
記住我








Coronavirus Disease 2019 (COVID-19) is a main pandemic infection that has hit the world with multiple waves (1). Its evolution through the years ahead remains uncertain (2), because of the emergence of new variants (3, 4), vaccination campaigns and innovative treatments (5).
Previous cardiovascular comorbidities seem to worsen the prognosis of the infection (6), but COVID-19 may cause several cardiovascular complications via different mechanisms (7). Systemic inflammation can destabilize vascular plaque, while viral illness increases cytokine activity, increasing cardiac demand, like influenza (8). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may also cause direct damage to the heart utilizing ACE2 receptors located within cardiac tissue (9). This infection is thereby associated with venous thromboembolic events (10–14), myocarditis (7, 15, 16), arrhythmias (14) and increased risk of acute myocardial infarction (17–20) and possible coronary tropism of the virus in thrombi (21, 22). All these complications may induce electrocardiographic abnormalities. Electrocardiogram (ECG) is a simple and broadly available exam which can be rapidly performed without exposing a large number of staff to the virus. Systematic standard ECG may be a useful screening tool for cardiovascular complications in patients presenting with COVID-19.
There are few published studies of ECG modifications related to COVID-19 (23–28). A retrospective cohort study of 756 patients comparing ECG abnormalities showed that both left- and right-sided heart disease in patients with COVID-19 have higher odds of death (26), but the confounding factors are not well-described.
A narrative review shows that up to 90% of critically ill patients have at least one ECG abnormality, including supraventricular tachycardia or ST modification, mainly related to cytokine storm, hypoxic injury, electrolyte abnormalities, plaque rupture, coronary spasm, microthrombi, or direct endothelial or myocardial injury (27). The objective of this study was to describe ECG abnormalities during COVID-19 and their impact on prognosis.
MethodsWe reviewed from our database all patients referred to our hospital for COVID-19 between January 1st, 2020 and December 31st, 2020. All the cases of COVID-19 were proved by SARS-CoV-2 RT-PCR on nasopharyngeal swabs. We included all hospitalized patients [including in intensive care unit (ICU)] with an available ECG. Patients with ventricular pacing were excluded.
Baseline characteristics of the population were systematically recorded: demographic characteristics (sex, body mass index, age), habits (smoking status), medical background (diabetes, hypertension, dyslipidemia, ischemic heart disease, history of familial cardiovascular disease, heart failure, history of supraventricular arrhythmia, history of venous thromboembolic disease, known pulmonary hypertension, peripheral arterial disease, history of stroke, chronic obstructive pulmonary disease or asthma, chronic lung failure, i.e., requiring home oxygen therapy, chronic kidney disease, defined as glomerular filtration rate < 60 ml/kg/m2, active cancer or immunosuppression), initial presentation (including time from symptoms onset), and hospitalization duration. We assessed several biomarkers at admission: leukocytes, C-reactive protein, hemoglobin, D-dimers, potassium, creatinine and troponin. We also recorded the main drugs that were administered to the patient (including heparin, oral anticoagulant drugs, antibiotics, immunotherapy, catecholamine, steroids) and major events that occurred during hospitalization, including pulmonary embolism, intensive care admission, extracorporeal life support, type of ventilation (non-invasive oxygen therapy, high-flow oxygen therapy, continuous positive airway pressure, mechanical ventilation).
Electrocardiograms at admission were systematically analyzed. We also assessed potential occurrence of new ECG abnormalities in patients with ECG performed during hospitalization. In case of multiple ECGs, we considered the first ECG done during hospitalization. The ECG interpretation was performed by two independent physicians blinded to clinical status and outcome. Any disagreement in interpretation between readers was resolved by consensus. The following ECG parameters were systematically assessed: (1) heart rate, (2) sinus rhythm status, (3) atrial and ventricular arrhythmias, (4) PR duration (in milliseconds), (5) atrioventricular block, (6) low voltage (defined as low amplitude of QRS complexes of < 10 mm in precordial leads, or < 5 mm in frontal leads), (7) Q wave, (8) S1Q3 pattern, (9) QRS duration and QRS abnormalities including bundle branch block and QRS axis, (10) repolarization abnormalities (negative T wave and/or unspecific repolarization abnormalities, ST elevation), (11) QT corrected measured with the Bazett formula, and (12) atrial or ventricular premature ventricular complexes. Prolonged QTc was defined as QTc > 460 ms.
The primary outcome was death occurring during hospitalization.
Statistical analysis was performed using MedCalc software (Ostend, Belgium) or with R Development Core Team (29) (R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria). Continuous variables with normal distribution are presented as mean ± SD and compared using Student's t-test. Continuous variables with non-normal distribution are presented as median [interquartile range (IQR)] and are compared using the Mann-Whitney U test. Qualitative variables are presented as variable (percentage) and compared using the Chi squared test or Fisher's exact test. Multivariate logistic regression models were used to assess the association between ECG abnormalities and death. We included in each logistic regression model baseline clinical characteristics and ECG abnormalities that were clinically relevant and possibly associated with death in univariate analysis (p < 0.20) using forward stepwise selection. The results are interpreted in terms of adjusted odds ratios with their associated 95% confidence interval. We performed a second multivariate analysis to identify variables independently associated with death among patients who had a second ECG during hospitalization. Sensitivity analyses were performed and did not modify the outcomes. Statistical tests were considered significant for a P-value < 0.05. This study was approved by the University Paris Saclay Institutional Review Board (CER-Paris-Saclay-2021-102).
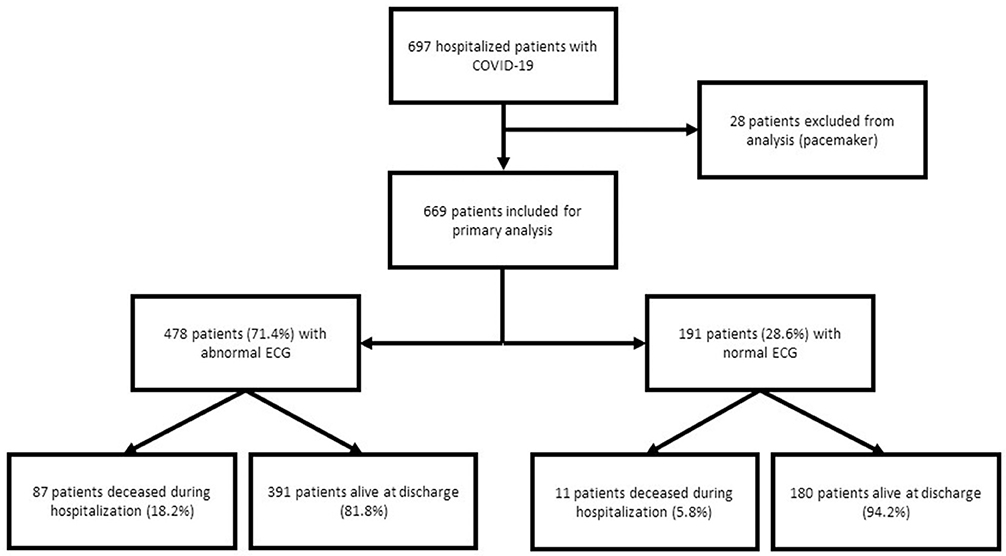
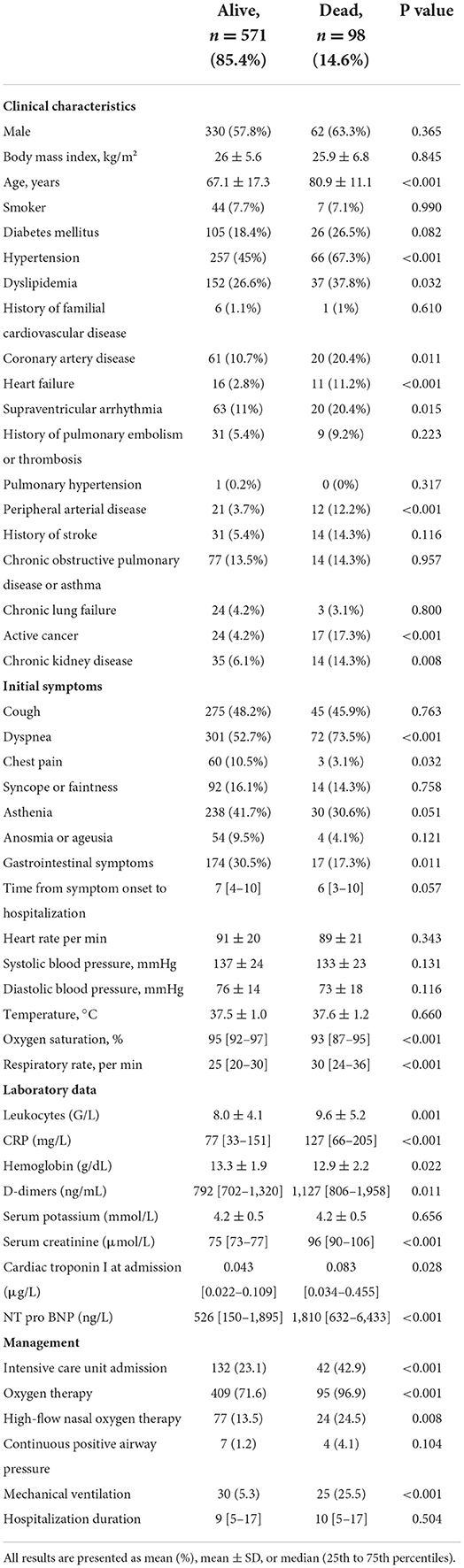
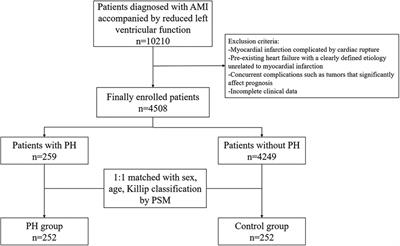
ResultsWe included 697 patients hospitalized with confirmed COVID-19. Of these patients, 28 were excluded because of pacing (Figure 1), and 669 patients were included in the primary analysis. Baseline characteristics of the global population and according to vital status are presented in Table 1. One hundred and seventy-four patients (26.0 %) were admitted in ICU. Ninety-eight patients (14.6%) died from COVID-19 during hospitalization. Mean age was 69.1 ± 17.2 years and was significantly older in deceased patients (80.9 ± 11.1 years vs. 67.1 ± 17.3 years, p < 0.001). Deceased patients more frequently had hypertension (67.3 vs. 45%, p < 0.001) and dyspnea (73.5 vs. 52.7%, p < 0.001). Mean leukocyte count was 8.2 ± 4.3 G/L and was statistically higher in the non-survival group (p = 0.001), as were CRP level (p < 0.001), D-dimers (p = 0.01), serum creatinine (p < 0.001), troponin (p = 0.03) and NT pro BNP (p < 0.001). The median time from symptoms onset to admission was 7 days, without any statistical difference between the two groups (p = 0.057). Pulmonary embolism was diagnosed in 37 patients (5.5%), heart failure in 45 patients (6.7%), acute coronary syndrome in 10 patients (1.5%) and pericarditis in 2 patients (0.3%). No myocarditis was observed.
FIGURE 1
Figure 1. Flowchart of the study.
TABLE 1
Table 1. Baseline characteristics of the study population presenting with COVID-19.
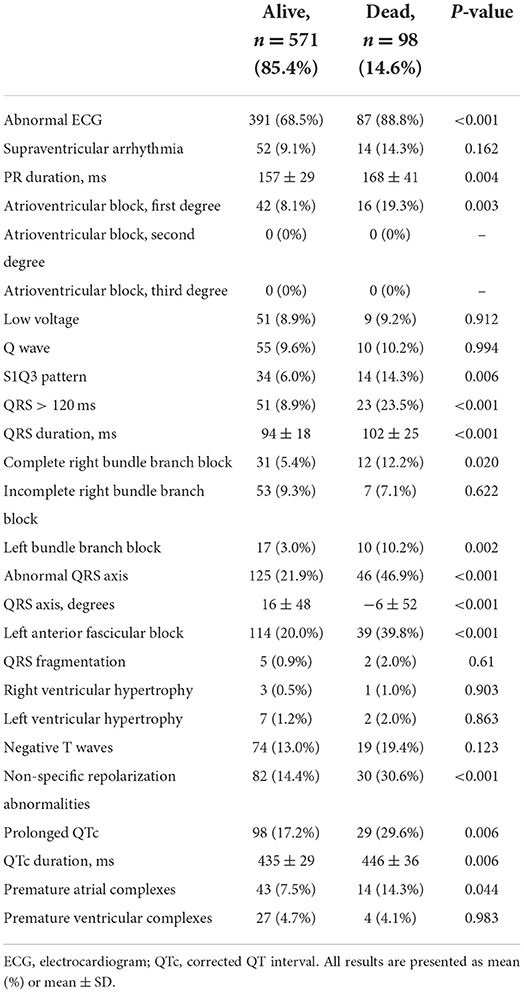
ECG characteristics at admissionThe ECG characteristics at admission are presented in Table 2. All patients had an ECG at admission, and 169 patients (25.3%) had another ECG during hospitalization. An abnormal ECG at admission was observed in 478 patients (71.4%) and was more frequently present in patients who did not survive (88.8 vs. 68.5%, p < 0.001). An abnormal ECG was also more frequently present in patients admitted in ICU than in non-ICU patients (79.3 vs. 68.7%, p < 0.01). The most common abnormality associated with death was left anterior fascicular block (39.8 vs. 20.0%, p < 0.001). Left and right bundle branch blocks were also statistically associated with death (10.2 vs. 3.0%, p = 0.002 and 12.2 vs. 5.3%, p = 0.02, respectively), as were S1Q3 pattern (14.3 vs. 6.0%, p = 0.006) and non-specific repolarization abnormalities (30.6 vs. 14.4%, p < 0.001). Mean corrected QT interval was 439 ± 31 ms (446 ± 36 ms among non-survival patients vs. 435 ± 29 ms among patients who survived, p = 0.006).
TABLE 2
Table 2. ECG characteristics at admission in patients presenting with COVID-19.
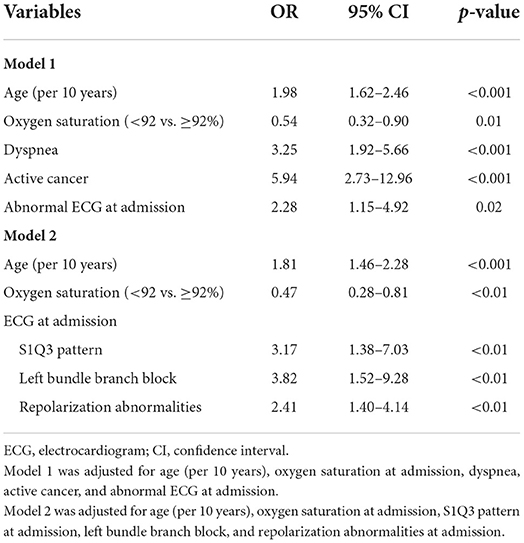
Supplementary Table 1 provides univariate analysis for identifying variables at admission associated with death. In multivariate analysis (Table 3), the presence of left bundle branch block remained statistically related to death [OR = 3.82, 95% confidence interval (CI): 1.52–9.28, p < 0.01], as did S1Q3 pattern (OR = 3.17, 95% CI: 1.38–7.03, p < 0.01) and repolarization abnormalities (OR = 2.41, 95% CI: 1.40–4.14, p < 0.01).
TABLE 3
Table 3. Multivariate analysis for identifying variables at admission independently associated with death.
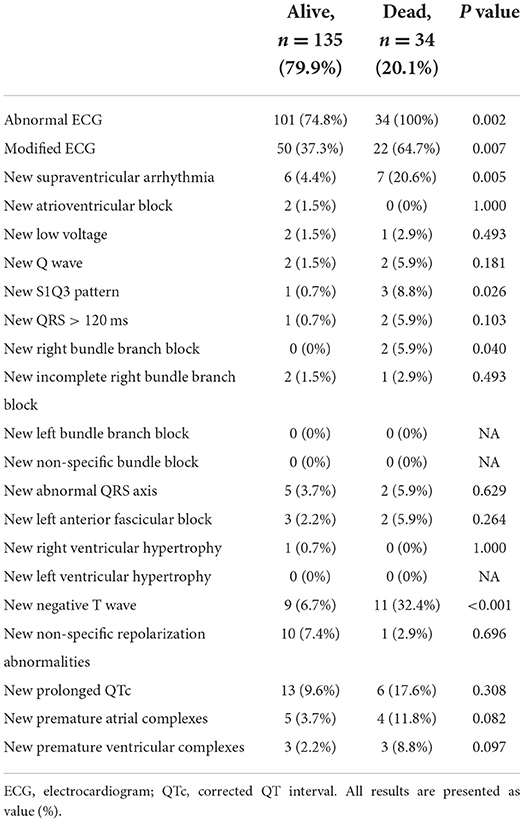
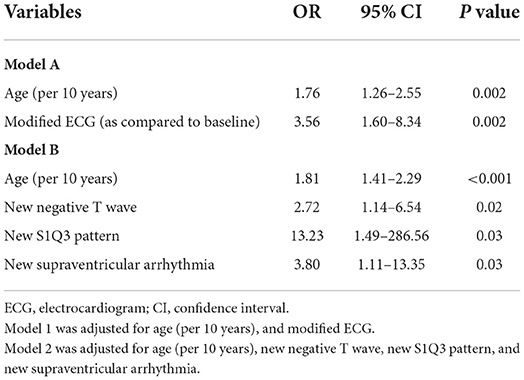
Characteristics of ECG performed after admissionThe characteristics of ECG performed after admission in 169 patients are presented in Table 4. An abnormal ECG was observed in 135 patients (79.9%) and 72 (42.9%) had a modified ECG as compared to the ECG at admission. The most frequent new ECG abnormality was T wave inversion (20 patients, 11.8%). Thirteen patients (7.7%) had a new supraventricular arrhythmia. Four patients (1.8%) presented a new S1Q3 pattern. Among the 169 patients who had a new ECG during hospitalization, 13 had a combination of hydroxychloroquine (HCQ) and azithromycin (AZT) regimen. The mean QTc interval was 443 ± 24 in patients under HCQ/AZT combination regimen vs. 437 ± 32 in patients without such treatment (p = 0.29). No patient in the HCQ/AZT group had a new prolonged QTC nor a QTc >500 ms. In multivariate analysis (Table 5), the occurrence of the following ECG parameters was associated with death: new repolarization abnormality (OR = 2.72, 95% CI: 1.14–6.54, p = 0.02), new S1Q3 pattern (OR = 13.23, 95% CI: 1.49–286.56, p = 0.03) and new-onset supraventricular arrhythmia (OR = 3.8, 95% CI: 1.11–13.35, p = 0.03).
TABLE 4
Table 4. New ECG abnormalities observed during hospitalization, n = 169.
TABLE 5
Table 5. Summary of multivariate analysis for identifying variables independently associated with death among patients who had a second ECG during hospitalization, n = 169.
DiscussionIn the present study, we evaluated the ECG characteristics of patients hospitalized with COVID-19. The main results are: (1) in a large cohort of COVID-19 patients, an abnormal ECG was observed in 478 patients (71.4%) and was more frequently described in patients who did not survive; (2) left bundle branch block, S1Q3 pattern and repolarization abnormalities at admission were associated with death; (3) new repolarization abnormality, new S1Q3 pattern and new-onset supraventricular arrhythmia during hospitalization were associated with death.
It is now well-known that ECG is modified by systemic inflammation, which may be consecutive to COVID infection or any of its complications (6, 8). In previous studies, an abnormal ECG was observed in between 47 and 93% of COVID-19 patients (23, 24, 26–28). In our study, 71.4% of patients presented with ECG abnormalities: 68.7% in patients admitted in medical wards and 79.3% in ICU patients. To our knowledge, no study reported on the proportion of ECG abnormalities in non-ICU COVID-19 patients. Even when these last patients presented with less severe COVID-19 involvement, most of them had ECG abnormalities and physicians should be aware that ECG should be systematically performed for a prognostic assessment. The observed differences between studies may be explained by different study populations, with a high prevalence of ECG abnormalities in the ICU. About one quarter of patients were admitted in ICU in the present study, which included all consecutive patients hospitalized in our university hospital during 2020.
In our study, CRP was not associated with ECG abnormality (p = 0.96), but was associated with new-onset supraventricular arrhythmia [mean CRP level was 163.4 mg/L in the group of patients with new-onset supraventricular arrhythmia vs. 107.2 mg/L in the group of patients without new-onset supraventricular arrhythmia (p = 0.04)]. This is consistent with previous studies, which identified systemic inflammation caused by COVID-19 as a key factor in arrhythmogenesis (14, 30). In the present study, new-onset supraventricular arrhythmia was associated with death in multivariate analysis which is consistent with previous studies (24, 26, 31). In our study, no significant difference in QTc duration was found between patients with HCQ/AZT combination therapy and patients without treatment. This is in contradiction with the study by Bernardini et al. (32); where the HCQ/AZT combination therapy caused a significantly increase of QT interval compared to HCQ alone or no treatment group. This may be due to the fact that in our institution, we prescribed HCQ/AZT combination regimen during a limited period (04/06/2020 to 04/16/2020) in a limited number of patients (n = 13) and ECG was not systematically performed. Other ECG abnormalities that we describe in our study are consistent with the literature (26–28, 33). Interestingly, we found that left bundle branch block, S1Q3 pattern and repolarization abnormalities were independently associated with death in cases of COVID-19.
ECG abnormalities may be associated with death by many mechanisms. Systemic inflammation can increase cardiac demand, and destabilize vascular plaque, resulting in myocardial infarction (17–20), and thereby cause T wave inversion or non-specific repolarization abnormalities, which can worsen the prognosis (8). In a postmortem study (21), the most common pathological cause of myocyte necrosis in patients with COVID-19 infection was microthrombi. Indeed, only 3 patients in this study had a ST-elevation myocardial infarction, supporting the hypothesis of intra-coronary microthrombi rather than macrothrombus. Another mechanism of death during COVID-19 is pulmonary embolism. It is now well-established that COVID-19 significantly increases the risk of pulmonary embolism (11, 34). In our study, S1Q3 pattern was statistically associated with death. This S1Q3 pattern is not pathognomonic for pulmonary embolism, but the occurrence of this ECG parameter may be helpful for the risk stratification of COVID-19 patients.
Potential limitations of the present study merit consideration. First, we recruited patients presenting with COVID-19 from the first wave and we did not study the ECG characteristics associated with new variants. Even if the prognosis of COVID-19 caused by these new variants is better as compared to the first wave (4), the most recent waves were accompanied by great contagiousness and many hospitalizations (3, 4). Second, in our study, ECG was not systematically repeated during hospitalization, and we analyzed at least two ECG during hospitalization in 169 selected patients, leading to a potential bias of interpretation. However, experts blinded to clinical data and outcome interpreted the ECG, and the occurrence of new ECG abnormalities was associated with death and was consistent with the results of ECG at admission. Finally, the low number of patients presenting with new S1Q3 pattern during hospitalization does not allow to definitively conclude on the prognostic impact of S1Q3 pattern.
ConclusionThe presence of abnormal ECG during COVID-19 is frequent. Several ECG abnormalities such as left bundle branch block, S1Q3 pattern, repolarization abnormalities and supraventricular arrhythmia are associated with death as well as the occurrence of ECG abnormalities during hospitalization. Clinicians should be aware of the usefulness of ECG for risk stratification during COVID-19.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving human participants were reviewed and approved by University Paris Saclay Institutional Review Board (CER-Paris-Saclay-2021-102). The patients/participants provided their written informed consent to participate in this study.
Author contributionsMH-M, GC, and NM contributed to conception and design of the study. GC and MH-M analyzed ECG and wrote the first draft of the manuscript. SG, AC, VA, A-SL, and MO obtained data. GC organized the database. MH-M, NM, and HH performed the statistical analysis. NM, SB, and OD wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.993479/full#supplementary-material
References3. Wang R, Chen J, Wei G-W. Mechanisms of SARS-CoV-2 evolution revealing vaccine-resistant mutations in Europe and America. J Phys Chem Lett. (2021) 12:11850–7. doi: 10.1021/acs.jpclett.1c03380
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Aleem A, Akbar Samad AB, Slenker AK. Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus (COVID-19). In: StatPearls. Treasure Island, FL: StatPearls Publishing (2022).
PubMed Abstract | Google Scholar
5. Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19). In: StatPearls. Treasure Island, FL: StatPearls Publishing (2022).
PubMed Abstract | Google Scholar
6. Ejaz H, Alsrhani A, Zafar A, Javed H, Junaid K, Abdalla AE, et al. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Health. (2020) 13:1833–9. doi: 10.1016/j.jiph.2020.07.014
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Sawalha K, Abozenah M, Kadado AJ, Battisha A, Al-Akchar M, Salerno C, et al. Systematic review of COVID-19 related myocarditis: insights on management and outcome. Cardiovasc Revasc Med. (2021) 23:107–13. doi: 10.1016/j.carrev.2020.08.028
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Kwong JC, Schwartz KL, Campitelli MA, Chung H, Crowcroft NS, Karnauchow T, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. (2018) 378:345–53. doi: 10.1056/NEJMoa1702090
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Chen L, Li X, Chen M, Feng Y, Xiong C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc Res. (2020) 116:1097–100. doi: 10.1093/cvr/cvaa078
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Bompard F, Monnier H, Saab I, Tordjman M, Abdoul H, Fournier L, et al. Pulmonary embolism in patients with COVID-19 pneumonia. Eur Respir J. (2020) 56:2001365. doi: 10.1183/13993003.01365-2020
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Poissy J, Goutay J, Caplan M, Parmentier E, Duburcq T, Lassalle F, et al. Pulmonary embolism in patients with COVID-19: awareness of an increased prevalence. Circulation. (2020) 142:184–6. doi: 10.1161/CIRCULATIONAHA.120.047430
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Suh YJ, Hong H, Ohana M, Bompard F, Revel MP, Valle C, et al. Pulmonary embolism and deep vein thrombosis in COVID-19: a systematic review and meta-analysis. Radiology. (2021) 298:E70–80. doi: 10.1148/radiol.2020203557
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Siripanthong B, Nazarian S, Muser D, Deo R, Santangeli P, Khanji MY, et al. Recognizing COVID-19-related myocarditis: the possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm. (2020) 17:1463–71. doi: 10.1016/j.hrthm.2020.05.001
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Welt FGP, Shah PB, Aronow HD, Bortnick AE, Henry TD, Sherwood MW, et al. Catheterization laboratory considerations during the coronavirus (COVID-19) pandemic: from the ACC's interventional council and SCAI. J Am Coll Cardiol. (2020) 75:2372–5. doi: 10.1016/j.jacc.2020.03.021
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Driggin E, Madhavan MV, Bikdeli B, Chuich T, Laracy J, Biondi-Zoccai G, et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. J Am Coll Cardiol. (2020) 75:2352–71. doi: 10.1016/j.jacc.2020.03.031
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Hauguel-Moreau M, Pillière R, Prati G, Beaune S, Loeb T, Lannou S, et al. Impact of Coronavirus Disease 2019 outbreak on acute coronary syndrome admissions: four weeks to reverse the trend. J Thromb Thrombolysis. (2021) 51:31–2. doi: 10.1007/s11239-020-02201-9
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Bavishi C, Bonow RO, Trivedi V, Abbott JD, Messerli FH, Bhatt DL. Special article - acute myocardial injury in patients hospitalized with COVID-19 infection: a review. Prog Cardiovasc Dis. (2020) 63:682–9. doi: 10.1016/j.pcad.2020.05.013
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Pellegrini D, Kawakami R, Guagliumi G, Sakamoto A, Kawai K, Gianatti A, et al. Microthrombi as a major cause of cardiac injury in COVID-19: a pathologic study. Circulation. (2021) 143:1031–42. doi: 10.1161/CIRCULATIONAHA.120.051828
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Hauguel-Moreau M, Mansencal N, Gault E, Prati G, Dubourg O, Annane D. SARS-CoV-2 in coronary blood from thrombus aspiration in a patient with myocardial infarction. Coron Artery Dis. (2022) 33:335–6. doi: 10.1097/MCA.0000000000001107
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Bertini M, Ferrari R, Guardigli G, Malagù M, Vitali F, Zucchetti O, et al. Electrocardiographic features of 431 consecutive, critically ill COVID-19 patients: an insight into the mechanisms of cardiac involvement. Europace. (2020) 22:1848–54. doi: 10.1093/europace/euaa258
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Denegri A, Pezzuto G, D'Arienzo M, Morelli M, Savorani F, Cappello CG, et al. Clinical and electrocardiographic characteristics at admission of COVID-19/SARS-CoV2 pneumonia infection. Intern Emerg Med. (2021) 16:1451–6. doi: 10.1007/s11739-020-02578-8
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Kowal J, Ahmad MI, Li Y, Soliman EZ. Prognostic significance of electrocardiographic right ventricular hypertrophy in the general population. J Electrocardiol. (2019) 54:49–53. doi: 10.1016/j.jelectrocard.2019.03.008
PubMed Abstract | CrossRef Full Text | Google Scholar
26. McCullough SA, Goyal P, Krishnan U, Choi JJ, Safford MM, Okin PM. Electrocardiographic findings in coronavirus disease-19: insights on mortality and underlying myocardial processes. J Card Fail. (2020) 26:626–32. doi: 10.1016/j.cardfail.2020.06.005
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Long B, Brady WJ, Bridwell RE, Ramzy M, Montrief T, Singh M, et al. Electrocardiographic manifestations of COVID-19. Am J Emerg Med. (2021) 41:96–103. doi: 10.1016/j.ajem.2020.12.060
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Kelesoglu S, Yilmaz Y, Ozkan E, Calapkorur B, Gok M, Dursun ZB, et al. New onset atrial fibrilation and risk faktors in COVID-19. J Electrocardiol. (2021) 65:76–81. doi: 10.1016/j.jelectrocard.2020.12.005
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Ghio S, Baldi E, Vicentini A, Lenti MV, Di Sabatino A, Di Matteo A, et al. Cardiac involvement at presentation in patients hospitalized with COVID-19 and their outcome in a tertiary referral hospital in Northern Italy. Intern Emerg Med. (2020) 15:1457–65. doi: 10.1007/s11739-020-02493-y
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Bernardini A, Ciconte G, Negro G, Rondine R, Mecarocci V, Viva T, et al. Assessing QT interval in COVID-19 patients:safety of hydroxychloroquine-azithromycin combination regimen. Int J Cardiol. (2021) 324:242–8. doi: 10.1016/j.ijcard.2020.09.038
PubMed Abstract | CrossRef Full Text | Google Scholar
33. De Carvalho H, Leonard-Pons L, Segard J, Goffinet N, Javaudin F, Martinage A, et al. Electrocardiographic abnormalities in COVID-19 patients visiting the emergency department: a multicenter retrospective study. BMC Emerg Med. (2021) 21:141. doi: 10.1186/s12873-021-00539-8
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Hauguel-Moreau M, Hajjam ME, De Baynast Q, Vieillard-Baron A, Lot AS, Chinet T, et al. Occurrence of pulmonary embolism related to COVID-19. J Thromb Thrombolysis. (2021) 52:69–75. doi: 10.1007/s11239-020-02292-4
留言 (0)