
記住我






Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released.
Author affiliations: Federal Institute of Education, Science, and Technology of Ceará, Fortaleza, Brazil (F.R. Martins-Melo); Harvard T.H. Chan School of Public Health, Boston, Massachusetts, USA (M.C. Castro); Universidade Federal de Minas Gerais, Belo Horizonte, Brazil (A.L.P. Ribeiro); Federal University of Ceará, Fortaleza (J. Heukelbach); Federal University of Rio de Janeiro, Rio de Janeiro, Brazil (G.L. Werneck); State University of Rio de Janeiro, Rio de Janeiro (G.L. Werneck)
Chagas disease, caused by the protozoan Trypanosoma cruzi, is a neglected public health problem in Latin America (1). It is the most common infectious cause of cardiomyopathy worldwide and for co-infections might play a role in clinical prognosis of COVID-19 patients (2,3). In Brazil, ≈1.4–3.4 million persons were estimated to be chronically infected with T. cruzi during 2015; 0.4–1.0 million of those persons had chronic Chagas heart disease (4).
On March 11, 2020, the World Health Organization declared COVID-19 a pandemic (5). In Brazil, a case of COVID-19 was detected on February 26, 2020, and a death from COVID-19 occurred on March 12, 2020 (5). COVID-19 vaccination campaigns started in late January 2021 (6). By September 18, 2022, there were >33.7 million confirmed cases and ≈685,000 deaths in Brazil (7).
Spread of COVID-19 in Chagas disease‒endemic areas is a public health challenge because of advanced age of chronically infected patients and high occurrence of heart complications (2). This finding probably increases risk for severe forms and deaths from COVID-19 in co-infected patients (5,8). We assessed epidemiologic characteristics and distribution of deaths related to COVID-19 and Chagas disease co-infection in Brazil during March-December 2020.
We conducted a nationwide analysis using mortality rate data for 2020 (preliminary records), obtained from the Brazilian Mortality Information System database (https://datasus.saude.gov.br/transferencia-de-arquivos) and extracted on September 4, 2021. We included all deaths reported from March 1‒December 31, 2020, in which Chagas disease (International Classification of Diseases, 10th revision [ICD-10], codes B57–57.5, K23.1, and K93.1) and COVID-19 (ICD-10 codes B34.2, U0.71 or U0.72) were mentioned on the same death certificate as underlying or contributing to death.
Available sociodemographic and clinical data included sex (male, female), age (<1–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, >80 years), education (years of study: none, 1–3, 4–7, 8–11, >12), ethnicity (White, Black/Afro-Brazilian, mixed/Pardo Brazilian, Asian, indigenous), marital status (single, married, divorced/separated, widowed, other), place of residence (regions, states, municipalities), date of death (epidemiologic week, month), place of death (hospital, other health establishment, home, public thoroughfare, others), and underlying/contributing causes of death. We calculated cumulative mortality rates per 100,000 inhabitants and rate ratios with 95% CIs stratified by sex, age group, place of residence, ethnicity, and educational level using population estimates from the Brazilian Institute of Geography and Statistics as the denominator. We assessed significant differences by χ2 test, performed analyses using Stata version 11.2 (StataCorp, https://www.stata.com), and created maps using ArcGIS version 9.3 (Esri, https://www.esri.com). Data were obtained anonymized, with no possibility of subject identification.
Figure 1
![Number of deaths related to Chagas disease and COVID-19 co-infection, by month (A) and epidemiologic week (B) of death, Brazil, March–December 2020. Data shown are from the epidemiologic week of the first reported death related to Chagas disease and COVID-19 co-infection (March 26, 2020) to December 31, 2020 (epidemiologic weeks from 13 [March 22–28, 2020] to 53 [December 27, 2020–January 2, 2021; data available until December 31, 2020], according to the 2020 epidemiologic calendar (https://portalsinan.saude.gov.br/calendario-epidemiologico-2020). Red bars indicate the number of deaths related to Chagas and COVID-19 co-infection.](https://wwwnc.cdc.gov/eid/images/21-2158-F1-tn.jpg)
Figure 1. Number of deaths related to Chagas disease and COVID-19 co-infection, by month (A) and epidemiologic week (B) of death, Brazil, March–December 2020. Data shown are from the epidemiologic week of...
Of 1,337,730 deaths recorded in Brazil during March‒December 2020, we identified 492 deaths in which Chagas disease and COVID-19 were on the same death certificates (9.1% [492/5,395] of Chagas disease‒related deaths and 0.2% [492/222,121] of COVID-19‒related deaths for that period). The cumulative co-infected mortality rate was 0.23 (95% CI 0.21–0.25) deaths/100,000 inhabitants. COVID-19 was mentioned as the underlying cause in most co-infected deaths (88.2% [434/492]), of which 77.2% (335/492) were laboratory-confirmed COVID-19 deaths (B34.2 + U07.1). Chagas disease was the underlying cause in 7.7% (38/492) of co-infected deaths, with predominance of the chronic cardiac form (B57.2) (Table 1). The number of co-infected deaths peaked in July, in epidemiologic week 30 (July 19–25) (Figure 1), following the patterns of COVID-19 deaths during the 2020 pandemic time (Appendix Figures 1‒3).
Overall, co-infected deaths were predominant among men (51%), persons 70–79 years of age (37%), persons of mixed ethnicity (44.9%), married persons (44.5%), persons who had schooling (1–3 years of study) (33.2%), and persons who resided in the Southeast region (43.7%) and São Paulo state (27%). The mean (+SD) age at death was 73.9 (+12.2) years, median (range) age at death was 75.5 (30.7–104.4) years, and 87% of deaths occurred in hospitals (Table 2).
Figure 2
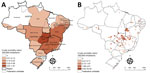
Figure 2. Spatial distribution of cumulative mortality rates per 100,000 inhabitants related to Chagas disease and COVID-19 co-infection by geographic units of residence, Brazil, March–December 2020. A) State-level crude rates. B) Municipality-level...
Cumulative mortality rates were higher for men than for women, but not significantly. Highest age-specific mortality rates were found for older age groups, the maximum in persons >80 years of age (3.29/100,000 inhabitants). Persons of Afro-Brazilian ethnicity had higher mortality rates than White persons. Mortality rates were higher among persons who had low levels of education (none and 1‒3 years of study) than persons who had advanced education. The Central-West region had the highest regional mortality rate, followed by Southeast and Northeast regions (Table 2). Federal District (1.57 deaths/100,000 inhabitants), Goiás (1.38 deaths /100,000 inhabitants), and Bahia (0.36 deaths /100,000 inhabitants) had the highest state-level mortality rates (Figure 2, panel A; Appendix Table).
A total of 4.1% (231/5,570) of municipalities in 22 of the 27 states of Brazil recorded >1 co-infected deaths during 2020. Cumulative mortality rates were 0.04–44.40 deaths/100,000 inhabitants among municipalities in Brazil that recorded >1 co-infected death. Municipalities that had high co-infected death rates were found mainly in the central region of Brazil (Goiás, Minas Gerais, São Paulo, Bahia, and the Federal District) (Figure 2, panel B).
We found higher death rates for Chagas disease and COVID-19 co-infection among older persons, persons who had Afro-Brazilian ethnicity, persons with low education levels, and persons lived in an area to which Chagas disease was previously endemic. The high co-infection mortality rate for older age groups is consistent with patterns of deaths for both infections in Brazil during 2020 because the highest age-specific death rates for the diseases were for these subgroup populations (9–11). Consistent with other reports for both infections, we found that the higher death rates found for persons of Black ethnicity and with low educational levels indicate social and structural inequities and health disparities in determination of severe illness and death related to Chagas disease and COVID-19 in Brazil (9,11,12).
The areas of Brazil that had the highest mortality rates were major disease-endemic areas for vector transmission in the past in the Central-West, Southeast, and Northeast regions (4,9,13). The extensive spread of COVID-19 in Brazil during 2020, including Chagas disease-endemic areas, caused substantial geographic overlap between the infections, increasing the risk of chronic Chagas disease patients, principally those with cardiac involvement, contracting SARS-CoV-2 infection (2,5). The high mortality rate for the Federal District when compared with other states, and the high number of co-infected deaths observed in state capitals of Brazil, such as Brasília, São Paulo, Goiânia, and Salvador, reflect urbanization of Chagas disease because of intense migratory movement from rural areas to urban areas in Brazil during the past 3 decades (9,14).
Our study’s limitations were mainly related to coverage and quality of secondary mortality rate data (9,13). Brazilian Mortality Information System data for 2020 are preliminary and might not represent all deaths for 2020 because it is subject to corrections, especially underlying causes of death. Even if minimal, frequencies might change after definitive consolidation (15). Other potential limitations are misclassification or underreporting and delays in reporting of COVID-19 deaths, especially in places where healthcare services were under stress because of the large COVID-19 caseload (6).
It is likely that a large number of patients who have chronic Chagas disease, especially the undetermined form, are not given a diagnosis in Brazil. Therefore, there might be more deaths of patients who have both infections than reported in this study. Schooling, ethnicity, and marital status included a considerable proportion of incomplete/unknown data, and these findings should be interpreted with caution.
Our findings show marked sociodemographic and geographic variations in deaths related to Chagas disease and COVID-19 co-infection in Brazil during 2020, occurring mainly in residents of Chagas disease‒endemic areas and disproportionately affecting susceptible population groups. The real effect of death from co-infection might be underestimated in Brazil. Efforts must be made to ensure a high COVID-19 vaccination coverage, improve access to healthcare services, and provide adequate clinical management for co-infected patients especially in patients who have chronic Chagas disease.
Dr. Martins-Melo is a research scientist at the Federal Institute of Education, Science, and Technology of Ceará, Fortaleza, Brazil. His primary research interests include control and epidemiology of neglected and poverty-related diseases.
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
留言 (0)