Ethics Compliance
This study was approved by the ethics committees of the Yokohama City University Medical Center (approval no. B220400040; April 18, 2022), Yokohama City University Hospital (approval no. B220300073; April 18, 2022), Yokohama Municipal Citizen’s Hospital (approval no. 21-03-03; March 9, 2021), Kanagawa Cancer Center (approval no. 2021-39; July 12, 2021), and NTT Medical Center Tokyo (approval no. 21-146; March 2, 2022), Japan. The requirement for written informed consent was waived by the ethics committee because of the retrospective study design. The opportunity to withdraw consent was provided on the institutional websites. This study was conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines and complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [16].
Study Design, Setting, and Patients
This was a multicenter retrospective observational study that analyzed the medical records of patients with cancer who underwent fluoroscopy-guided NSNB via the transintervertebral disc approach. The participants were selected from five institutions—Yokohama City University Medical Center, Yokohama City University Hospital, Yokohama Municipal Citizen’s Hospital, Kanagawa Cancer Center, or NTT Medical Center Tokyo—between April 2005 and October 2020. The inclusion criteria were as follows: age 20 years or older, and patients with cancer who had undergone NSNB via the transintervertebral disc approach. Patients who underwent NSNB via approaches other the transintervertebral disc approach were excluded.
Neurolytic Splanchnic Nerve Block: Transintervertebral Disc Approach to the Retrocrural Space Using a Single Needle
In this study, patients indicated for NSNB were those who consulted the anesthesiologists at each institution for control of cancer pain. The patients were evaluated by anesthesiologists with expertise in interventional treatment, and deemed suitable for undergoing NSNB on the basis of their pain and imaging findings.
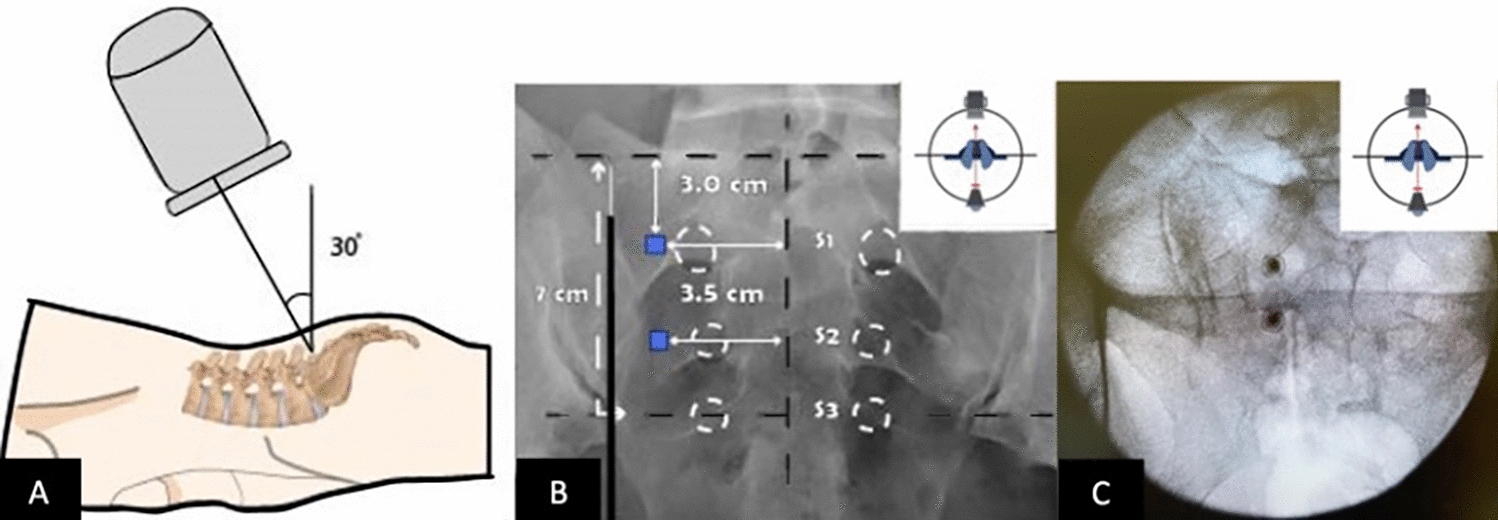
All procedures were performed by anesthesiologists specialized in pain intervention. All participants received NSNB using a standardized, fluoroscopically guided, transintervertebral disc approach technique to the retrocrural space with a single needle. The blocks were performed with patients in the prone position; a mild oblique or side lying position was adopted if the supine position was difficult because of pain. The patients were prepared by placing a sterile draping over their backs (Fig. 1i). Subsequently, the intervertebral discs ranging from T11 to L2 were observed under fluoroscopy and local anesthesia was delivered at the needle insertion sites (2.5–6.5 cm from the midline at the level of intervertebral discs T11–T12, T12–L1, or L1–L2). When we performed NSNB, and left-sided puncture was our first choice. This is because the descending aorta is often located on the left side, and a left-sided puncture allows us to avoid the aorta from the direction of the needle (Fig. 1v is an example). Under fluoroscopic guidance, a 21-gauge, 15-cm needle was inserted through the predetermined site toward the intervertebral disc in a predetermined direction. When the tip of the needle encountered the disc, it was advanced until it penetrated the disc (Fig. 1ii). Penetration was confirmed when the depth of the needle coincided with the predetermined depth and by the loss-of-resistance technique using a syringe containing sterile saline (Fig. 1iii, iv). After verification of the placement of the needle tip through radiography, 10–30 ml of local anesthesia and contrast mixture were injected. After administering the local anesthetic and contrast mixture, we carefully checked that the contrast spread remained within the vertebral body on the anteroposterior view (Fig. 1vi, ix) and in front of the vertebral body on the lateral view (Fig. 1vii), and that there was no injection into arteries or veins. On confirming satisfactory pain relief and adequate spread of the contrast medium (Fig. 1vi, vii, ix), we performed a motor and sensory examination of the lower extremities after 15–20 min. These processes were implemented to prevent major organ damage during or after alcohol injection. Subsequently, a neurolytic agent (10–30 ml of absolute alcohol) was injected through the needle. During the administration of the absolute alcohol, we also carefully checked for the appearance of any new neurological findings. Following NSNB, patients were kept in the prone or supine position for at least 120 min [12].
Measurement
We extracted patient data from electronic medical records that included the following baseline characteristics: age, sex, body mass index (BMI), primary tumor site, extent of disease, metastatic locations, history of anticancer treatment, and Eastern Cooperative Oncology Group (ECOG) Performance Status score. ECOG Performance Status score describes a patient’s level of functioning in terms of their ability to care for themself, daily activity, and physical ability (walking, working, etc.). Score 1—restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light housework, office work. Score 2—ambulatory and capable of all selfcare but unable to carry out any work activities; up and about more than 50% of the waking hours. Score 3—capable of only limited selfcare; confined to a bed or chair more than 50% of the waking hours. Score 4—completely disabled; cannot carry out any selfcare; totally confined to a bed or chair [17]. Data on the following pain characteristics were retrieved from the records: pre-block numerical rating scale (NRS) scores, pain duration, pain therapy, opioid use duration, opioid dose (equivalent oral morphine dose), post-block NRS scores (lowest scores within 14 days after block), post-block pain therapy, post-block opioid dose (lowest equivalent oral morphine dose within 14 days after block). We defined clinical success as at least 50% reduction in NRS score without opioid escalation within 14 days after block. We investigated the clinical success ratio of NSNB, absolute alcohol, neurolytic agent, dose, and the ratio of NSNB-related adverse events. Baseline and pain characteristics were compared between clinically successful and unsuccessful groups.
Outcome
The primary outcome was the efficacy of NSNB via transintervertebral disc approach technique (ratio of patients with at least 50% reduction in NRS score without opioid escalation within 14 days after block).
The secondary outcome was the safety of NSNB via transintervertebral disc approach technique (incidence ratio of NSNB-related adverse events such as hypotension, alcohol intoxication, diarrhea, and vascular puncture).
Statistical Analysis
All statistical analyses were performed using JMP version 15 (SAS Institute Inc., Cary, NC, USA). Categorical and numerical data were analyzed using the chi-squared and Mann–Whitney U tests, respectively. Statistical significance was set at P < 0.05. We did not perform a sample size calculation because of the descriptive epidemiological nature of the study.










留言 (0)