
記住我









The patient was diagnosed as having bilateral carotid body tumors and supposedly an aortic body tumor at the age of 43 and eventually underwent resections of bilateral carotid body tumors treated by head and neck surgeons in a local hospital at the age of 52. Following surgery, the patient had slight hoarseness due to residual right recurrent nerve palsy, which was functionally compensated by the left recurrent nerve. The pathology of the tumors was compatible with paraganglioma on both sides and was classified as Shamblin grade IIIa. Subsequently, familial succinate dehydrogenase subunit D (SDHD) mutation was noted. In fact, his family history was positive; his sister had a documented history of skull base tumor surgery and two relatives undergone neck tumor surgeries. Five years later, a contrast-enhanced computed tomography (CT) scan showed an enlarged tumor of 45 mm in size located at the aortopulmonary mediastinum. Sequential follow-up with diagnostic CT scans were retrospectively evaluated (Fig. 1). At the age of 43 years, a hypervascularized tumor of approximately 8 mm was found and inferred to be an aortic body tumor (Fig. 1A), and he, thereafter, was followed by a thoracic surgeon at the same hospital for his convenience. His mediastinal tumor became 29 mm in diameter at the age of 52 (Fig. 1B). Reportedly, the tumor was considered high risk for surgical resection due to its hypervascularity and proximity to vital organs, and it was further followed up at that time. It continued to grow and expanded to 45 mm in maximum diameter by the age of 57. Although there had been no clinical evidence of respiratory distress or dysphagia, progressive compression of the left bronchus and esophagus was revealed by the CT scans. Thus, he was referred to our cardiovascular surgical outpatient clinic for possible surgical management with or without cardiopulmonary bypass support. Based on the previously known genetic mutation, the tumor was thought to be a paraganglioma. We decided to perform surgery because we were concerned about the increased difficulty in removal of the tumor due to prominent vascularity and seemingly tight adhesion to the surrounding organs (Figs. 1C, 2A and B), although he was not being subjected to an imminent risk of sudden death due to a rapid expansion of the tumor as documented in the literature [1].
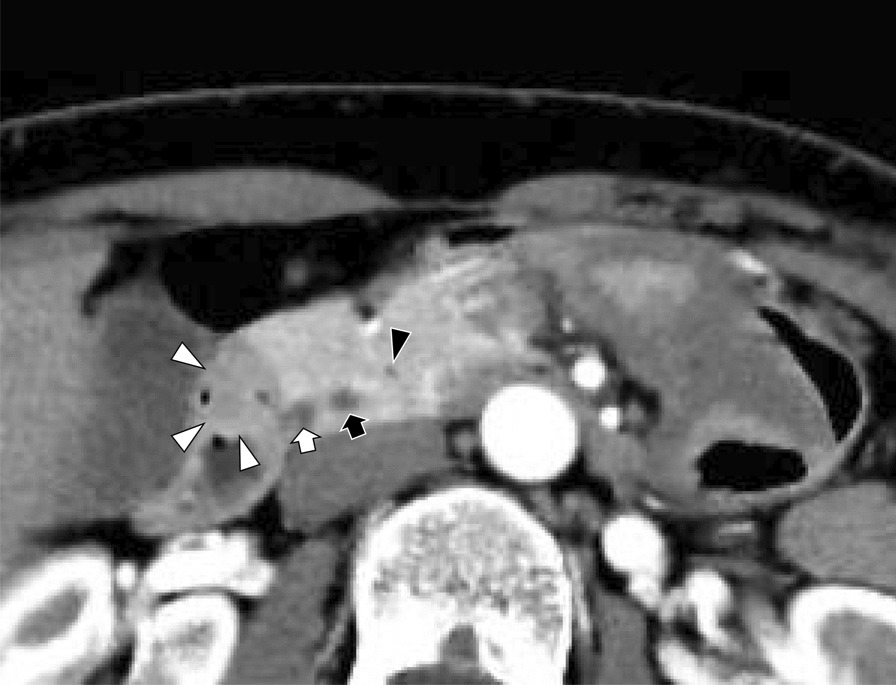
Fig. 1
Computed tomographic images depicting serial tumor growth. When the patient was 43 years old, the tumor measured 8 mm in diameter and subsequently exhibited a gradual tendency to expand (A). Nine years later, the tumor size increased up to 29 mm (B) and it turned out to be 45 mm 4 years later (C). As the tumor expanded, the compression of the left bronchus and esophagus progressed over time
Fig. 2
Preoperative computed tomography demonstrating space occupying mass between aorta and pulmonary artery. A Sagittal view of the tumor and great vessels was shown. The tumor would be severely adherent to the pulmonary artery trunk and ascending aorta underneath the arch. B Coronal view of the tumor and great vessels was shown. The distorted configuration of the aortic arch compressed from underneath and concaved shape of the tumor were well illustrated. These figures raise a great concern about the presence of severe adhesions around the tumor
We proceeded with the functional evaluation of his tumor. 123Iodine-MIBG scintigraphy showed focal high tracer uptake in the aortic arch. The tumor was assessed as a non-functional tumor, without catecholamine secretory capacity. A 24-h urine examination revealed that adrenaline and noradrenaline or their metabolites, including metanephrine and normetanephrine, levels were within normal limits. It was inferred that there would be only a negligible risk for hypertensive crisis immediately after selective angiography of the feeding vessels even after surgical manipulation. Thus, preoperative embolization of the feeding arteries was planned as follows.
CT angiography demonstrated feeding arteries originating from the left internal thoracic artery, bronchial artery, and coronary artery circumflex branches (Fig. 3A, B). The left internal thoracic and bronchial arteries feeding the major component of the tumor were selectively embolized with the fragments of sponzel (Fig. 4A, C). The left circumflex artery was not intervened to avoid potential myocardial infarction following the embolization procedure. Systemic blood pressure of the patient did not change during the procedure. Post-embolization angiography demonstrated no significant opacification of the tumor (Fig. 4B, D).
Fig. 3
The tumor localization and the routes of major feeding arteries for the tumor are visualized by 3-dimensional CT. The tumor was located in the area surrounded by the aortic arch and pulmonary artery, and was fed by a well-developed mediastinal branch (arrow) of the left internal thoracic artery (LITA) that flew into the right dorsal side of the tumor. The other main feeding artery was derived from the bronchial artery (B), which flew from the left dorsal side of the tumor. A Viewed from the left lateral side, B Viewed from the right lateral side
Fig. 4
Intraoperative digital angiograms showing embolization of the major feeding arteries. A The feeding arteries from the LITA before embolization. The tumor was densely stained. B The opacified area decreased in tumor staining (surrounded by arrows) after embolization of the feeding arteries through the LITA. C Tumor stain via the feeding arteries from a bronchial artery (BA) was also confirmed before embolization. D Following embolization, the tumor staining through BA was completely eliminated. LITA left internal thoracic artery, BA bronchial artery
On the following day, a surgical team consisting of thoracic and cardiovascular surgeons elected to resect the aortic body tumor using a video-assisted small left thoracotomy approach combined with a median sternotomy approach in an attempt to complete en bloc resection without cardiopulmonary bypass. Thoracic surgeons dissected the tumor of the descending thoracic aorta, left pulmonary artery, left bronchus, and esophagus using a thoracoscopic approach by opening the left fourth intercostal space. Through the fifth intercostal space on the left mid-clavicular line, a single port was created to develop an ideal surgical field. A thoracoscope was inserted via the small thoracotomy site. The tumor was severely adherent to the pulmonary artery trunk and ascending aorta underneath the arch, particularly around the ductus arteriosus. Nonetheless, a preservation of the left recurrent nerve was feasible with thoracoscopic magnified view. The boundary between the adventitia of the great vessels and the tumor was indefinite. Median sternotomy was then performed by cardiovascular surgeons. The root of the feeding vessel derived from the left internal thoracic artery was clipped and the tumor on the right side was dissected. The border between the pericardial reflection and the tumor was easy to observe. LigaSure™ vessel sealing system (Covidien, Dublin, Ireland) was used as an appropriate since there were tiny drainage vessels. Dorsal dissection of the aortic arch was performed; thereafter, the tumor became more mobile. As with the thoracoscopic findings, adhesions around the ascending aorta and pulmonary artery trunk were the most severe, but it was possible to proceed with dissection while preserving the adventitia of the great vessels. (Fig. 5A, B) Intraoperative hemodynamics was stable and bleeding was minimal; therefore, the resection was feasible without the use of cardiopulmonary bypass. Blood transfusion was not required. The operative time was 351 min. The patient was weaned off the ventilator on the day of surgery. He did not develop dysphagia, and the degree of hoarseness unchanged from preoperative status. The patient was discharged on the ninth postoperative day uneventfully. Macroscopic appearance is shown in Fig. 6. The tumor tissue was immunohistochemically stained for chromogranin A and synaptophysin. Both immunohistochemical studies showed positive staining for the neuroendocrinological proteins. Accordingly, definitive diagnosis for paraganglioma was made. The grading system for adrenal pheochromocytoma and paraganglioma, GAPP score, was 2 with Ki-67 of more than 3%. In addition, pheochromocytoma of the adrenal gland scaled score, PASS, was assessed 0 indicating low grade malignancy.
Fig. 5
Intraoperative photos. A Thoracoscopic image from the left side of the tumor. B Direct vision of the right lateral side of the tumor through a median sternotomy. Asc. A ascending aorta, Dec. A descending aorta, LPA left pulmonary artery, PN phrenic nerve, RPA right pulmonary artery, SVC superior vena cava, T tumor
Fig. 6
Macroscopic and microscopic findings of the resected tumor. A Scale bar is cm. Cross-sectional appearances of the tumor after formalin fixation. Tumor necrosis induced by preoperative feeder embolization was noted as darkish area. Arrowheads point the flattened surface adjacent to the undersurface of the aortic arch. Arrows point the protruding surface of caudal end of the tumor adjacent to concaved pulmonary artery trunk. B Scale bar is 100 µm. Nests of cells with abundant cytoplasm were demonstrated (hematoxylin and eosin stain, × 200). C, D Scale bar is 100 µm. The tumor cells demonstrated positive staining for chromogranin A and synaptophysin (× 200)
留言 (0)