
記住我
Lifestyle factors such as diet and exercise are established targets for prevention and management of type 2 diabetes (T2D). However, improving sleep behaviors (eg, establishing a regular sleep pattern) is rarely recommended, despite evidence that disrupted sleep is associated with T2D. Sleep deprivation studies show a relationship between lack of sleep and increased glucose intolerance,1 and longitudinal studies have concluded that suboptimal sleep durations (>8 hours or ≤6 hours) increase risk of T2D.2 Individuals with T2D also commonly experience impaired sleep quality, which has implications for disease severity, condition management3 4 and psychological well-being.5 6 Additionally, people with T2D may experience ‘social jetlag’ (SJL), that is, discrepancy between an individual’s natural circadian rhythm and the timing of their sleep based on societal demands. Greater misalignment is associated with greater risk of developing T2D.7 8 Consequently, sufficient good-quality sleep appears crucial in diabetes care, but effective self-regulation can be affected by psychological factors such as negative affect and critical self-appraisals.9 It has accordingly been suggested that self-compassion (attending mindfully to oneself and one’s needs without judgment) may promote effective self-regulation, thereby reducing condition-related distress.10–12 Here, we explore associations between self-compassion, sleep quality and psychological well-being in people with T2D.
Diabetes and psychological well-beingDiabetes-related distress (DRD) is a multifaceted construct describing psychological impacts of living with diabetes.13 It includes emotional reactions and appraisals experienced in relation to diagnosis, day-to-day management and ongoing risks of T2D.14 Growing evidence shows that high DRD adversely affects self-management behaviors and diabetes outcomes,15 possibly due to distress and sleep behavior affecting inter-related biological pathways associated with diabetes, stress and sleep16 17 via self-regulation of health behaviors and perceptions of self and condition.18 19 Furthermore, the demands of regulating hemoglobin A1c (HbA1c) may disproportionately affect psychological well-being,20 with failure to sustain self-management behaviors leading to negative self-appraisals.21 It therefore appears clear that DRD, sleep and psychological well-being are mutually impactful in T2D. However, their specific inter-relationships require clarification.
Successful self-regulation allows individuals to set goals, engage in goal-related behaviors, evaluate progress and adjust behaviors or goals accordingly.10 11 Emotional regulation is consequently relevant to effective self-management of T2D. However, sustained emotional regulation in the stressful context of a long-term health condition carries increased risk of negative affect and self-appraisals, which in turn disrupt self-regulation.9 Such long-term emotional regulation can deplete capacity to self-regulate and use adaptive coping, undermining adherence to health-promoting behaviors and increasing risk of negative appraisals of oneself and health threats.11 22 This provides context for exploring potential influences of DRD on physical and emotional well-being in people with T2D.
Self-compassionSelf-compassion (the ability to approach personal failure and difficulties with kindness, acceptance and lack of judgment) may promote effective self-regulation and reduce condition-related distress.10–12 The commonly used Self-Compassion Scale (SCS)23 evaluates six constructs; the positively oriented constructs are ‘self-kindness’, ‘common humanity’ (seeing oneself in context of others’ experiences) and ‘mindfulness’ (non-judgmental awareness of one’s difficult feelings and thoughts in the moment).12 Cultivating these components mitigates impact of the negative constructs, ‘self-judgment’, ‘isolation’ (negative feelings regarding felt separation from others) and ‘overidentification’ (magnification of negative attention on the self). Pertinent to DRD, greater self-compassion is known to improve emotional regulation and self-regulation of goal-orientated behaviors,24 25 and a self-compassionate approach to health threats such as T2D can promote successful management and limit condition-related distress via adaptive strategies.10 11
Associations with sleepSelf-compassion is argued to directly and indirectly affect physiological pathways related to psychological stress and pathophysiology of T2D,19 and higher self-compassion has been linked with lower inflammatory marker levels (interleukin-6).26 Given the relationship between sleep and these physiological pathways,17 27 and that rising and sleeping later (evening chronotype) is associated with higher DRD,28 self-compassion may also play an important role in sleep behaviors. Research suggests that self-compassion is linked to reduced bedtime procrastination29 30 and better sleep quality,31–33 suggesting a potential role for self-compassion interventions around improving sleep.
RationaleWe know that suboptimal sleep behaviors may negatively affect psychological well-being and T2D outcomes.5 6 Cultivating self-compassion via diabetes management interventions improves outcomes and psychological well-being through its intrinsic regulatory function,21 34 and higher self-compassion is associated with better sleep quality.31–33 Here, we evaluate associations between self-compassion, sleep variables and DRD in people with T2D, hypothesizing that lower self-compassion is associated with higher DRD and poorer sleep quality.
Research design and methodsThe data presented here are a subset of the ‘Chronotype of Patients with Type 2 Diabetes and Effect on Glycaemic Control (CODEC)’ study.35 This study is registered with clinicaltrials.gov (NCT02973412).
Recruitment included primary and secondary care centers across four UK East Midlands sites (Leicester, Lincoln, Derby and Nottingham). Data were collected by clinical research staff via clinical interview, anthropometric and clinical data (ie, blood (venous) for biomarker and glycemic analysis) and self-report questionnaires. Participants in the current analysis attended between June 2017 and February 2019. All participant information was anonymized prior to inclusion in this dataset.
The CODEC study included 808 male and female adults (aged 18–75 years) prior to application of exclusion criteria (figure 1). Participants had an established T2D diagnosis (ie, >6 months since diagnosis), body mass index (BMI) of ≤45 kg/m2, HbA1c ≤10%, no sleep disorder diagnosis excluding obstructive sleep apnea (OSA), competency in English and willingness and ability to give informed consent to participate. Participants were all on a glucose-lowering therapy or lifestyle modification approach for T2D management. Exclusion criteria included terminal illness, weekly+ cannabis use or regular use of wakefulness-promoting agents, sedatives, melatonin or medications for nocturnal movement disorders. Further details on inclusion and exclusion criteria are detailed in the study by Brady et al.36
 Figure 1
Figure 1 Consolidated Standards of Reporting Trials flow diagram. *CODEC, Chronotype of Patients with Type 2 Diabetes and Effect on Glycaemic Control; HbA1c, hemoglobin A1c.
Data collectionDemographic dataAnthropometric (BMI) and demographic data (age, sex, ethnicity and year of diabetes onset) were collected by appropriately trained research staff. Social deprivation was determined by assigning an index of multiple deprivation (IMD) rank to the participant’s resident area based on their postcode. IMD scores are publicly available continuous measures of compound social and material deprivation linked to health outcomes.37
Diabetes Distress ScaleThe Diabetes Distress Scale (DDS)13 is a 17-item self-report DRD measure comprising four domains—emotional burden, physician-related distress, regimen-related distress and diabetes-related interpersonal distress. Individuals report severity of difficulties over the last month using a 6-point scale (1: ‘not a problem’; 6: ‘a very serious problem’). No items evaluated sleep difficulties. Item scores were averaged for an overall mean (range: 1–6), with higher values indicating greater distress. A consistent structure and good internal reliability and validity have been demonstrated,13 with Cronbach’s α evaluated at 0.89.34 Regarding criterion validity, the DDS has demonstrated associations with HbA1c, diabetes self-efficacy, diet and physical activity.38
Self-Compassion ScaleThe SCS23 is a self-report questionnaire measuring individual self-compassion. It comprises 26 statements rated on a 5-point scale (1: ‘almost never’; 5: ‘almost always’). Items form six subscales: three positive (self-kindness, common humanity, mindfulness) and three negative (self-judgment, isolation, overidentified), with an established bifactor model in which total and subscale scores provide equally effective explanations of outcome variance across international samples.39 The total score comprises the mean of subscale scores (range: 1–5), with negative items reverse-scored; consequently, higher scores indicate greater self-compassion (low: 1–2.5; moderate: 2.5–3.5; high: 3.5–5).12 Reliability in populations affected by diabetes is excellent (α=0.91).34
Epworth Sleepiness ScaleThe Epworth Sleepiness Scale (ESS)40 is a self-report questionnaire measuring daytime sleepiness via current dozing behavior rather than subjective sleepiness. Eight items are rated on a 4-point scale regarding likelihood of dozing while undertaking readily relatable daytime activities (0: ‘would never doze’; 3: ‘high chance of dozing’). These items are summed (range: 0–24). Higher scores relate to higher daytime sleepiness, with a ‘normal’ range of 0–10.
Objective sleep measuresParticipants wore a GENEActiv accelerometer device on their non-dominant wrist for up to eight consecutive 24-hour days. The device was fitted at the data collection clinic and participants were asked not to remove it until the end of the wear period, when they returned it in a prepaid envelope. The GENEActiv was initialized to collect data at 100 Hz and data uploaded using GENEActiv PC software V.3.2. Data were processed using R package GGIR V.1.8–1 (http://cran.r-project.org).41 Participants were excluded if their accelerometer files showed postcalibration error >0.01 g (10 mg), or <3 days’ valid wear (defined as >16 hours per day). Sleep duration was calculated using the automated sleep detection algorithm.42 Outputs included mean sleep duration (all days, weekday and weekend) and mean sleep midpoint (weekday and weekend). SJL was calculated by subtracting sleep midpoint for weekdays from weekends, following the study by Wittmann et al.7
AnalysisData were collated using Microsoft Excel before transfer into SPSS for Windows V.25 for analysis. The SCS was completed by 484 participants, 5 of whom were excluded due to missing DDS data. Hierarchical multiple regressions were used to determine the predictive value of sleep variables and self-compassion for DDS score. Age, sex, ethnicity, BMI, HbA1c, age of diabetes onset and IMD were added at step 1, sleep variables (ESS, sleep duration and SJL) at step 2 and self-compassion at step 3. Two models were generated, using either total SCS score or the six subscales at step 3, since both components explain similar variance in outcomes.39 Mediation analyses were completed using PROCESS V.4.0, model 4,43 with 95% bootstrap CIs (5000 sample).
For the regression analyses, power analysis using G*power indicated that 199 participants were required to detect a medium effect, given the maximum of 15 predictors in the most complex model (f2=0.15, α=0.05, power=0.95). For the mediation analysis, 107 participants per group were required to detect a medium effect (f2=0.15, α=0.05, power=0.95). Therefore, our sample size was adequate.
ResultsSample characteristicsFour hundred and sixty-seven participants with a T2D diagnosis and completed SCS data were included. For demographic variables, see table 1 and table 2. Most participants (89.5%; n=418) were overweight or living with obesity (BMI 25+). Most were below clinical threshold for DRD (DDS <2; 66.0%; n=308). Most (89.5%; n=418) reported moderate to high self-compassion (SCS mean score ≥2.5). Clinically relevant daytime sleepiness (ESS ≥11) affected 18.4% (n=86) of participants, and 53.1% (n=248) had suboptimal HbA1c (≥7.0; range: 5%–10%).
Table 1Sample characteristics (n=467)
Table 2Ethnic background frequencies (n=467)
Predictors of diabetes-related distressHierarchical regressions (table 3) were used to determine associations between self-compassion, sleep characteristics and DRD, controlling for demographic and condition-related variables. Variable tolerances (0.5–1.0) and variance inflation factors (1.0–2.0) did not contravene thresholds that would otherwise suggest unacceptable collinearity between independent variables.44
Table 3Regression model using SCS total score (step 3a) or subscales (3b), with Diabetes Distress Scale as outcome variable
At step 1, the set of control variables (age, sex, BMI, ethnicity, age of diabetes onset, HbA1c and IMD) significantly predicted DRD (F(7,344)=16.28, p<0.001; r2=0.25). Age had the largest influence on DRD (β=−0.28, p<0.001) with younger age predicting higher DRD. Higher HbA1c (β=0.27, p<0.001) and higher BMI predicted higher DRD (β=0.13, p=0.011). Finally, ethnicity predicted DRD (β=−0.15, p=0.003). Follow-up one-way analysis of variance indicated through Bonferroni post hoc comparisons that significant differences lay between (1) people of Indian ethnicity, who reported 0.63 points greater DRD than white British people and (2) people reporting a mixed white and Asian background, who had 2.26 points greater DRD than white British participants and 2.42 points greater than people from an other white background (p<0.05 for all). Sex, age of onset and IMD did not predict DRD (p>0.05).
Step 2 incorporated sleep variables (sleep duration, ESS and SJL) (F(10,341)=16.35, p<0.001; r2=0.32). Age (β=−0.29, p<0.001), HbA1c (β=0.26, p<0.001) and ethnicity (β=−0.18, p<0.001) remained significant predictors, while BMI no longer significantly predicted DRD (p=0.079). Daytime sleepiness was the only sleep variable predicting significant additional variance in DRD (β=0.28, p<0.001), with greater sleepiness associated with greater distress. SJL and sleep duration did not predict DRD (p>0.05).
Step 3 comprised inclusion of overall SCS score (F(11,340)=20.43, p<0.001; r2=0.40). Greater overall SCS score predicted lower distress DRD (β=−0.30, p<0.001). Age (β=−0.23, p<0.001), HbA1c (β=0.21, p<0.001), ethnicity (β=−0.17, p=<0.001) and daytime sleepiness (β=0.21, p<0.001) remained significant predictors.
When the six self-compassion subscales were substituted for overall SCS score at step 3, the model still significantly predicted DRD (F(16,335)=20.58, p<0.001) and explained greater variance (r2=0.50). Age (β=−0.18, p=0.002), ethnicity (β=−0.14, p=0.001), HbA1c (β=0.15, p=<0.001) and daytime sleepiness (β=0.16, p<0.001) remained significant predictors, with lower impact than at step 3 for the overall SCS model. In addition, IMD was a significant predictor of DRD in this model, with lower IMD predicting higher distress (β=−0.09, p.039). The three positive SCS subscales did not significantly predict DRD, nor did self-judgment (p>0.05). However, higher isolation (β=0.15, p=0.030) and overidentified (β=0.27, p<0.001) scores predicted higher DRD.
MediationWe generated seven mediation models using the PROCESS V.4.0 macro43 for SPSS for Windows 28, with 95% CIs and 5000 bootstrap samples, examining direct and indirect (mediated by ESS scores) effects on DRD of SCS total and subscales. Findings are detailed in online supplemental table S1 and depicted for significant relationships in figure 2. We identified positive direct and indirect effects for the self-judgment, isolation and overidentified subscales. Total SCS score had negative direct and indirect effects on DRD. Self-kindness and mindfulness had neither a direct or indirect effect on DRD, and common humanity only had a direct positive path (no indirect effect).
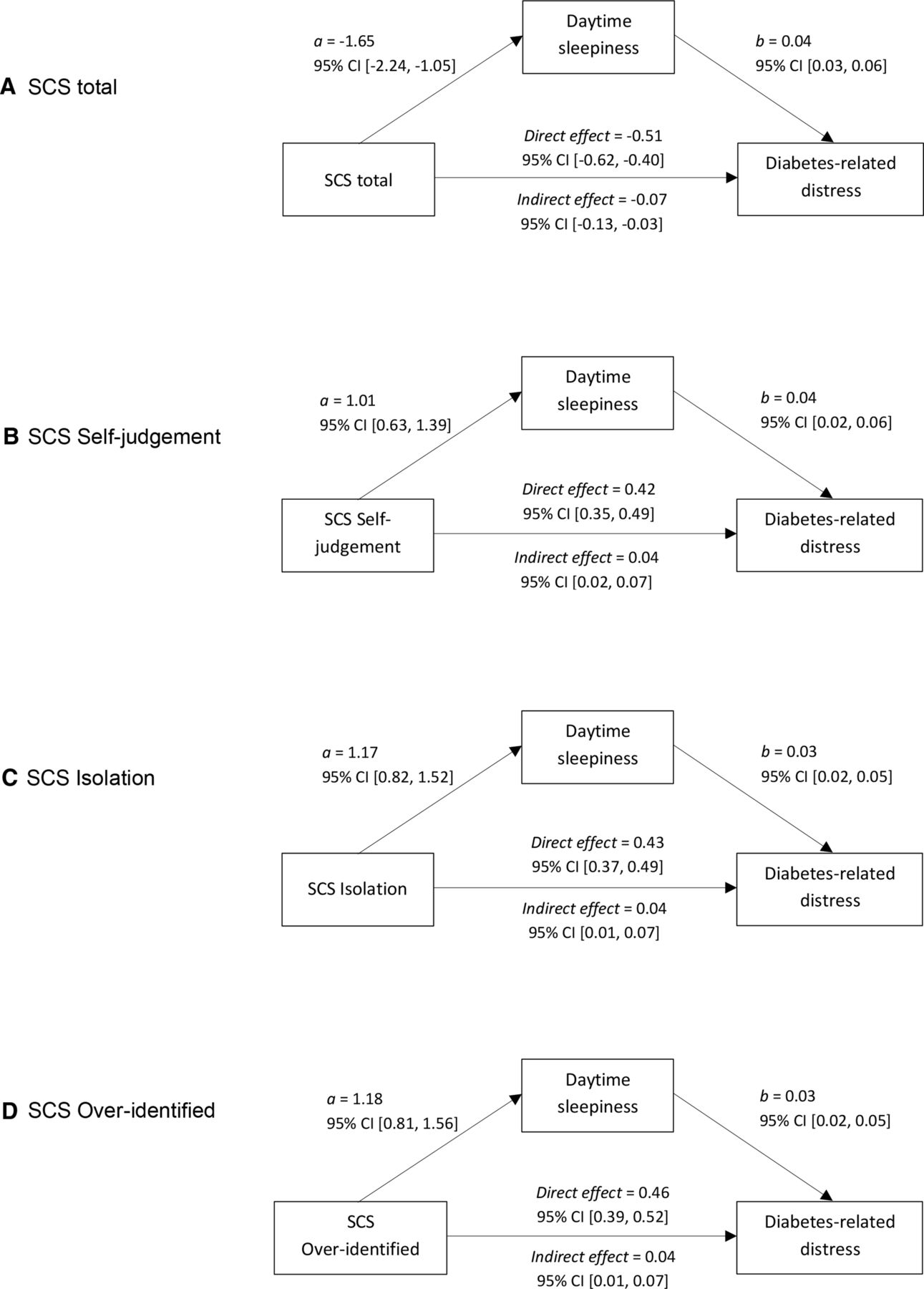 Figure 2
Figure 2 Mediation models for direct and daytime sleepiness-mediated effect on diabetes-related distress of (A) SCS total; (B) SCS self-judgment; (C) SCS isolation; (D) SCS overidentified. SCS, Self-Compassion Scale.
All analyses were recompleted with individuals with OSA excluded (n=33) to confirm that this diagnosis did not significantly affect outcomes. No differences were found, except that BMI remained a significant predictor of DRD at step 2 of both models (β=0.11, p=0.03 for both).
DiscussionThis cross-sectional, multivariable analysis examined associations between DRD, sleep behaviors and self-compassion among people with T2D using multiple regression and mediation analyses. Demographic variables (age, sex, ethnicity, BMI, HbA1c and age of onset) were controlled for, to parse out influences of sleep variables and self-compassion.
Self-compassion and DRDIn the regression model incorporating mean SCS score, overall self-compassion explained the most DRD variance (followed by age and daytime sleepiness, then HbA1c and ethnicity). The relationship was inverse; higher self-compassion predicted lower DRD. In the subscales model, only the overidentified and isolation negative subscales predicted DRD. Overidentified was the stronger predictor, but both positively predicted distress. This suggests that higher distress is reported by individuals who fixate on negative situations affecting them with less clarity and balance, and perceive difficulties in sensed separation from others.
The subscales model explained substantially more variance than the total SCS model, potentially attributable to a masking effect of the other subscales in the latter, reducing the impact of overidentified and isolation. Consequently, despite prior research arguing for equal effectiveness of the full score and subscales in describing self-compassion,39 the subscales appear valuable for highlighting specific difficulties in this population.
Increased self-compassion predicting lower DRD resonates with past research showing that self-compassionate approaches to health threats can improve condition management, support emotional self-regulation and help control condition-related distress.10 11 17 24 25 Another study found that DRD decreased as self-compassion increased following a mindful self-compassion programme for people with diabetes types 1 and 2.34 Our study extends former findings by identifying significant associations between two negative SCS subscales and DRD in people with T2D. This may open up new therapeutic avenues for addressing specific self-compassion deficits, and reducing DRD.
Influence of sleep variablesIn the total and subscale regressions, greater daytime sleepiness predicted higher DRD. Mediation analyses indicated that the association between SCS total and negative subscales on DRD was partially mediated by daytime sleepiness. Lower total SCS and higher negative subscale scores were associated with higher daytime sleepiness and higher DRD (there was also a direct association between SCS variables and DRD). Sleep could therefore comprise one route by which self-compassion influences distress in people with T2D, possibly by increasing engagement in good self-care behaviors around sleep. Our results concur with previous findings that sleep quality partially mediates relationships between depression and anxiety symptoms and diabetes-related quality of life.5 They also highlight the potential importance of self-compassion in management of sleep-related well-being, recommending the consideration of inter-relations between these factors when developing DRD interventions.
Neither SJL nor sleep duration predicted DRD, contradicting previous findings identifying an association between DRD and sleep duration.6 However, that study examined no other sleep variables, so their analysis may have neglected to disambiguate sleep-related factors related to well-being (including daytime sleepiness). The authors also included a daytime nap (30–120 min) alongside night-time sleep when measuring sleep duration, which may distinguish their sample in China from our UK-based sample.
Clinical implicationsThis study establishes key relationships between self-compassion, sleep quality and DRD, although direction of causation is so far undetermined. The importance of the overidentified and isolation subscales suggests that fixation and obsession around negative events, plus distress associated with sensed separation from others, may affect how people experience T2D. Our results also correspond to findings that daytime sleepiness negatively predicts self-care in people with T2D.45 Consequently, third-wave therapies focusing on cognitive defusion and increasing self-compassion may be particularly valuable in T2D populations. Appropriate interventions might include therapies focused on positive self-appraisal and reducing self-criticism, such as compassion-focused therapy,46 or acceptance and commitment therapy (ACT), which aims to increase psychological flexibility and acceptance of difficulty.47 Studies have already shown improved psychological flexibility, reduced stress and low mood and better psychological well-being following ACT with people with diabetes,48 49 and reduction in emotional distress in a randomized controlled trial of elderly people with T2D.50 Friis et al34 further demonstrated in a small trial that a mindful self-compassion group for people with diabetes types 1 and 2 increased self-compassion and decreased DRD, providing evidence for self-compassion as a modifiable treatment target.34 However, a trial in a larger T2D cohort is required, and will help to quantify any causative relationship between self-compassion and DRD (which will be crucial to determine clinical implications of the associations we have identified). Group interventions may also be viable, potentially reducing the social isolation associated with T2D.51
Our findings corroborate previous work suggesting that optimizing sleep behaviors may improve T2D outcomes.2 3 5 6 We found that higher daytime sleepiness was associated with higher DRD, with an important mediating role for daytime sleepiness in predicting distress. Therefore, assessment of individuals with T2D should include consideration of sleep behaviors, particularly daytime sleepiness and self-care around sleep. Educational interventions alongside therapeutic approaches might include provision of sleep hygiene information alongside traditional management strategies, as a potential preventative strategy to reduce long-term psychological impact of T2D.
A further finding was that IMD significantly predicted DRD in the model using the six SCS subscales. IMD is a relative measure of deprivation specific to a small locality, based on deprivation around employment, income, education, skills, training, health, crime, housing and services and living environment.37 Our finding that lower IMD predicted higher distress is consonant with other research showing impacts of deprivation on mental well-being (eg, see the recent large dataset analysis and review of the literature by Qi et al, showing contributions of IMD to risk of depression and anxiety).52
Finally, our identification of greater DRD in younger people and in particular ethnic groups suggests that assessments and interventions targeting mental well-being, self-compassion and sleep in these groups may be important. For example, people self-reporting an Indian or mixed white and Asian background had higher DRD than people reporting a white background. Ethnicity may therefore influence experiences of T2D, and people from some groups may require additional support in adjusting to and managing their condition. This is an understudied area and should be prioritized. Exploring possible interactions between effects relating to ethnicity and socioeconomic status is also critical, since while both variables significantly explained a proportion of the variance (IMD only for the six subscales model, and ethnicity across both models), people from ethnic minority backgrounds are likely to be more socioeconomically vulnerable and these variables are commonly and easily confounded.53
LimitationsTwo key limitations must be noted. First, this cross-sectional study design (common within mediation research) does not enable identification of causation, only association. As such, it is unknown whether low self-compassion causes, is caused by, or is inter-related with DRD. We prepared our models based on experimental and correlational findings indicating that increased self-compassion has positive impacts on well-being,24 25 54 55 and following recent relevant research into self-compassion in type 1 diabetes which also used mediational analyses in a similar way.56 Nevertheless, this latter study acknowledged limitations in applying this methodology, and the same limitations apply here. Importantly, mediation analysis traditionally requires a known time ordering between exposure, mediator and outcome (although this is not always possible and can be substituted for incorporation of information from prior research around ordering of variables, as we have done).57 It is important to acknowledge this departure from the assumptions of the methodology, and to fully recognize that our findings only lend weight to hypothesized and partially evidenced relationships between self-compassion and DRD rather than confirming their existence. Additionally, meditation requires a lack of potential confounding variables, including to estimate the indirect effect, and it is crucial to highlight the possibility of confounds in this case which may contribute to the identified associations. Consequently, a crucial recommendation for future research comprises longitudinal or pre-post intervention analyses to test the proposed associations over time, and determine the direction of causation.
Second, the self-reported ESS could be confounded by psychosocial variables affecting experience of daytime sleepiness such as attention, motivation, quality of life and emotional regulation, potentially arising from comorbid conditions, which may relate more to self-compassion and DRD than objective sleep processes. Finally, there was a high proportion of retirees in our sample (57.6%). Daytime sleepiness may be less common within retired populations due to reduced social influence on sleep patterns, potentially reducing any role of SJL. We must also acknowledge the bias towards people reporting a white British background (84%), reducing generalizability of findings to other populations—as noted above, further exploration of the role of ethnicity (and socioeconomic status) in diabetes-related well-being will be important.
Future researchThese data contribute to growing evidence for self-compassionate approaches and targeted sleep interventions in psychological management of T2D. Future work might take longitudinal and interventional approaches to assessing causality and long-term impacts of self-compassion and sleep behaviors on DRD. Considering variables not included here, including chronotype and comorbidities, may illuminate additional contributors to DRD and further inform development of multifaceted self-compassion and sleep interventions. Qualitative studies would be also valuable to assess beliefs and behaviors around sleep and self-compassion in people with T2D. As noted, evaluation of sleep, self-compassion and DRD across age groups and in different ethnic/cultural groups is also essential.
留言 (0)