
記住我








Insomnia is very common in the population, which is characterized by difficulty starting or maintaining sleep, along with symptoms such as irritability or fatigue when awake (1). Adequate sleep is very important for human health, affecting people's work and life, while insomnia will seriously affect our daily life. Insomnia is defined in the fifth edition of the Diagnostic and statistical manual of mental disorders (DSM-5) as difficulty getting to sleep, staying asleep, or having non-restorative sleep despite having the adequate opportunity for sleep, together with associated impairment of daytime functioning, with symptoms being present for at least 4 weeks (2). Around the world, 15–30% of adults and 10% of adolescents suffer from some form of insomnia (3, 4). Insomnia has a great impact on the human body (1, 5, 6), first of all, insomnia will make the human immune decline, weakened resistance to various diseases. Long-term insomnia can cause high blood pressure, heart disease, high blood fat, senile dementia, and so on. Secondly, patients with long-term insomnia are easy to cause negative effects in mental aspects, such as inattention, decreased thinking ability, anxiety, depression, mental tension and other emotions, cerebral cortex dysfunction, causing plant neurological dysfunction, serious forms of psychosis, neurosis, and so on.
At present, the treatment methods for insomnia mainly include drug therapy (7), cognitive behavioral therapy (8), exercise therapy (9), mindfulness meditation (10), and traditional Chinese acupuncture therapy (11), etc. But these treatments have some limitations, no matter western medicine or Traditional Chinese medicine, the current treatment of insomnia is mainly drugs, but drugs have addictions, adverse reactions, or unstable compatibility, there are individual differences in curative effect (12) and the use of drugs like doxepin, ramelteon, and secobarbital is increasingly being discouraged due to their potential toxicity. According to the European insomnia guidelines, cognitive-behavioral therapy, which usually consists of sleep hygiene, relaxation training, sleep restriction therapy, and cognitive therapy, is the most studied non-pharmacologic treatment (13). However, it requires frequent monitoring and high maintenance costs (9). Acupuncture may be beneficial for insomnia, but it is invasive (14). Therefore, we need to find more effective, simple, and safe non-invasive treatments.
Studies have shown that Taijiquan, as a new intervention, has a good effect on insomnia. Irwin et al. (15) observed 112 healthy elderly people aged 59–86 who were randomly assigned to the Taijiquan group and the health education group, among adults with moderate sleep complaints, Taijiquan can be considered a useful non-pharmaco-logic approach to improve sleep quality in them. Siu et al. (16) studied the effect of Taijiquan or exercise on sleep of the elderly with insomnia and found that compared with the control group, the sleep efficiency of the taijiquan group was improved. However, evidence-based research remains insufficient in this area, and analysis of the efficacy of insomnia caused by different diseases is lacking. There has been no systematic review of the efficacy of various forms of Tai chi compared with different exercise interventions.
Therefore, we sought to summarize existing high-quality studies on Taijiquan intervention for insomnia, and overcome the limitations of the previous Meta-analysis, to seek a higher level of evidence-based medical evidence.
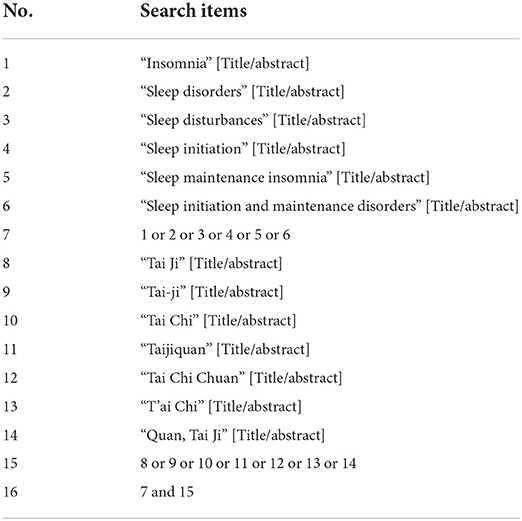
Materials and methods Search strategy and selection criteria Search strategyWe conducted a comprehensive search for all published and unpublished RCTs of Taijiquan for patients with insomnia or other diseases with sleep complaints, in both Chinese and English language. We searched four English databases—Pubmed, Embase, Cochrane library, Web of Science, and four Chinese databases—CNKI, CBM, VIP, and Wanfang Data, from their inception to October 20, 2021. The search strategy is outlined in Appendix 1. Using the Pubmed database as an example, the search strategy was as follows (Table 1). In addition, efforts were made to find other literature sources, such as references from all included studies and clinical trial registries, which were also searched for additional relevant studies. If the original text or relevant data is not available, we will contact the original author for more information.
TABLE 1
Table 1. The specific search strategy of the Pubmed database.
The inclusion criteria are presented as follows1) Randomized and controlled design
2) Sample size ≥30
3) Duration of intervention ≥1 week
4) Use a suitable control intervention (non-active placebo or established positive control, e.g., benzodiazepine)
5) Have measurable results for sleep, any form of scale, or objective electrophysiological indicators
6) Any form of Taijiquan
7) Full text available and can get enough data.
Exclusion criteriaWe excluded duplicate reports, reviews, conference abstracts and letters, trials enrolling patients with non-related subject research, and data that were incomplete or not obtainable. In addition, after the researchers reviewed the full text and discussed for many times, the articles identified as having serious quality defects, such as data confusion, and the articles with obvious flaws in the study design were also excluded.
Data extraction and outcome measuresThe two authors (DMH and ZCL) independently searched and screened the retrieved literature. Unqualified trials were excluded, and the differences were resolved through discussion between the two authors. For problems that cannot be solved through discussion, consult the third author (YH) jointly to assess whether the trials met the inclusion criteria.
Some baseline information is extracted from the original studies, and they include the first author and published year, sample of patients, age, sex, outcome, intervention, frequency in two groups, and follow-up period. Data are extracted independently by two investigators (DMH and ZCL), and discrepancies are resolved by consensus. We have contacted the corresponding author to obtain the data when necessary. The primary outcome is Pittsburgh Sleep Quality Index (PSQI), PSQI is the most widely used sleep assessment tool with good reliability and validity (17, 18). It has been translated and used in many countries and can accurately reflect the sleep status of patients (19).
Assessment of risk of bias in included studiesTwo review authors (DMH and ZCL) independently evaluated the risk of bias for each study according to the Cochrane Handbook for Systematic Reviews of Interventions. Disagreements were resolved by discussion or by consultation with a third reviewer (YH), when necessary. The following domains were assessed: sequence generation, allocation concealment, blinding of participants, providers and outcome assessors, completeness of outcome data, selective outcome reporting, and other sources of bias. Each potential source of bias was classified as either high, low, or unclear.
Statistical analysisReview Manager (RevMan) version 5.3 software was used for the meta-analysis. Since this meta-analysis included only continuous data, we used the mean difference (MD) and 95% confidence interval (CI) for analysis. If the data was not available in the article, and the authors could not be contacted, estimates were made using the known data and the formula in the Cochrane Handbook for Systematic Reviews of Interventions. The I2 statistic was used to evaluate the heterogeneity revealed by data analysis. The interpretation of the I2 statistic is as follow (Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1.2008):
• 10–40%: might not be important
• 30–60%: may represent moderate heterogeneity
• 50–90%: may represent substantial heterogeneity
• 75–100%: considerable heterogeneity.
If substantial heterogeneity (above 50%) was detected, a random-effects model was used in the meta-analysis, where appropriate, subgroup or sensitivity analyses were performed to explore the source of heterogeneity.
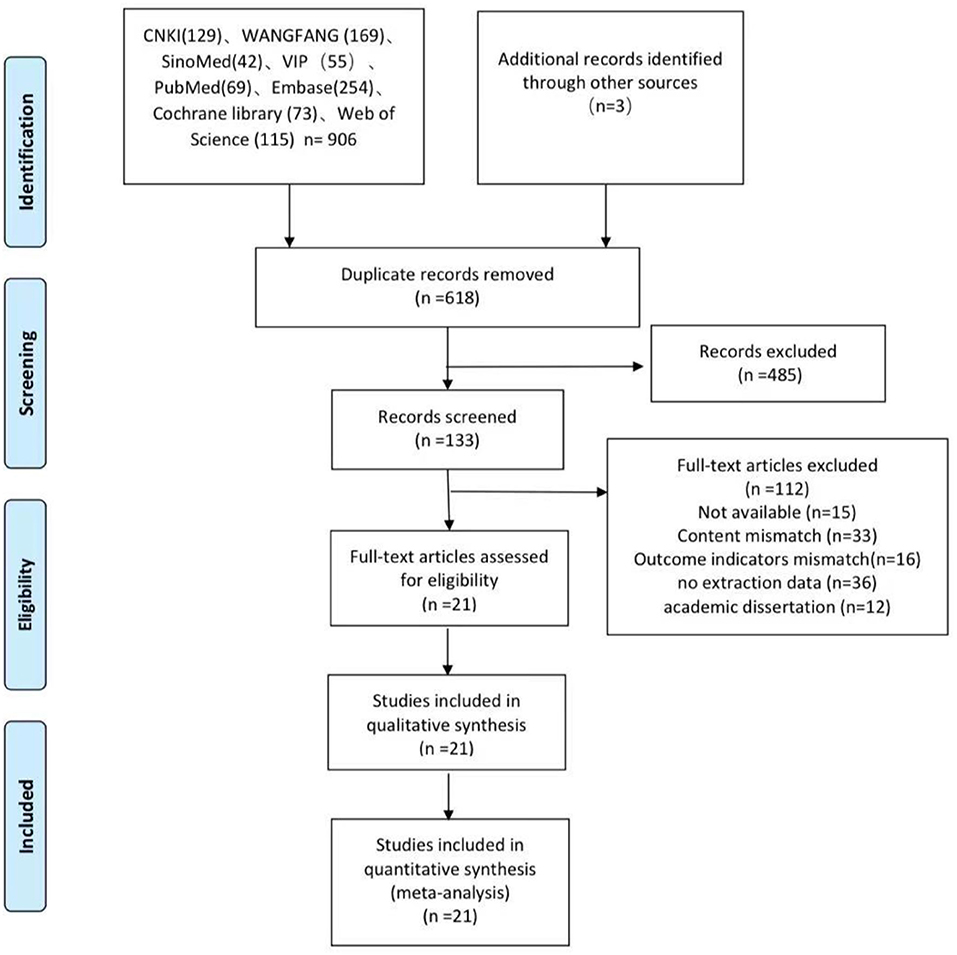
Results Search resultsThe review searched literature from eight databases. Figure 1 shows the search and selection process. A total of 909 potentially relevant articles were searched for strategies. After removing the duplicates, 618 articles need to be abstracted. 485 were excluded from titles and summaries, leaving 133 requiring full text. After reading the full text of these articles, were excluded, mainly because of inadequate study design, inadequate interventions, or incomplete data. The qualitative analysis included 21 studies (15, 16, 20–38).
FIGURE 1
Figure 1. Flowchart of the study search and selection process.
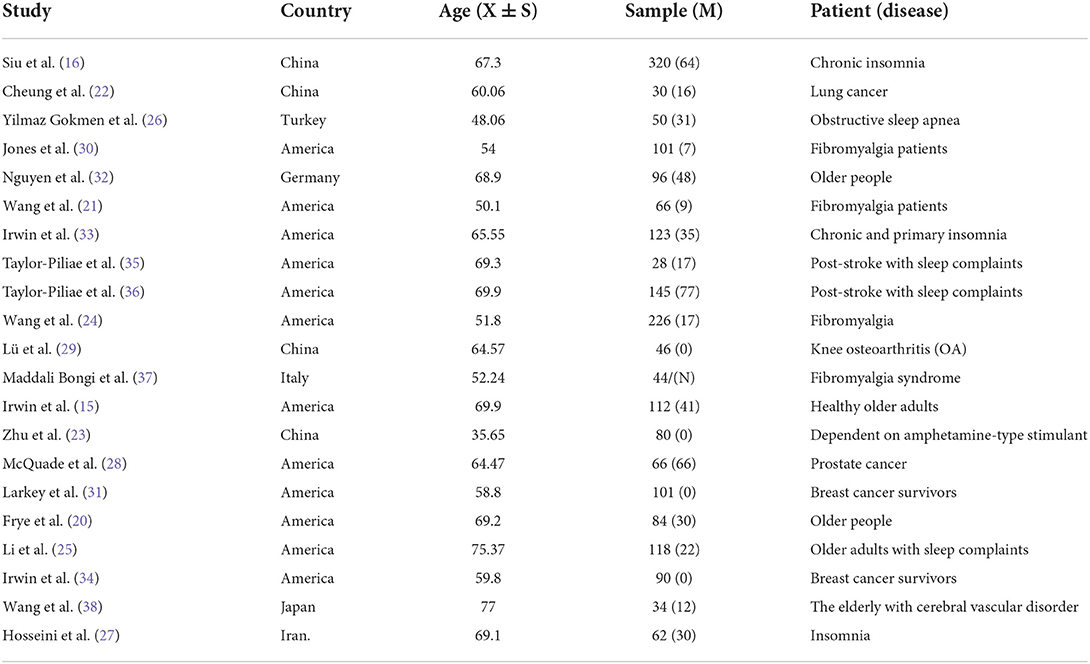
Characteristics of included studiesThe study included 21 articles from seven countries—four from China, 12 from the United States, one from Iran, one from Italy, one from Turkey, one from Japan, and one from Germany. Their characteristics are presented in Table 2. In all of the studies, the mean total PSQI score at baseline was ≥5. This is consistent with insomnia diagnosis. In addition to insomnia, some patients also had other diseases such as depression, prostate cancer, knee osteoarthritis, fibromyalgia, post-stroke, or breast cancer. A total of 2,022 patients were included in this meta-analysis, of which 907 were allocated to the Taijiquan group and 1,115 were allocated to the control group. The average age of patients is over 35. One article (37) did not describe gender, and there were 522 male patients and 1,456 female patients in the retained literature (Table 2).
TABLE 2
Table 2. Basic information included in the study.
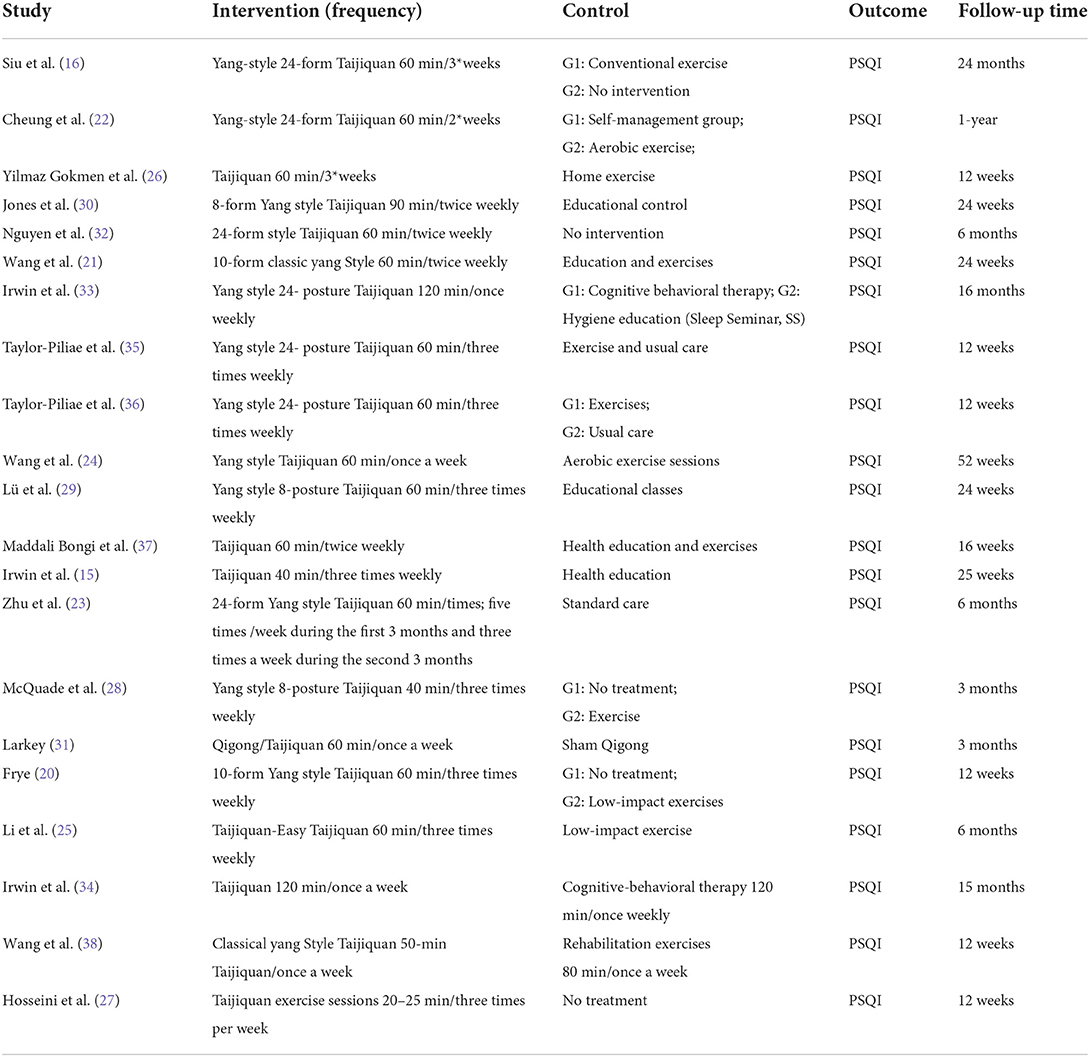
For the interventions, 15 articles trace back or describe in detail the types of taijiquan. eight studies used 24 forms of Yang's Taijiquan, and four studies used 8-form Yang style Taijiquan. Three studies used 10-form Yang style Taijiquan. Taijiquan lasts for a minimum of 12 weeks and a maximum of 24 months. Most are 3–6 months. The frequency of Taijiquan varies from 1 to 5 times per week (Table 3).
TABLE 3
Table 3. Basic information included in the study.
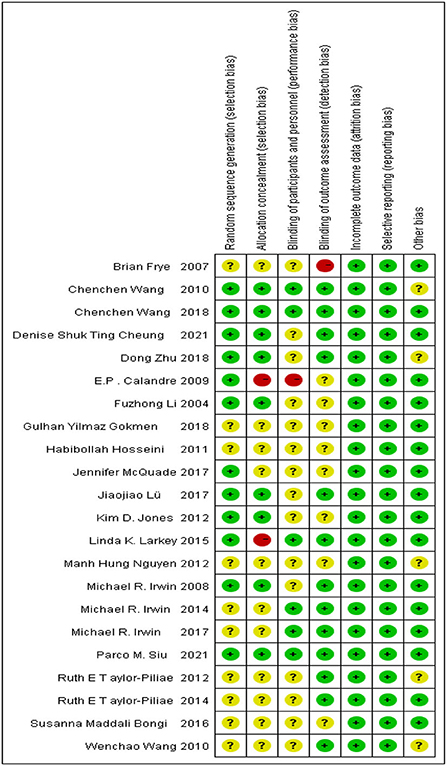
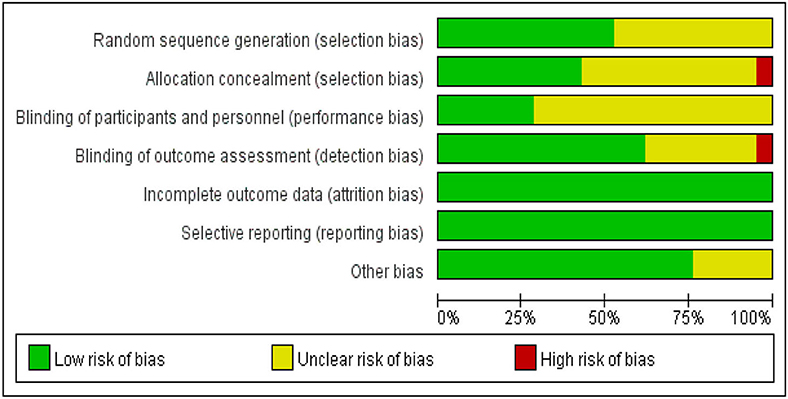
Risk of bias in the included studiesAccording to the Cochrane Handbook for Systematic Reviews of Interventions, we assessed the risk of bias in the included literature. The results are shown in Figures 2, 3. 12 RCTs described the appropriate random sequence generation method in detail. The other eight studies did not report the random sequence generation. Thus, the risk for these domains was determined to be unclear. Only nine of the studies reported using allocation concealment. Only 13 reported blinding the assessors. Due to the nature of Taijiquan, strict blinding of participants was difficult. All of the included studies reported the complete outcome data, and we considered them to be low-risk for this item. Most studies reported all of the outcomes. No other significant bias was found in any of the studies.
FIGURE 2
Figure 2. Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
FIGURE 3
Figure 3. Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
Meta-analysis resultsAccording to our retrieval results and the characteristics of the included studies, most of the studies used PSQI as the outcome indicator, while other outcome indicators could not be meta-analyzed due to the lack of a sufficient number of studies.
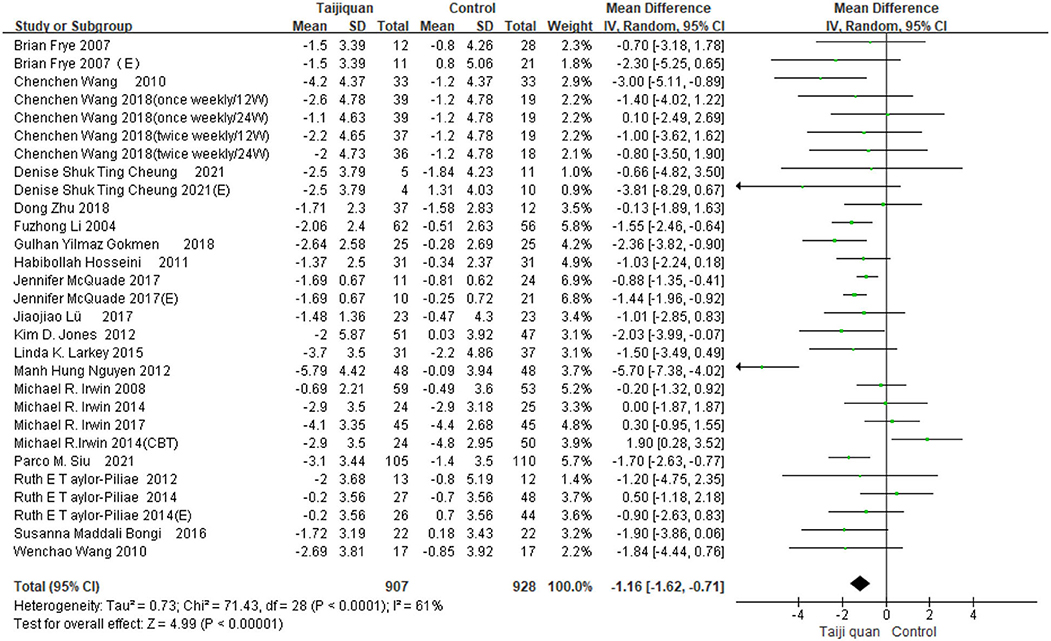
Our meta results suggest that Taijiquan is beneficial to insomnia patients and can significantly improve PSQI [MD = −1.16, 95% CI (−1.62, −0.71), P < 0.00001] (Figure 4). However, we found high heterogeneity of meta [I2 = 61%, P < 0.0001] (Figure 4), Further subgroup analysis is required to identify the source of heterogeneity.
FIGURE 4
Figure 4. Forest plot for PSQI meta-analysis was performed on all included studies.
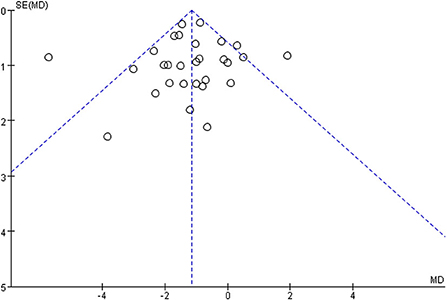
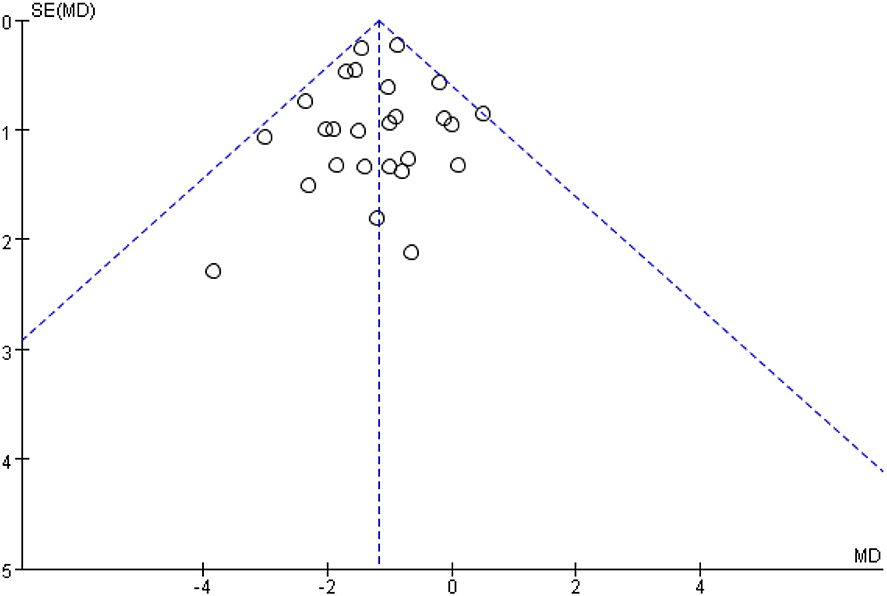
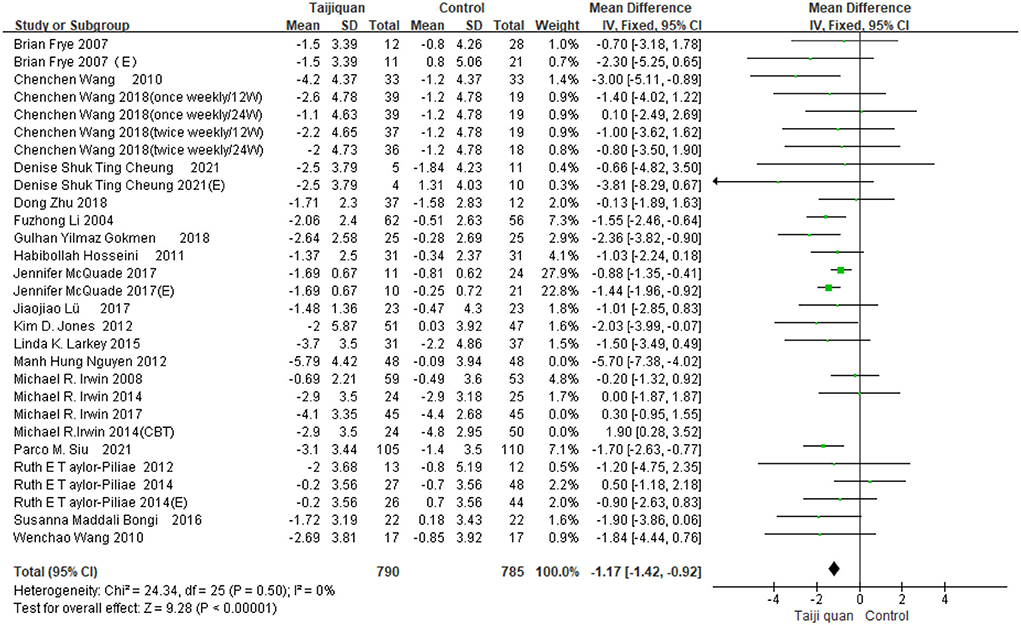
Figure 5 shows that the funnel diagram is symmetric, But there are three studies in the funnel outside, We use sensitivity analysis to determine that three studies with both large heterogeneity and publication bias from Irwin et al. (33, 34) studies and Nguyen et al. (32) study. After removing the three articles with publication bias, the Funnel plot is symmetric (Figure 6) and the combined results of the meta-analysis were stable [MD = −1.17, 95% CI (−1.42, −0.92), P < 0.00001] and the heterogeneity is small [I2 = 0, P = 0.05] (Figure 7).
FIGURE 5
Figure 5. The publication bias of all studies was determined by funnel plot.
FIGURE 6
Figure 6. After removing three studies, the symmetrical funnel plot was obtained.
FIGURE 7
Figure 7. After deleting three studies, the PSQI forest plot of the remaining studies.
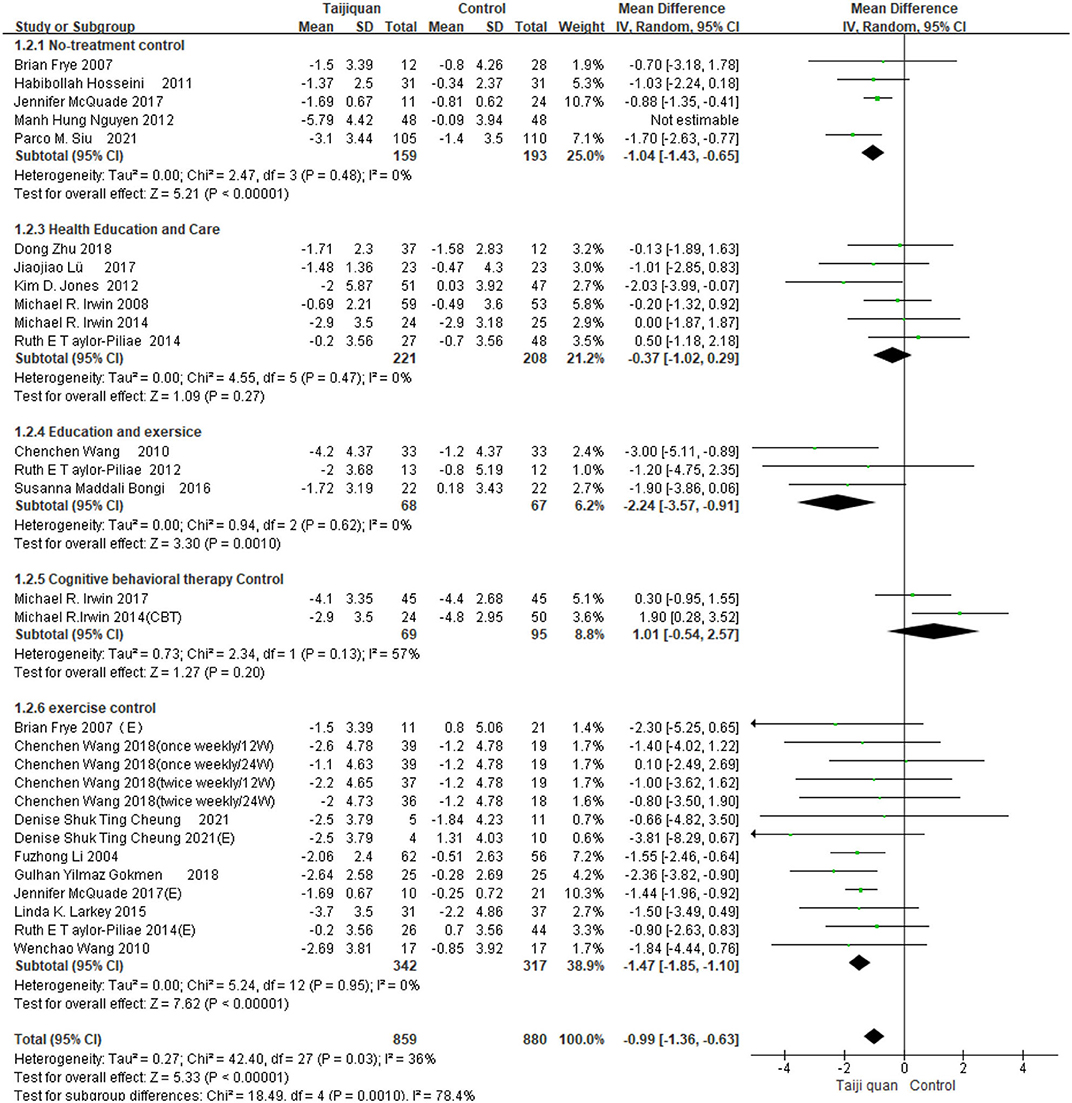
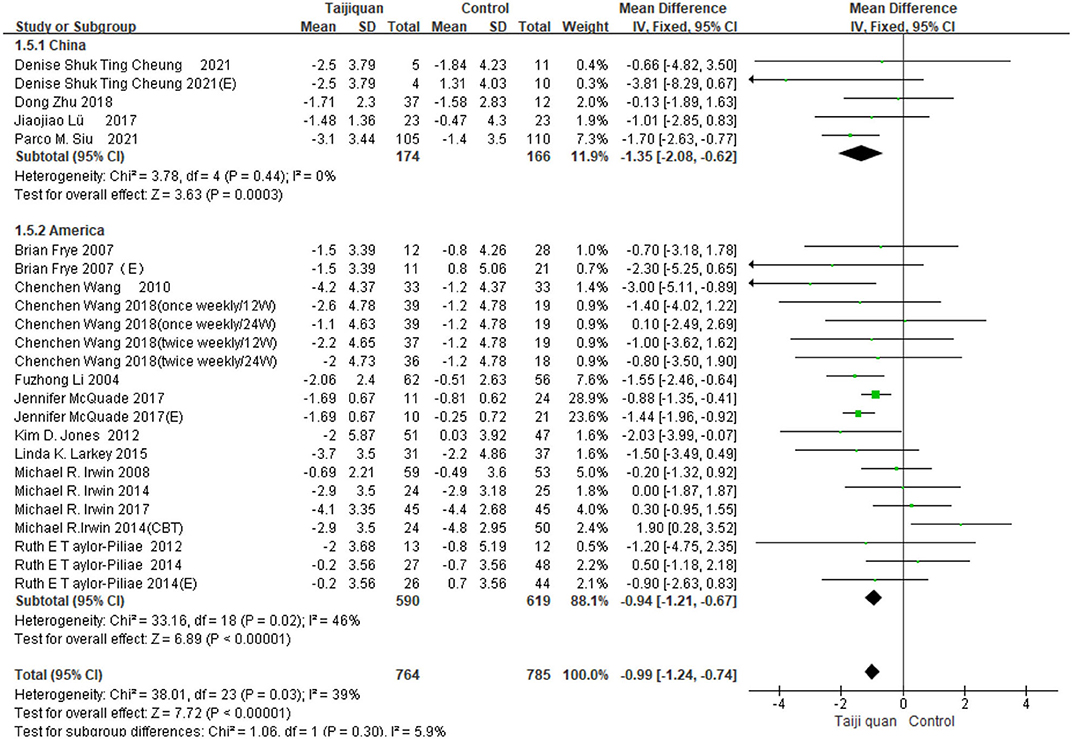
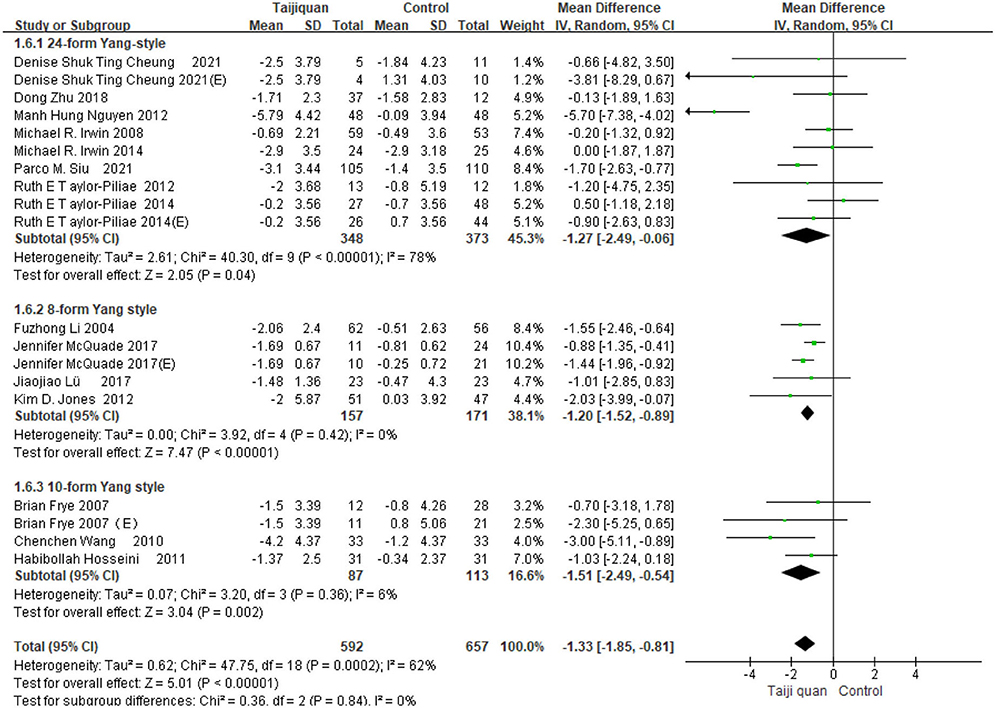
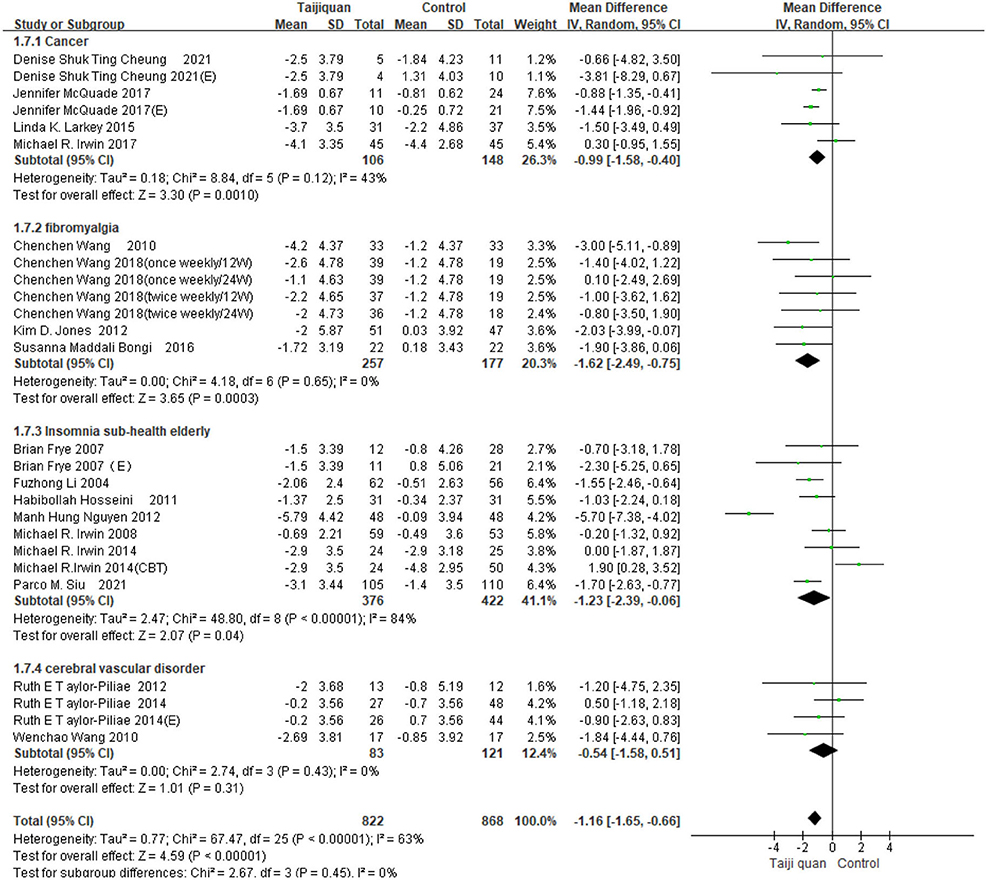
Subgroup analysisFive studies showed the effect of Taijiquan on global PSQI scores compared with non-treatment groups. Results of our meta-analysis showed that Taijiquan significantly reduced PSQI scores [MD = −1.95, 95% CI (−3.31, −0.59), P = 0.005], and a significant heterogeneity (I2 = 87%, P < 0.00001). When the Nguyen et al. (32) study was excluded, the heterogeneity of the overall PSQI score decreased to 0 (I2 = 0%, P = 0.48), and the meta-analysis still showed a stable, significant effect [MD = −1.04, 95% CI (−1.43, −0.65), P < 0.00001] (Figure 8, 1.2.1). Compared with simple exercise control group, Taijiquan has significant difference [MD = −1.47, 95% CI (−1.85, −1.10), P < 0.00001] (Figure 8, 1.2.6); When health education was combined with exercise as a control group, Taijiquan continued to significantly improve sleep [MD = −2.24, 95% CI (−3.57, −0.91), P = 0.0010] (Figure 8, 1.2.4). In addition, our subgroup analysis also found that compared with simple health education, both Taijiquan and health education or usual care could significantly reduce PSQI scores, but there was no significant difference between them [MD = −0.37, 95% CI (−1.02, 0.29), P = 0.27] (Figure 8, 1.2.3). Both cognitive behavioral therapy and Taijiquan can significantly reduce PSQI scores, but there is no significant difference between the two in improving insomnia [MD = 1.01, 95% CI (−0.54, 2.57), P = 0.20] (Figure 8, 1.2.5). There was no significant difference between studies in China and the United States, and Taijiquan was equally effective for Americans and Chinese (P = 0.30, Figure 9). Current studies mainly focus on Yang's Taijiquan, and different forms of Taijiquan have no significant difference in improving PSQI (P = 0.76, Figure 10); Through subgroup analysis of different patients, we found that Taijiquan significantly improved cancer, fibromyalgia, and insomnia of normal elderly people, while there seemed to be no significant difference in patients with cerebrovascular diseases (P = 0.31, Figure 11).
FIGURE 8
Figure 8. Subgroups of different control groups analyzed forest plot.
FIGURE 9
Figure 9. Subgroups of different countries analyzed forest plot.
FIGURE 10
Figure 10. Subgroups of different forms of Taijiquan analyzed forest plot.
FIGURE 11
Figure 11. Subgroups of different patients analyzed forest plot.
DiscussionIn this systematic review and meta-analysis, we identified 21 RCTs of 2022 individuals from seven countries. Overall, taijiquan has a better effect on insomnia improvement compared with exercise and health education alone, and subgroup analyses found that tai chi was as effective as cognitive behavioral therapy in improving insomnia. In terms of different diseases, we found that Taijiquan significantly improved cancer, fibromyalgia, and insomnia in normal elderly people, while there seemed to be no significant difference in patients with cerebrovascular disease. Compared with other studies, Taijiquan was equally effective for Americans and Chinese. There are no influences that have a significant effect on Asians. This systematic evaluation includes all the studies on Taijiquan intervention for insomnia in both Chinese and English, and the research objects include both healthy people and various patients, the old and the young, which is a relatively complete systematic evaluation of Taijiquan intervention for insomnia. Additionally, since no adverse events were reported, Taijiquan could be promoted as a safe intervention for improving sleep quality.
Insomnia is a common problem, with about a quarter of adults suffering from insomnia. Body and mind exercise is a hot topic in the intervention treatment of insomnia. Taijiquan was gradually formed in the late Ming and early Qing Dynasties. It is a centuries-old martial art that combines physical movement and relaxation and is a traditional Chinese sport that has spread worldwide in recent years, more than five million people practice Tai Chi in the US alone (39). At present, Tai Chi has been widely used in the intervention of various diseases, including the rehabilitation of motor function after stroke (40), Parkinson's disease (41), atherosclerosis (42), diabetic foot (43), and so on. The first research on the intervention of taijiquan in insomnia occurred in 2002 when Lu et al. (44) found that taijiquan could improve the sleep of cancer patients. So why does taijiquan affect people's sleep?
The exact biological mechanism of Taijiquan in treating insomnia is not clear, Compared to simple exercise training, current hypotheses suggest that Taijiquan may improve sleep outcomes by reducing sympathetic activity and stimulating the parasympathetic nervous system, restoring the homeostasis balance of sympathetic/parasympathetic function (45). As a low-intensity aerobic exercise, Taijiquan may also encourage the brain to induce normal sleep by inhibiting the non-5-HT spinal system or improving the plasma concentration of pro-inflammatory cytokines to prevent insomnia (46, 47). In addition, studies have shown that Tai Chi can enhance functional connections in the brain (48). It can cause a change in the central nervous medium, thus improving people's sleep conditions and treating insomnia symptoms (46). Studies have shown that chronic insomniacs have reduced hippocampal volume and orbitofrontal gray matter concentration and increased anterior cingulate rostral cortex volume compared to non-insomniacs (15, 49, 50). Taijiquan may improve insomnia by inducing changes in hippocampal volume and orbitofrontal gray matter concentration (51, 52). Changes in brain regions associated with insomnia have been observed in Taijiquan trained individuals. Decreased anterior cingulate cortex homogeneity was observed in patients with long-term Taijiquan use (53). Long-term Taijiquan exercise can slow down gray matter atrophy and this can decrease sympathetic activity (54, 55). In addition, Taijiquan significantly increased functional connectivity between the medial prefrontal cortex and the medial temporal lobe in insomniacs (56). Taijiquan can improve emotional stability and, to some extent, improve sleep quality. The Chinese believe that taijiquan exercises emphasize the leading role of consciousness of “mind first behind body” and pay attention to the two characteristics of “peace of mind” and “relaxation of the body.” “Peace of mind” is to eliminate all the adverse effects of sub-stimuli on the cerebral cortex. The combination of consciousness and exercise can stimulate the cerebral cortex, causing excitement in one area of the cerebral cortex, while other areas enter a state of inhibition and get sufficient rest. Taijiquan can improve the function of the central nervous system, improve the coordination between organs in the body, and play a role in regulating and training brain function (57). Compared with simple exercise training, Taijiquan exercise is to improve people's psychology, life and behavior, adjust the physical and mental conditions of insomnia patients, fundamentally cure insomnia.
This systematic review has some advantages and limitations. We conducted a relatively comprehensive systematic review, and the patient types included cancer, fibromyalgia and normal elderly people, etc. There were many diseases, so we could objectively evaluate the efficacy of Taijiquan on insomnia. Compared with previous systematic reviews (58), we included more RCTs with a larger sample size and strictly limited inclusion and exclusion criteria, with higher credibility. In terms of limitations, we only selected PSQI as the only evaluation index. However, most of the other evaluation results were insufficient or original data could not be obtained. In addition, subgroup analysis is lacking randomized controlled studies for some diseases, which may be biased.
In reviewing almost all about Taijiquan to improve insomnia, the high quality of research, we believe that Taijiquan to improve insomnia is convincing, however, the effects of different groups for different styles of Taijiquan treatment is not clear, Taijiquan differences between different age also needs to continue to study, different intervention dose and frequency of the need to continue to study. In addition, further research is needed on the physiological mechanism of Taijiquan in improving insomnia. Future research directions require more large-sample, multi-center, high-quality randomized controlled trials. It is necessary to further optimize the application of different types of Taijiquan in insomnia.
ConclusionIn conclusion, our meta-analysis showed that Taijiquan can improve sleep quality and improve insomnia. It provides evidence for taijiquan to treat different insomnia people and improve sleep quality. Subgroup analysis showed that Taijiquan can also improve insomnia caused by different diseases (except cerebrovascular diseases), which can be used as a supplement and alternative treatment for insomnia. There was no difference in the efficacy of different forms of Taijiquan, and there was no significant difference in the effect of Taijiquan on improving sleep between Chinese and Americans.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributionsDH and ZL conceptualized the study design, search and filter the title and abstract of the article, and confirmed the data and statistical analysis. YW and XW drafted and supplemented the methodology. HL and YH solved the difference. YH provided the funds. YC and XL modified their English and provided help in data analysis. JQ and JC are responsible for supervision and quality control. All authors provided information about the direction of research and the contents of the manuscript. All authors approved the final version of the manuscript.
AcknowledgmentsWe would like to thank all the authors for their hard work and thank the teachers of Gannan Medical University and Yuebei People's Hospital for their help, and thanks to XP for her English help with this manuscript.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.892453/full#supplementary-material
References3. Mellor A, Hamill K, Jenkins MM, Baucom DH, Norton PJ, Drummond SPA, et al. Partner-assisted cognitive behavioural therapy for insomnia versus cognitive behavioural therapy for insomnia: a randomised controlled trial. Trials. (2019) 20:262. doi: 10.1186/s13063-019-3334-3
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Shi ML, Zhao M, Wang YH, Sun TY, Li XL, Ren F, et al. [Network meta-analysis of efficacy and safety of Chinese patent medicines in treatment of insomnia]. Zhongguo Zhong Yao Za Zhi. (2021) 46:5403–17. doi: 10.19540/j.cnki.cjcmm.20210407.503
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Ong JC, Manber R, Segal Z, Xia Y, Shapiro S, Wyatt JK, et al. A randomized controlled trial of mindfulness meditation for chronic insomnia. Sleep. (2014) 37:1553–63. doi: 10.5665/sleep.4010
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Yin X, Gou M, Xu J, Dong B, Yin P, Masquelin F, et al. Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Sleep Med. (2017) 37:193–200. doi: 10.1016/j.sleep.2017.02.012
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Riemann D, Baglioni C, Bassetti C, Bjorvatn B, Dolenc Groselj L, Ellis JG, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. (2017) 26:675–700. doi: 10.1111/jsr.12594
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Kim SB, Kim JY, Park SW, Lee NR, Lee SW, Kim YH, et al. Comparison of 2 methods of non-invasive treatment between transcutaneous electrical stimulation and pulsed electromagnetic field stimulation as replacement of invasive manual acupuncture. Acupunct Electrother Res. (2012) 37:247–61. doi: 10.3727/036012912X13831831256294
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Irwin MR, Olmstead R, Motivala SJ. Improving sleep quality in older adults with moderate sleep complaints: a randomized controlled trial of Tai Chi Chih. Sleep. (2008) 31:1001–8.
PubMed Abstract | Google Scholar
16. Siu PM, Yu AP, Tam BT, Chin EC, Yu DS, Chung KF, et al. Effects of Tai Chi or exercise on sleep in older adults with insomnia: a randomized clinical trial. JAMA Netw Open. (2021) 4:e2037199. doi: 10.1001/jamanetworkopen.2020.37199
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Xiong P, Spira AP, Hall BJ. Psychometric and structural validity of the pittsburgh sleep quality index among filipino domestic workers. Int J Environ Res Public Health. (2020) 17. doi: 10.3390/ijerph17145219
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Farah NM, Saw Yee T, Mohd Rasdi HF. Self-reported sleep quality using the Malay version of the pittsburgh sleep quality index (PSQI-M) in Malaysian adults. Int J Environ Res Public Health. (2019) 16. doi: 10.3390/ijerph16234750
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Frye B, Scheinthal S, Kemarskaya T, Pruchno R. Tai Chi and low impact exercise: effects on the physical functioning and psychological wellbeing of older people. J Appl Gerontol. (2007) 26:433–53. doi: 10.1177/0733464807306915
CrossRef Full Text | Google Scholar
21. Wang C, Schmid CH, Rones R, Kalish R, Yinh J, Goldenberg DL, et al. A randomized trial of tai chi for fibromyalgia. N Engl J Med. (2010) 363:743–54. doi: 10.1056/NEJMoa0912611
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Cheung DST, Takemura N, Lam TC, Ho JCM, Deng W, Smith R, et al. Feasibility of aerobic exercise and Tai-Chi interventions in advanced lung cancer patients: a randomized controlled trial. Integr Cancer Ther. (2021) 20:15347354211033352. doi: 10.1177/15347354211033352
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Zhu D, Dai G, Xu D, Xu X, Geng J, Zhu W, et al. Long-term effects of Tai Chi intervention on sleep and mental health of female individuals with dependence on amphetamine-type stimulants. Front Psychol. (2018) 9:1476. doi: 10.3389/fpsyg.2018.01476
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Wang C, Schmid CH, Fielding RA, Harvey WF, Reid KF, Price LL, et al. Effect of tai chi versus aerobic exercise for fibromyalgia: comparative effectiveness randomized controlled trial. BMJ. (2018) 360:k851. doi: 10.1136/bmj.k851
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Li F, Fisher KJ, Harmer P, Irbe D, Tearse RG, Weimer C, et al. Tai chi and self-rated quality of sleep and daytime sleepiness in older adults: a randomized controlled trial. J Am Geriatr Soc. (2004) 52:892–900. doi: 10.1111/j.1532-5415.2004.52255.x
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Yilmaz Gokmen G, Akkoyunlu ME, Kilic L, Algun C. The effect of T'ai Chi and Qigong training on patients with obstructive sleep apnea: a randomized controlled study. J Altern Complement Med. (2019) 25:317–25. doi: 10.1089/acm.2018.0197
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Hosseini H, Esfirizi MF, Marandi SM, Rezaei A. The effect of Ti Chi exercise on the sleep quality of the elderly residents in Isfahan, Sadeghieh elderly home. Iran J Nurs Midwifery Res. (2011) 16:55–60.
PubMed Abstract | Google Scholar
28. McQuade JL, Prinsloo S, Chang DZ, Spelman A, Wei Q, Basen-Engquist K, et al. Qigong/tai chi for sleep and fatigue in prostate cancer patients undergoing radiotherapy: a randomized controlled trial. Psychooncology. (2017) 26:1936–43. doi: 10.1002/pon.4256
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Lü J, Huang L, Wu X, Fu W, Liu Y. Effect of Tai Ji Quan training on self-reported sleep quality in elderly Chinese women with knee osteoarthritis: a randomized controlled trail. Sleep Med. (2017) 33:70–5. doi: 10.1016/j.sleep.2016.12.024
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Jones KD, Sherman CA, Mist SD, Carson JW, Bennett RM, Li F, et al. A randomized controlled trial of 8-form Tai chi improves symptoms and functional mobility in fibromyalgia patients. Clin Rheumatol. (2012) 31:1205–14. doi: 10.1007/s10067-012-1996-2
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Larkey LK, Roe DJ, Weihs KL, Jahnke R, Lopez AM, Rogers CE, et al. Randomized controlled trial of Qigong/Tai Chi Easy on cancer-related fatigue in breast cancer survivors. Ann Behav Med. (2015) 49:165–76. doi: 10.1007/s12160-014-9645-4
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Nguyen MH, Kruse A. A randomized controlled trial of Tai chi for balance, sleep quality and cognitive performance in elderly Vietnamese. Clin Interv Aging. (2012) 7:185–90. doi: 10.2147/CIA.S32600
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Irwin MR, Olmstead R, Carrillo C, Sadeghi N, Breen EC, Witarama T, et al. Cognitive behavioral therapy vs. Tai Chi for late life insomnia and inflammatory risk: a randomized controlled comparative efficacy trial. Sleep. (2014) 37:1543–52. doi: 10.5665/sleep.4008
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Irwin MR, Olmstead R, Carrillo C, Sadeghi N, Nicassio P, Ganz PA, et al. Tai Chi Chih compared with cognitive behavioral therapy for the treatment of insomnia in survivors of breast cancer: a randomized, partially blinded, non-inferiority trial. J Clin Oncol. (2017) 35:2656–65. doi: 10.1200/JCO.2016.71.0285
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Taylor-Piliae RE, Coull BM. Community-based Yang-style Tai Chi is safe and feasible in chronic stroke: a pilot study. Clin Rehabil. (2012) 26:121–31. doi: 10.1177/0269215511419381
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Taylor-Piliae RE, Hoke TM, Hepworth JT, Latt LD, Najafi B, Coull BM, et al. Effect of Tai Chi on physical function, fall rates and quality of life among older stroke survivors. Arch Phys Med Rehabil. (2014) 95:816–24. doi: 10.1016/j.apmr.2014.01.001
PubMed Abstract | CrossRef Full Text | Google Scholar
37. Maddali Bongi S, Paoletti G, Calà M, Del Rosso A, El Aoufy K, Mikhaylova S, et al. Efficacy of rehabilitation with Tai Ji Quan in an Italian cohort of patients with fibromyalgia syndrome. Complement Ther Clin Pract. (2016) 24:109–15. doi: 10.1016/j.ctcp.2016.05.010
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Wang W, Sawada M, Noriyama Y, Arita K, Ota T, Sadamatsu M, et al. Tai Chi exercise versus rehabilitation for the elderly with cerebral vascular disorder: a single-blinded randomized controlled trial. Psychogeriatrics. (2010) 10:160–6. doi: 10.1111/j.1479-8301.2010.00334.x
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Budhrani-Shani P, Berry DL, Arcari P, Langevin H, Wayne PM. Mind-body exercises for nurses with chronic low back pain: an evidence-based review. Nurs Res Pract. (2016) 2016:9018036. doi: 10.1155/2016/9018036
PubMed Abstract | CrossRef Full Text | Google Scholar
40. Wu S, Chen J, Wang S, Jiang M, Wang X, Wen Y, et al. Effect of Tai Chi exercise on balance function of stroke patients: a meta-analysis. Med Sci Monit Basic Res. (2018) 24:210–15. doi: 10.12659/MSMBR.911951
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Li F, Harmer P, Fitzgerald K, Eckstrom E, Stock R, Galver J, et al. Tai chi and postural stability in patients with Parkinson's disease. N Engl J Med. (2012) 366:511–9. doi: 10.1056/NEJMoa1107911
PubMed Abstract | CrossRef Full Text | Google Scholar
42. Zhou S, Zhang Y, Kong Z, Loprinzi PD, Hu Y, Ye J, et al. The effects of Tai Chi on markers of atherosclerosis, lower-limb physical function, and cognitive ability in adults aged over 60: a randomized controlled trial. Int J Environ Res Public Health. (2019) 16. doi: 10.3390/ijerph16050753
PubMed Abstract | CrossRef Full Text | Google Scholar
44. Lu H, Yu J, Qiaoping Y, Zhu H. Taijiquan can improve the sleep of cancer patients with insomnia. Chin Nurs Res. (2002) 79:799.
留言 (0)