
記住我
For the current pilot study, we recruited 160 patients prescribed at least one of the study drugs. The participants' characteristics are listed in Table 3. Most (100/160, 62.5%) of the included patients were from the inpatient settings, while the rest were recruited from one cardiology outpatient clinic. The participants' mean age was 54 ± 14 years, ranging from 25 to 85. Most participants were males (130/160; 81.25%). Recruited patients descended from different ethnicities, where 52.5% were Arabs, 38% were South Asians, and 7.5% were Austronesians (from the Philippines and Indonesia).
Table 3 Participants’ characteristicsIn the inpatient group (N = 100), 67% were starting on clopidogrel at recruitment. At the same time, 77 patients of all participants (N = 160, 48%) were prescribed clopidogrel at or before recruitment. Atorvastatin was the most commonly (119/160; 74.4%) prescribed drug among all participants. Rosuvastatin was prescribed less frequently (33/160; 21%), while warfarin was the least prescribed medication in our cohort (7/160; 4%). Moreover, 75/160 (47%) cases received a combination of clopidogrel and statin.
As expected, the clinical presentation of patients at recruitment varied widely between the inpatient and outpatient settings. In the inpatient group (N = 100), 64% of patients were admitted due to myocardial infarction (MI). In comparison, 17% were admitted due to stroke, and the rest were admitted for various reasons (e.g., atrial fibrillation, cardiomyopathy). In the same inpatients' group, 37% were recruited following a percutaneous coronary intervention in the. In comparison, 51 of the 60 participants (84%) in the outpatient group had a history of coronary artery disease, and seven patients (11%) had had at least one invasive cardiac intervention before recruitment. Patients in the outpatient group were mainly recruited because they were prescribed a statin; however, eight patients were also on clopidogrel, and two were using warfarin.
PGx genotyping resultsFor CYP2C19 tested variants, the alternative alleles at the two splicing variants, rs1276925 and rs4244285, were the most common, with frequencies of 26.6% and 25.3%, respectively. These alleles, defining together CYP2C19*2, appear with a frequency higher than their worldwide frequency in gnomAD [18] (17.4% and 17.95%, respectively) and the 1000Genome [19] (17.6% and 17.1%, respectively) databases. Another common alternative CYP2C19 allele in our cohort is the CYP2C19*17 tag variant, rs12248560, which constituted 20% of the tested alleles, an equal frequency to that reported in gnomAD data (20%). Three SNPs (CYP2C19*5/*6/*8) showed no alternative alleles in our pilot cohort. The same variants are infrequent in all gnomAD populations [18].
Among all the tested variants, the alternative allele (T) in VKORC1: rs9923231 occurred with the highest frequency compared to all impaired function alleles in our cohort. It was reported with a frequency of 38%, which is higher than its frequency in all gnomAD populations (32.6%) [18]. Similarly, the impaired function allele C at SLCO1B1: rs4149056 was reported with a 16.9% frequency in our cohort, a frequency higher than in gnomAD and 1000Genome databases [19]. Table 4 lists the complete genotype frequencies at the tested variants in our cohort, with a comparison of the alternative alleles’ frequencies with their frequencies in gnomAD data (https://gnomad.broadinstitute.org/, accessed on 12 June 2022) and the results of the Chi-square test of independence. Statistically significant differences were found between the frequencies of alternative alleles in our cohort, and that reported in gnomAD all populations at the following variants: CYP2C19: rs4244285, rs12769205, rs4986893, rs12248560, VKORC1: rs9923231, and CYP2C9: rs1057910.
Table 4 Genotypes frequencies and a comparison of alternative allele frequency in UAE cohort and gnomAD all populationsClinical impact and guiding therapyThe resultant genotypes were translated into haplotypes and diplotypes for CYP2C19 and CYP2C9, according to the most recently updated haplotype definitions in PharmVar [19]. After inferring haplotypes and diplotypes, the phenotypes (enzyme activities) were predicted from the corresponding genes of the participants, as denoted in CPIC guidelines. Participants who were not found to carry any of the tested impaired function alleles were designated as “probably *1/*1” and predicted to have regular enzyme activity.
For CYP2C19 enzyme activities, 19 participants (11.9%) were poor metabolizers (i.e., carry two of the impaired function alleles *2, *3, *4, *5, *6, *8, *35), 56 (35%) intermediate metabolizers (i.e., carry one of the impaired function alleles listed previously), 45 (28.1%) normal metabolizers, and 40 (25%) were rapid or ultrarapid metabolizers (i.e., have one or two *17 alleles, respectively). According to the latest CPIC issued CYP2C19-clopidogrel recommendations [20], patients with intermediate CYP2C19 activity should avoid clopidogrel if they are using it for acute coronary syndrome (ACS) or following a percutaneous cardiac intervention (PCI). Still, no similar recommendation is given for clopidogrel use in CVD indications other than ACS and PCI in intermediate metabolizers. In contrast, poor CYP2C19 metabolizers are recommended to avoid clopidogrel for all CVD indications. Moreover, those taking it for NVD indications, like strokes, should consider an alternative if they have an intermediate enzyme activity and avoid it if they have poor activity. Collectively, 46.9% of our cohort should receive a recommendation to avoid the use of clopidogrel or consider an alternative P2Y12 inhibitor. Figure 1 illustrates the distribution of our cohort according to their CYP2C19 metabolic status predicted by their genetic testing results.
Fig. 1
CYP2C19 diplotypes and predicted metabolizer status. Pie charts representing the CYP2C19 metabolizer status displayed in percentage and their associated diplotypes
For CYP2C9, diplotypes were inferred from the most common star alleles, *2 and *3. In our cohort, 4% are poor CYP2C9 metabolizers (i.e., *2/*2, *2/*3, or *3/*3), while 44.4% are intermediate metabolizers (i.e., one *2 or *3 allele). The results of CYP2C9 diplotypes and predicted enzyme functionality are illustrated in Fig. 2.
Fig. 2
CYP2C9 diplotypes and predicted phenotypes. A pie chart demonstrates the predicted phenotypes and associated diplotypes of CYP2C9 pharmacogene
Subsequently, we collectively analyzed variants in CYP2C9 and VKORC1, which interact with warfarin doses. It was found that only 32 of the 160 participants (20%) carried wild-type (i.e., reference) alleles at VKORC1-1639G > A, CYP2C9*2, and CYP2C9*3, leaving 80% of our cohort with at least one alternative allele at any of the three SNPs. According to the CPIC warfarin pharmacogenetic-guided dosing guidelines [21], the presence of an alternative allele at any of these sites (VKORC1-1639G > A, CYP2C9*2, or CYP2C9*3) results in a strong recommendation for adjusting the warfarin dose according to one of the published dosing PGx-algorithms (e.g., IWPC algorithm [22]). Accordingly, if the patients’ genotypes are available in health records, 80% of our cohort are eligible for a genetic-modified warfarin dose whenever they need a warfarin prescription. Moreover, The same CPIC guidelines [21] recommend modifying the dose according to the presence of any of the following variants: CYP2C9*6/*8/*11 and CYP4F2 rs2108622 T allele. Using the IWPC online available calculator [22], we calculated the genetic-warfarin dose of participants, then adjusted the resultant genetic dose for the other CYP2C9 alleles and CYP4F2 rs2108622 T allele. The participants were then grouped into three groups according to age, less than 50 years, 50 to 70 years, and more than 70 years. The range and average warfarin genetic dose for each group were calculated and represented as a box and whiskers plot in Fig. 3.
Fig. 3
Average warfarin genetic dose for participants categorized by age. The genetic dose was calculated by the IWPC algorithm, which considers age, BMI, amiodarone use, using CYP2C9 inhibitors, and the genotypes at VKORC1-1639G > A, CYP2C9*2, and CYP2C9*3. The dose was adjusted for CYP4F2 rs2108622 genotypes and represented as mg/day. The numbers represent each group's minimum, maximum, median (the line), and average dose
The resultant average dose for the three age groups was lower than that reported by Shendre and colleagues [23], who reported the average warfarin dose for the same three age groups from a real-world setting. The average warfarin dose was 8.1 mg/day compared to 5.1 mg/day in the young (< 50) group, 7.2 mg/day compared to 4.4 mg/day in middle-aged (50–70), and 7.2 mg/day compared to 3.1 mg/day for elderly (> 70), in Shendere and coworker’s cohort compared to ours, respectively. Nevertheless, we prefer interpreting these observed differences with extreme caution, given that we built our calculation on hypothesizing that our participants will be prescribed warfarin at the time of recruitment and utilized their recruitment age and BMI data, which are changing variables.
Indeed, warfarin was the least prescribed medication for our participants. We had only seven patients receiving a warfarin prescription at recruitment. Consequently, we tested their warfarin genotype-adjusted dose and compared it with their clinically prescribed one, which depended exclusively on the patient’s clinical characteristics. The result of this analysis is demonstrated in Table 5. Unfortunately, the observed warfarin dosing data are limited by this subset's low number of samples. However, the high prevalence of alternative VKORC1 and CYP2C9 alleles in the entire cohort indicates the potential significance of PGx-guided dosing in our population whenever warfarin is prescribed.
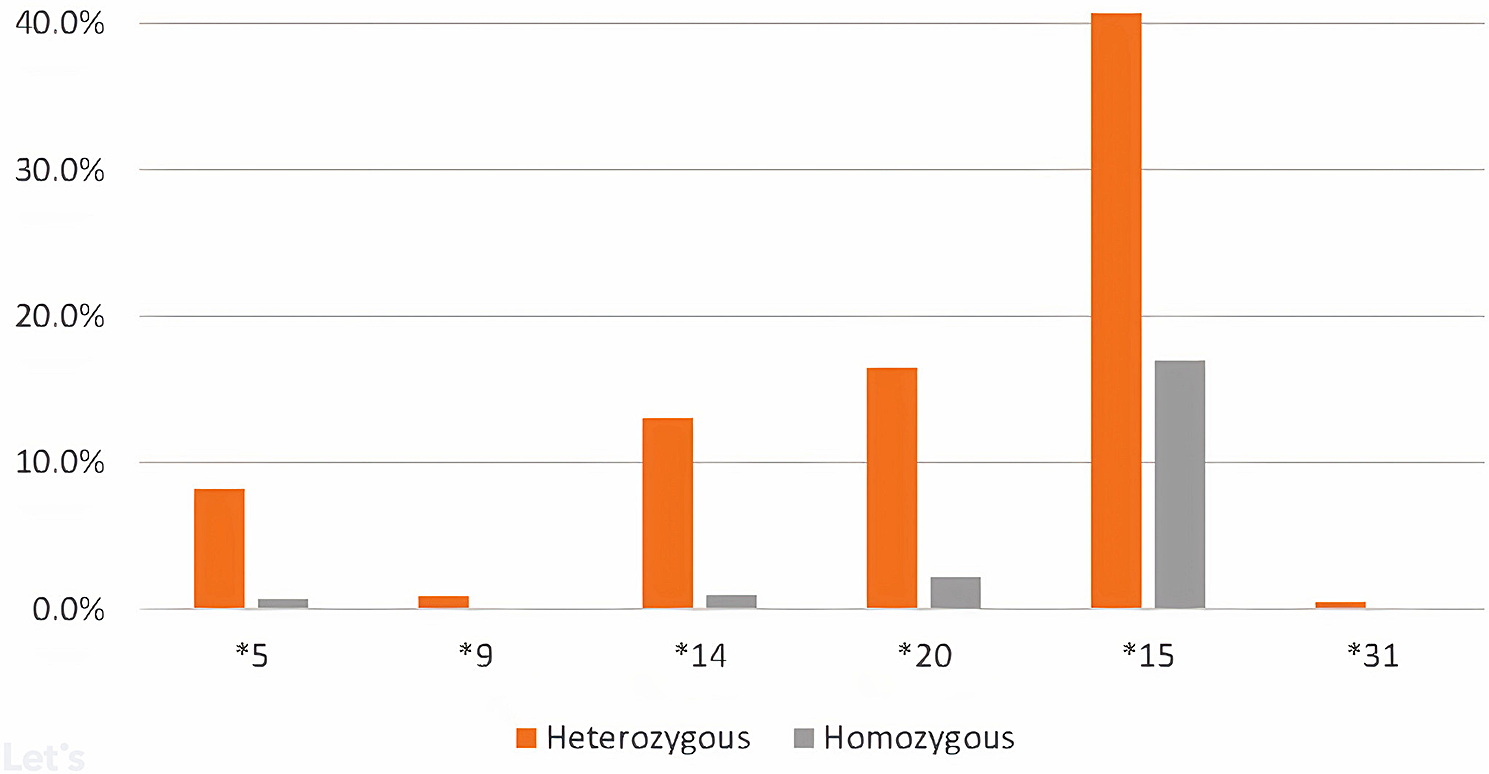
Table 5 Warfarin gene-calculated dose versus clinical-prescribed doseFor statins, 50 participants (31.25%) carried at least one allele at the genotyped SLCO1B1 variant, increasing their risk of developing myopathy. CPIC recently issued guidelines for statin-associated musculoskeletal symptoms depending on SLCO1B1, ABCG2, and CYP2C9 [24]. Moreover, PharmVar recently published SLCO1B1 haplotypes [25], which were cited in the new CPIC recommendations. Both updates were issued following the initiation of our pilot study and were not considered in its design. However, these updates prompted us to add new variants to our targeted SNPs in the extended clinical trial. The newly added variants will cover the most common SLCO1B1 haplotypes (*5 and *15) and the ABCG actionable variant, rs2231142 G > T, which interacts with rosuvastatin.
Interestingly, when intersecting the recommendations generated, we found that only seven participants carried reference alleles at all the tested variants and received no recommendations in their PGx-testing reports. In other words, 96% (153/160) of participants received at least one PGx clinical guidance.
Finally, after optimizing the pipeline, pharmacogenomic testing results were issued within 24 to 48 h of collecting the samples. Ensuring that the clinician receives the reports within this time frame is crucial for the successful planning for the extended implementation trial.
留言 (0)