
記住我
Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released.
Author affiliations: Public Health Seattle and King County, Seattle, Washington, USA (J.W. Lewis, J. Loughran, S. Clark, C. Harrison, M. Gacetta); Centers for Disease Control and Prevention, Atlanta, Georgia, USA (L. Deng, J. Varghese, J.A. Jernigan. K.E. Fleming-Dutra)
COVID-19 mRNA vaccines demonstrated high efficacy (>94%) against COVID-19 in clinical trials (1,2). However, initial observational vaccine effectiveness (VE) estimates against infection among residents of skilled nursing facilities (SNFs), a high-risk population, were lower, 53%–75% (3). A local health department in Washington, USA, investigated a COVID-19 outbreak of the P.1 (Gamma) variant in April 2021 in an SNF and estimated VE of 2 mRNA vaccine doses against SARS-CoV-2 infection. The Centers for Disease Control and Prevention reviewed the activity to confirm it was conducted consistent with applicable federal law and organizational policy. This investigation was defined as having met the requirements for public health surveillance as outlined in 45 C.F.R. part 46.102(l) (2).
Daily symptom screening of residents and staff had been ongoing in this SNF since March 2020. Routine antigen testing of symptomatic residents with BinaxNOW tests (Abbott Diagnostics, https://www.diagnostics.abbott) was performed upon symptom recognition; routine testing of staff was ongoing. Nucleic acid amplification test (NAAT) confirmation of all positive antigen results and antigen negative results for symptomatic persons was performed. The outbreak index case was a symptomatic fully vaccinated resident identified on April 16, 2021. All residents and staff were tested immediately and again every 3–7 days for the duration of the outbreak period, April 15–May 9, 2021.
We defined a case as a positive SARS-CoV-2 antigen or NAAT result in a resident of the SNF. The local health jurisdiction requested viral whole-genome sequencing (WGS) for all positive specimens. Washington State Department of Health Public Health Laboratories and their partners identified SARS-CoV-2 variant status for individual cases through WGS and recorded cases in the Washington Disease Reporting System.
The SNF conducted vaccination clinics on January 12, February 2, and February 23, 2021. We defined vaccination status as fully vaccinated with 2 doses, if receipt of second vaccine dose was >14 days before the outbreak began (4), and unvaccinated if no COVID-19 vaccine had been received before or during the outbreak. We excluded from the VE analysis residents who were partially vaccinated (i.e., who had received 1 vaccine dose or had received a second dose <14 days before the outbreak). We ascertained vaccination status through Washington Immunization Information System and facility medical records. We obtained age, race, ethnicity, and comorbidity information from facility medical records.
We calculated VE for 2 mRNA vaccine doses on the basis of relative risk (RR) of infection in vaccinated versus unvaccinated residents using a log-binomial model and adjusted for potential confounders of age (<85 vs. >85 years) and race (White vs. all other residents with nonmissing race). We used the equation VE = 100% × (1 − RR). We conducted a separate analysis limited to WGS-confirmed P.1 cases to estimate VE against P.1 infection.
Figure
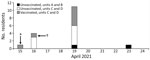
Figure. Date of first positive SARS-COV-2 specimen collection among residents in a skilled nursing facility, Washington, April 2021, Cases shown are restricted to the 17 resident cases included in vaccine effectiveness...
Of 63 residents present during the outbreak, 43 (68%) were fully vaccinated with 2 doses and 16 (25%) were unvaccinated; we excluded 4 partially vaccinated residents from the analysis. Thirty-six (84%) of 43 vaccinated residents received vaccination during the onsite clinics. Seven residents (16%) were fully vaccinated at other locations. Nineteen residents tested positive for SARS-CoV-2 during the outbreak (Figure; Appendix Figure); 2 of those were partially vaccinated and excluded from analysis. Of the 17 included outbreak cases, 7 were in fully vaccinated residents. Thirteen (77%) of 17 outbreak cases had WGS data; all were identified as P.1 lineage.
Most of the 59 residents included in the analysis were White (83%) and female (63%); the age range was >60 years (Table). Ethnicity was unknown for 56% of residents. All residents had ≥2 underlying health conditions that may increase risk for severe COVID-19.
The attack rate in unvaccinated residents was 63% (10/16) versus 16% (7/43) in fully vaccinated residents (adjusted RR 4.0, 95% CI 1.8–8.9). Unadjusted VE against infection was 74.0% (95% CI 43.4%–88.0%). Age-adjusted and race-adjusted VE against infection among 57 residents (excluding 2 residents with unknown race) was 75.0% (95% CI 44.5%–88.7%). Age- and race-adjusted VE against WGS-confirmed P.1 infection among 53 residents (excluding 2 residents with unknown race) was 80.0% (95% CI 46.4%–92.6%). In this outbreak, vaccination was associated with decreased likelihood of infection. Our estimated VE of 75% (95% CI 45%–89%) against infection is consistent with other findings of mRNA VE against infection with other pre-Delta variants among residents of SNFs (3–7).
The first limitation of our study is that unvaccinated residents might have differed from vaccinated in ways we did not measure, including in the use of mitigation behaviors. In addition, the demographics of residents in this facility may differ from the broader general long-term care resident population.
In conclusion, our evaluation indicates that receiving 2 mRNA vaccine doses was effective in reducing the likelihood of testing positive for SARS-CoV-2 during an outbreak of P.1 lineage variant in an SNF. VE against P.1 is comparable to that against other pre-Delta SARS-CoV-2 variants among long-term care residents.
Dr. Lewis is a board-certified physician in internal medicine, infectious disease, and preventive medicine. He is currently the health officer for the Snohomish County Health District; prior to this position and during the initial composition of this article he was a medical epidemiologist at Public Health Seattle & King County helping to oversee the response to the SARS-CoV-2 pandemic in healthcare settings.
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
留言 (0)