. B-LZ: drafting the manuscript, revising the manuscript for important intellectual content, and interpretation of data for the study. All authors contributed to the article and approved the submitted version.
FundingThis work was supported by the National Natural Science Foundation of China (grant number: 71774060), 2015 Irma and Paul Milstein Program for Senior Health Awards from the Milstein Medical Asian American Partnership Foundation, the Young Top Talent Programme in Public Health from Health Commission of Hubei Province (PI: B-LZ), and Wuhan Health and Family Planning Commission (grant numbers: WX17Q30, WG16A02, and WG14C24). The funding source listed had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
AcknowledgmentsWe thank all the research staff for their team collaboration work and all the older adults and primary healthcare physicians involved in this study for their cooperation and support.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Endomba FT, Mazou TN, Bigna JJ. Epidemiology of depressive disorders in people living with hypertension in Africa: a systematic review and meta-analysis. BMJ Open. (2020) 10:e037975. doi: 10.1136/bmjopen-2020-037975
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Li Z, Li Y, Chen L, Chen P, Hu Y. Prevalence of depression in patients with hypertension: a systematic review and meta-analysis. Medicine (Baltimore). (2015) 94:e1317. doi: 10.1097/MD.0000000000001317
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Meng L, Chen D, Yang Y, Zheng Y, Hui R. Depression increases the risk of hypertension incidence: a meta-analysis of prospective cohort studies. J Hypertens. (2012) 30:842–51. doi: 10.1097/HJH.0b013e32835080b7
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Zong L, Shi H, JIng J, Zhang X. Study on prevalence and correlates of depressive symptoms among patients with essential hypertension from 4 tertiary general hospitals in Guangzhou City and Ningbo City. Med Soc. (2016) 29:71–4. doi: 10.13723/j.yxysh.2016.01.023
CrossRef Full Text | Google Scholar
6. Zhang X, Fan Q, Fang Q, Jing J, Zong L. Current prevalence and correlates of depressive disorder among outpatients with essential hypertension from cardiovascular divisions of tertiary general hospitals. Chin J Nerv Ment Dis. (2015) 28:193–8, 223. doi: 10.3936/j.issn.1002-0152.2015.04.001
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Krousel-Wood MA, Frohlich ED. Hypertension and depression: coexisting barriers to medication adherence. J Clin Hypertens (Greenwich). (2010) 12:481–6. doi: 10.1111/j.1751-7176.2010.00302.x
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Maier A, Riedel-Heller SG, Pabst A, Luppa M. Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS One. (2021) 16:e0251326. doi: 10.1371/journal.pone.0251326
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Ma C. The prevalence of depressive symptoms and associated factors in countryside-dwelling older Chinese patients with hypertension. J Clin Nurs. (2018) 27:2933–41. doi: 10.1111/jocn.14349
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Xue J, Chen S, Bogner HR, Tang W, Li L, Conwell Y. The prevalence of depressive symptoms among older patients with hypertension in rural China. Int J Geriatr Psychiatry. (2017) 32:1411–7. doi: 10.1002/gps.4628
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Ma L, Tang Z, Sun F, Diao L, Li Y, Wang J, et al. Risk factors for depression among elderly subjects with hypertension living at home in China. Int J Clin Exp Med. (2015) 8:2923–8.
PubMed Abstract | Google Scholar
16. Asmare Y, Ali A, Belachew A. Magnitude and associated factors of depression among people with hypertension in Addis Ababa, Ethiopia: a hospital based cross-sectional study. BMC Psychiatry. (2022) 22:327. doi: 10.1186/s12888-022-03972-6
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Ji K, Bai Z, Tang L, Yan H, Zhu Y, Chen G, et al. Institutional satisfaction and anxiety mediate the relationship between social support and depression in hypertension patients in elderly caring social organizations: a cross-sectional study. Front Psychol. (2021) 12:772092. doi: 10.3389/fpsyg.2021.772092
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Yang Y, Cui L, Zhang Y, Li J, Sun X, Yan B, et al. Sleep quality of hypertensive patients with comorbid depression and its influence factors. J Pract Med. (2021) 37:2053–7, 64. doi: 10.3969/j.issn.1006-5725.2021.16.004
CrossRef Full Text | Google Scholar
19. Du W, Zheng Y, Yuan Y. Investigation and analysis of depressive factors in elderly hy-pertensive patients in Guancheng District, Dongguan City. J Clin Psychosomatic Dis. (2020) 26:127–9. doi: 10.3969/j.issn.1672-187X.2020.06.029
CrossRef Full Text | Google Scholar
20. Dong L, Ma X, Wang R, Zhang Y, Zhou Y. Quality of life and its association in elderly patients with hypertension and depression in Beijing community. J Cardiovasc Pulmonary Dis. (2020) 39:410–6. doi: 10.3969/j.issn.1007-5062.2020.04.012
CrossRef Full Text | Google Scholar
21. Ranganathan P, Pramesh CS, Aggarwal R. Common pitfalls in statistical analysis: logistic regression. Perspect Clin Res. (2017) 8:148–51. doi: 10.4103/picr.PICR_87_17
CrossRef Full Text | Google Scholar
22. Zhong BL, Xu YM, Li Y. Prevalence and unmet need for mental healthcare of major depressive disorder in community-dwelling Chinese people living with vision disability. Front Public Health. (2022) 10:900425. doi: 10.3389/fpubh.2022.900425
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Camp NJ, Slattery ML. Classification tree analysis: a statistical tool to investigate risk factor interactions with an example for colon cancer (United States). Cancer Causes Control. (2002) 13:813–23. doi: 10.1023/a:1020611416907
CrossRef Full Text | Google Scholar
24. Xu YM, Li C, Zhu R, Zhong BL. Prevalence and correlates of insomnia symptoms in older Chinese adults during the COVID-19 outbreak: a classification tree analysis. J Geriatr Psychiatry Neurol. (2022) 35:223–8. doi: 10.1177/08919887221078561
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Zhong BL, Xu YM, Xie WX, Liu XJ. Quality of life of older Chinese adults receiving primary care in Wuhan, China: a multi-center study. PeerJ. (2019) 7:e6860. doi: 10.7717/peerj.6860
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Zhong BL, Ruan YF, Xu YM, Chen WC, Liu LF. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: a multi-center cross-sectional study. J Affect Disord. (2020) 260:26–31. doi: 10.1016/j.jad.2019.09.011
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Zhong BL, Xu YM, Xie WX, Liu XJ, Huang ZW. Depressive symptoms in elderly Chinese primary care patients: prevalence and sociodemographic and clinical correlates. J Geriatr Psych Neur. (2019) 32:312–8. doi: 10.1177/0891988719862620
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Zhong BL, Liu XJ, Chen WC, Chiu HF, Conwell Y. Loneliness in Chinese older adults in primary care: prevalence and correlates. Psychogeriatrics. (2018) 18:334–42. doi: 10.1111/psyg.12325
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Zhu XM, Xu YM, Wang ZQ, Zhong BL. Prevalence and correlates of suicidal ideation among older adults attending primary care clinics in Wuhan, China: a multicenter cross-sectional study. Front Psychiatry. (2022) 13:1003810. doi: 10.3389/fpsyt.2022.1003810
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Si T, Shu L, Dang W, Su Y, Chen J, Dong W, et al. Evaluation of the reliability and validity of Chinese version of the Mini-International Neuropsychiatric Interview in patients with mental disorders. Chin Ment Health J. (2009) 23:493–7. doi: 10.3969/j.issn.1000-6729.2009.07.011
CrossRef Full Text | Google Scholar
32. Turana Y, Tengkawan J, Chia YC, Shin J, Chen CH, Park S, et al. Mental health problems and hypertension in the elderly: review from the HOPE Asia Network. J Clin Hypertens (Greenwich). (2021) 23:504–12. doi: 10.1111/jch.14121
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Zhong BL, Chen SL, Tu X, Conwell Y. Loneliness and cognitive function in older adults: findings from the chinese longitudinal healthy longevity survey. J Gerontol B Psychol Sci Soc Sci. (2017) 72:120–8. doi: 10.1093/geronb/gbw037
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Zhong BL, Xiang YT. Challenges to and recent research on the mental health of older adults in China during the COVID-19 pandemic. J Geriatr Psychiatry Neurol. (2022) 35:179–81. doi: 10.1177/08919887221078558
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Chen WC, Chen SJ, Zhong BL. Sense of alienation and its associations with depressive symptoms and poor sleep quality in older adults who experienced the lockdown in Wuhan, China, during the COVID-19 pandemic. J Geriatr Psychiatry Neurol. (2022) 35:215–22. doi: 10.1177/08919887221078564
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Hua R, Ma Y, Li C, Zhong B, Xie W. Low levels of low-density lipoprotein cholesterol and cognitive decline. Sci Bull. (2021) 66:1684–90. doi: 10.1016/j.scib.2021.02.018
CrossRef Full Text | Google Scholar
37. Li C, Zhu Y, Ma Y, Hua R, Zhong B, Xie W. Association of cumulative blood pressure with cognitive decline, dementia, and mortality. J Am Coll Cardiol. (2022) 79:1321–35. doi: 10.1016/j.jacc.2022.01.045
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Ye M, Zhong S, Lin C, Ye S, Chen C. Prevalence, influencing factors and help-seeking style of depression among elderly population in Wenzhou area. Chin J Public Health. (2013) 29:8–11. doi: 10.11847/zgggws2013-29-01-03
CrossRef Full Text | Google Scholar
39. Liu XJ, Zhou Y, Dong L, Guo Q, Chen WC. A survey of major depression among elderly population in Wuhan. Chin Ment Health J. (2017) 31:851–6.
40. Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05: an epidemiological survey. Lancet. (2009) 373:2041–53. doi: 10.1016/S0140-6736(09)60660-7
CrossRef Full Text | Google Scholar
41. Chen S, Conwell Y, Vanorden K, Lu N, Fang Y, Ma Y, et al. Prevalence and natural course of late-life depression in China primary care: a population based study from an urban community. J Affect Disord. (2012) 141:86–93. doi: 10.1016/j.jad.2012.02.027
PubMed Abstract | CrossRef Full Text | Google Scholar
42. Herrera PA, Campos-Romero S, Szabo W, Martinez P, Guajardo V, Rojas G. Understanding the relationship between depression and chronic diseases such as diabetes and hypertension: a grounded theory study. Int J Environ Res Public Health. (2021) 18:12130. doi: 10.3390/ijerph182212130
PubMed Abstract | CrossRef Full Text | Google Scholar
43. Hsueh YC, Chen CY, Hsiao YC, Lin CC. A longitudinal, cross-lagged panel analysis of loneliness and depression among community-based older adults. J Elder Abuse Negl. (2019) 31:281–93. doi: 10.1080/08946566.2019.1660936
PubMed Abstract | CrossRef Full Text | Google Scholar
44. Cacioppo JT, Hawkley LC, Thisted RA. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychol Aging. (2010) 25:453–63. doi: 10.1037/a0017216
PubMed Abstract | CrossRef Full Text | Google Scholar
45. van Zutphen EM, Kok AAL, Rijnhart JJM, Rhebergen D, Huisman M, Beekman ATF. An examination of reciprocal effects between cardiovascular morbidity, depressive symptoms and loneliness over time in a longitudinal cohort of Dutch older adults. J Affect Disord. (2021) 288:122–8. doi: 10.1016/j.jad.2021.03.081
PubMed Abstract | CrossRef Full Text | Google Scholar
46. Dunlop DD, Lyons JS, Manheim LM, Song J, Chang RW. Arthritis and heart disease as risk factors for major depression: the role of functional limitation. Med Care. (2004) 42:502–11. doi: 10.1097/01.mlr.0000127997.51128.81
CrossRef Full Text | Google Scholar
47. Lam WW, Fielding R, McDowell I, Johnston J, Chan S, Leung GM, et al. Perspectives on family health, happiness and harmony (3H) among Hong Kong Chinese people: a qualitative study. Health Educ Res. (2012) 27:767–79. doi: 10.1093/her/cys087
PubMed Abstract | CrossRef Full Text | Google Scholar
48. Chan SS, Viswanath K, Au DW, Ma CM, Lam WW, Fielding R, et al. Hong Kong Chinese community leaders’ perspectives on family health, happiness and harmony: a qualitative study. Health Educ Res. (2011) 26:664–74. doi: 10.1093/her/cyr026
留言 (0)