
記住我




A 70-year-old woman with a history of insulin-dependent type 2 diabetes and inflammatory arthritis who is currently on prednisone and adalimumab was referred to the wound care center for a 3-month history of a painful left heel ulcer after a pedicure. She developed a left heel ulcer after her heel callus was smoothened (Figure 1). There has been only scant serous drainage. She had no systemic symptoms. She took amoxicillin/clavulanic acid and trimethoprim-sulfamethoxazole for 7 days without improvement. How would you manage this case?
 Figure 1:
Figure 1: A 70-YEAR-OLD WOMAN WITH A PAINFUL CHRONIC HEEL ULCER
INTRODUCTIONAlthough all chronic wounds are colonized by microbes and not all wounds are infected, antibiotics are widely prescribed in wound care settings. Skin and soft tissue infection is one of the most common types of infection; approximately 15% of Medicare beneficiaries (8.2 million) had at least one type of wound with or without infection in 2014, and total Medicare spending for all wound types is $28.1 to $96.8 billion.1 Wise et al2 reported that up to 50% of prescribed antibiotics were unnecessary or inappropriate in both the outpatient and inpatient settings. Antibiotic misuse in wound care occurs for many reasons, including diagnostic uncertainty regarding the presence of a bacterial infection, insufficient clinician knowledge about when antibiotics are necessary, clinicians’ fear of achieving unfavorable patient outcomes, and patient demand.3 It is critical to accurately assess whether chronic wounds are infected or colonized and to choose appropriate antibiotics based on cultures to treat infected wounds. In this article, the authors review wound infection stages, host resistant factors, and virulence factors affecting the progress of wound infection stages, as well as specimen collection methods, common causative organisms, and commonly prescribed antibiotics in wound care settings.
WOUND INFECTION STAGESBacteria are present in all chronic wounds. The wound infection continuum encompasses many stages, from initial contamination of the wound to systemic infection if it is not treated properly (Figure 2).
 Figure 2:
Figure 2: WOUND INFECTION STAGES
Contamination is the presence of nonreplicating organisms on the surface of a wound.4 All chronic wounds are contaminated. These contaminants come from normal skin flora and the environment. Most organisms from the environment cannot multiply in wounds. Examples of normal skin flora include Staphylococcus epidermidis and Staphylococcus aureus. Intact skin provides a natural physical barrier; however, once a wound develops, this natural protection is lost, and normal skin flora may gain entry.
Colonization is the presence of replicating organisms adherent to the wound in the absence of injury to the host or immune response from the host. It is considered a normal state and is not associated with active disease or delayed wound healing.
Critical colonization is the presence of replicating organisms without invasion but interfering with wound healing.4 Although there is no inflammation or fever, discoloration or odor may be observed, and exudate may be increased. Topical antiseptics should be considered to control the bioburden of the colonizing organisms. Topical antiseptics in conjunction with wound debridement of devitalized tissue and wound cleansing are beneficial.
Wound infection is the presence of replicating organisms within a wound that overwhelm the host’s immune response, resulting in spreading cellulitis and host injury. Topical or systemic antibiotic treatment is required in addition to debridement of the wound bed.
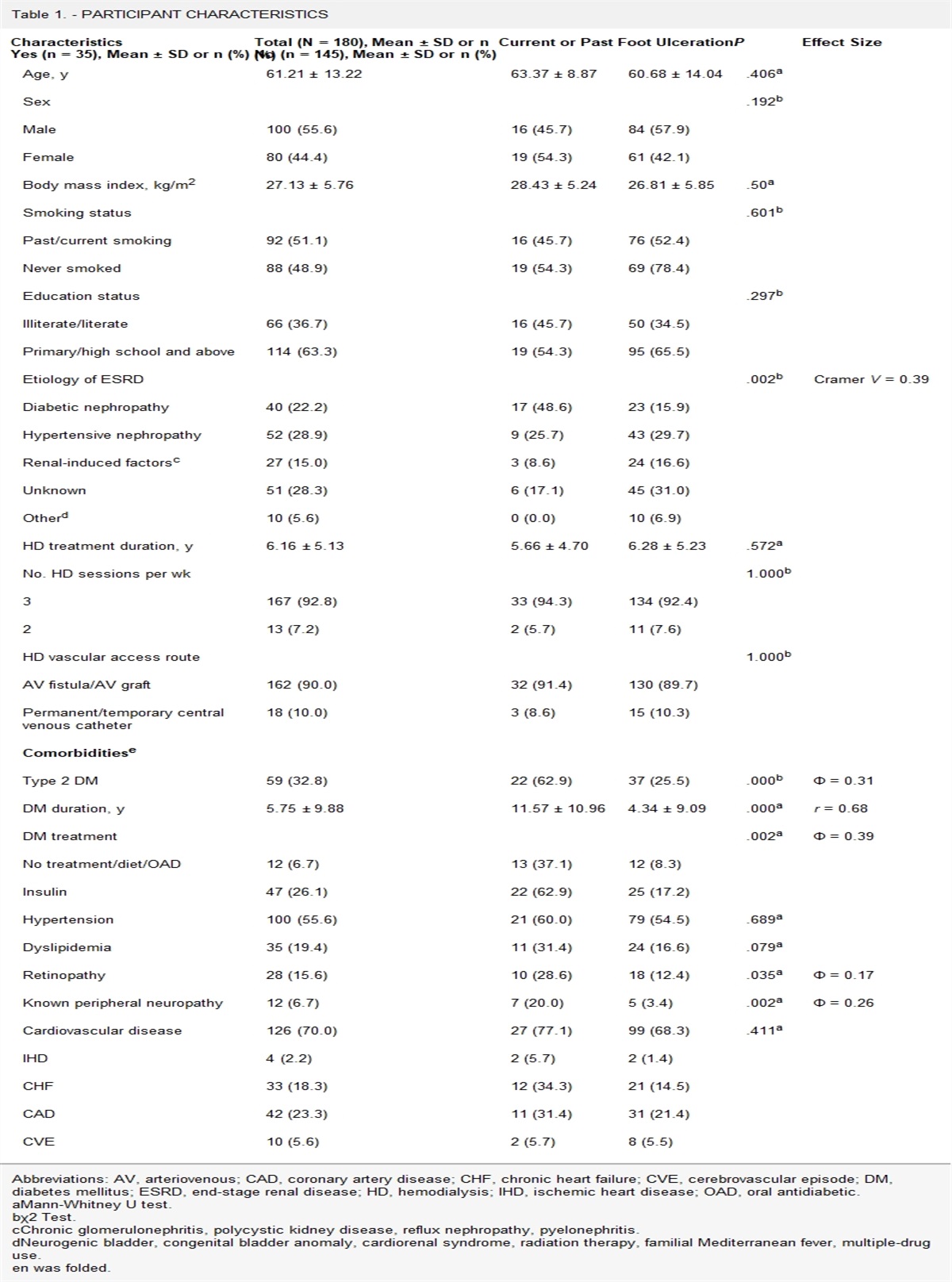
Factors Affecting Wound Infection ProgressionWhether a wound remains harmlessly colonized or becomes infected is influenced by microbe-host interactions, particularly the abundance and density of pathogens, the virulence of the organisms, and the host immune response.5 Normal, intact skin can often contain upward of 105 colony-forming units of bacteria per gram of tissue without any clinical problems.4 However, bacterial loads higher than this in open wounds are often associated with infection because of the absence of an intact epithelium. Highly pathogenic organisms, such as β-hemolytic Streptococcus, can cause infections at significantly lower colony-forming unit levels, as can less pathogenic organisms when the virulence factors of the wound microbiota act synergistically. Virulence is the ability of a microorganism to cause disease in the host. Virulence factors help microorganisms to invade the host, cause disease, and evade host defenses.6 Examples of virulence factors include endotoxin produced by Gram-negative rods and proteases produced by S aureus. Host resistant factors are summarized in Table 1.
Table 1 - HOST FACTORS THAT INCREASE CHANCES OF WOUND INFECTION Host Resistance Local Factors Systemic Factors Large wound area Vascular disease Increased wound depth Edema Degree of chronicity Malnutrition Anatomic location Diabetes Foreign body Alcohol use disorder Necrotic tissue Prior surgery or radiation Mechanisms of injury ImmunocompromiseBiofilms are complex communities of aggregated bacteria embedded in a self-secreted extracellular polysaccharide matrix that can attach to a variety of surfaces, including wounds and medical devices.4 The bacteria are protected from host defenses and develop significant resistance to antibiotic treatment. Biofilms can be seen on at least 70% of chronic wounds.7 Biofilms can contribute to infection, cause inflammation, and delay wound healing. Identifying and managing biofilms are critical in wound care.
DIAGNOSING INFECTIONWound infection is primarily diagnosed clinically. The classic signs of inflammation suggesting cellulitis include erythema, warmth, swelling, pain, and purulent secretions. Noninfectious etiologies such as venous insufficiency, lymphedema, or reflex sympathetic dystrophy can mimic some of these findings. Secondary signs that suggest infectious etiologies, including friable or discolored granulation tissue, pocketing, undermining, or foul odor, need to be assessed to rule out noninfectious etiologies.3 After wound cleaning and debridement, obtain microbiologic cultures to identify the causative organisms. A deep ulcer with necrotic muscle, undermined tissue, or sinus tracts suggests deeper infection involving fascia, tendon, muscle, and bone. Suspect osteomyelitis when bone is exposed in a chronic ulcer or fails to heal with proper management, or if the patient has recurrent soft tissue infections associated with a chronic ulcer. Radiologic imaging such as MRI is useful to assess for bone involvement when osteomyelitis is suspected. Bone biopsy enables histologic examination to confirm the diagnosis and cultures to identify the causative organisms.8 Systemic symptoms (eg, fever, altered mental status) or elevated inflammation markers are usually absent in wound infections.
SPECIMEN COLLECTIONWound culture is the best way to determine the optimal antibiotic regimen when a wound is clinically infected. The wound should be cleansed with a nonbactericidal agent and debrided before collecting a specimen for culture.3 Obtaining tissue by curettage or biopsy is preferred to specimens obtained with swabs. Surface wounds and superficial material are unsuitable for anaerobic cultures, but specimens from deep wounds are acceptable for anaerobic cultures. It is best to collect a specimen for cultures before starting antibiotic therapy to avoid false-negative results. Order blood cultures when patients have systemic symptoms. When diabetic foot osteomyelitis is suspected, culture of bone specimens from deep within the osteomyelitic focus is considered the most accurate method for identification; however, deep-bone cultures are often difficult to obtain because of limited technical expertise, time, and availability of surgical tools or facilities.9 Soft tissue specimens collected via biopsy or aspiration have more reliable microbiologic concordance with bone cultures to identify diabetic foot osteomyelitis causative organisms than do specimens collected with a swab.10
MICROBIOLOGYThe major groups of microorganisms include bacteria, viruses, fungi, and parasites. Most wound infections are caused by bacteria, whereas fungal infections are most often observed in patients who are immunocompromised. One of the major characteristics of bacteria is their reaction to the Gram stain. Depending on the chemical and structural composition of the cell wall, some bacteria are Gram-positive, taking on the primary stain’s purple color, whereas others are Gram-negative, appearing pink due to the counterstain. Gram-stained bacteria are also described according to the cellular morphology, such as spherical “cocci” and rod-shaped “bacilli” (or simply “rod”), as well as the arrangement of cells, such as “in chains” or “in clusters.” For many culture types, the first result is the Gram stain of the specimen, which provides preliminary evidence of the abundance and types of organisms present in the sample. Gram-positive cocci and Gram-negative rods are common findings from a Gram stain of a wound specimen. After the Gram stain is performed, cultures are set up for bacterial identification, followed by antimicrobial susceptibility testing, as appropriate.
A variety of organisms are found in chronic wound infection (Table 2).3,10 The microbial flora in wounds appears to change over time. Normal skin flora such as S. aureus and β-hemolytic Streptococcus are predominant in early acute wounds. In contrast, aerobic Gram-negative rods and anaerobes are seen in long-term chronic wounds, which are frequently polymicrobial in nature. In diabetic foot infections (DFIs), superficial infections are usually caused by Gram-positive cocci including S aureus, Streptococcus agalactiae, and Streptococcus pyogenes, whereas deep, chronically infected wounds more commonly have polymicrobial infections with Gram-negative rods and anaerobes in addition to the above organisms.11 Polymicrobial infection is common in infected pressure injuries (PIs) as well.12
Table 2 - COMMON BACTERIA IN WOUND CARE SETTINGS Gram-Positive Cocci Gram-Negative Rods Anaerobes Staphylococcus aureus Pseudomonas aeruginosa Bacteroides fragilis Streptococcus pyogenes Escherichia coli Clostridium perfringens Streptococcus agalactiae Enterobacter aerogenes Peptostreptococci Coagulase-negative staphylococcia Klebsiella pneumoniae Enterococcus faecalis Acinetobacter baumannii Stenotrophomonas maltophiliaaCommon in surgical site infection and hardware infection.
Streptococcus species, especially those that exhibit β-hemolysis when grown on blood agar, such as S pyogenes and S agalactiae, can cause a variety of skin and soft tissue infections.13 The severity varies from spontaneous resolution to life-threatening. Streptococcal toxic shock syndrome and necrotizing fasciitis are both medical emergencies. Nonpurulent cellulitis and erysipelas are most commonly caused by Streptococcus species. Monomicrobial necrotizing soft tissue infection is usually caused by S pyogenes. In DFIs, Streptococcus species are often found in early superficial infections or chronic complicated infections.
Staphylococcus aureusStaphylococcus aureus is responsible for a wide range of clinical manifestations, from folliculitis to life-threatening conditions such as endocarditis or empyema. Purulent cellulitis, abscesses, and surgical site infections are most commonly caused by S aureus.14 In DFIs, S aureus is also found in early superficial infections or chronic complicated infections. Staphylococcus aureus is categorized as either methicillin-resistant S aureus (MRSA) or methicillin-susceptible S aureus (MSSA), depending on its susceptibility against methicillin. However, MSSA is often referred to simply as S aureus, which can be ambiguous. Although MRSA was once considered exclusively a hospital-acquired pathogen, it is now prevalent in the community. Risk factors for MRSA infection include recent hospitalization, residence in a long-term care facility, recent surgery, hemodialysis, HIV infection, injection drug use, and prior antibiotic use.15
Coagulase-Negative StaphylococciCoagulase-negative staphylococci (CoNS) are a large group of Staphylococcus species that are normal flora of the skin and mucosa.16 They are described as such to distinguish them from more pathogenic coagulase-positive staphylococci, namely, S aureus. In wound care settings, CoNS are an important cause of surgical site infections and hardware-related infections. Diagnosis of CoNS infection is made by culture of CoNS as the predominant isolate or by repeated isolation of the same Staphylococcus species in serial cultures; CoNS are usually indicative of contamination or colonization when grown from a single superficial culture.
EnterococciEnterococci (Enterococcus faecalis, Enterococcus faecium) are regular inhabitants of the bowel and colonizers of the skin and mucosa. When enterococci are isolated from one single superficial wound culture, colonization is likely. However, enterococci can be the causative organisms of deep DFIs11,17 and infected PIs,12 particularly when isolated from multiple specimens. Whereas E faecalis tends to be susceptible to many antibiotics, E faecium is often highly resistant. Vancomycin-resistant enterococci (VRE), typically E faecium, are a major cause of hospital-acquired infections, and antibiotic options for them are limited. Risk factors for VRE acquisition include prior antibiotic exposure, hospitalization, and comorbidities.18
Pseudomonas aeruginosaPseudomonas aeruginosa is one of the most common Gram-negative rods recovered from clinical specimens. Pseudomonas aeruginosa can cause various skin and soft tissue infections, including ecthyma gangrenosum; burn wound infections; folliculitis associated with hot tub exposures; cellulitis, especially in neutropenic patients; surgical site infections; chronic wound infections; and osteomyelitis related to chronic decubitus ulcers or DFIs.19 Some hospital-acquired P aeruginosa infections may be fatal, especially in patients who are immuncompromised. Pseudomonas aeruginosa can develop multidrug resistance with antibiotic use, hospitalization, or ICU stay.20
EnterobacteralesEnterobacterales is a large order of Gram-negative rods, including Enterobacter aerogenes, Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis. They can cause chronic wound infections, deep DFIs,11 and infected PIs.12 Because Enterobacterales are enteric bacteria, they are often associated with perirectal abscesses or infected sacral PIs. Enterobacterales can harbor several antibiotic resistance genes and can become multidrug resistant, such as extended-spectrum β-lactamase (ESBL)-producing organisms or carbapenem-resistant Enterobacterales. These multidrug-resistant organisms are associated with prior antibiotic use, prolonged hospital stays, and residency in a long-term care facility.
AnaerobesAnaerobes, which are organisms that do not require molecular oxygen for growth, are frequently found in abscesses and other wound types with polymicrobial infections. Although many organisms, such as Staphylococcus and Enterobacterales, are facultative anaerobes and can grow anaerobically and aerobically, “anaerobes” generally refer to obligate anaerobes, which can only grow anaerobically, and the term is used as such in this article. Common anaerobes in wound care settings include Bacteroides fragilis, a Gram-negative rod; Peptostreptococcus species, a Gram-positive cocci; and Clostridium species, a Gram-positive rod. Bacteroides fragilis is commonly seen in abscesses located in the perirectal area or infected sacral PIs. Polymicrobial infections including anaerobes are commonly seen in complicated DFIs;11 infected deep PIs;12 or wounds with extensive local inflammation, necrosis, malodorous drainage, or gangrene with signs of systemic symptoms.
MANAGING INFECTIONInfected wounds require systemic antimicrobial therapy in addition to debridement and local wound care. It is essential to fully debride devitalized tissue and eradicate biofilm to achieve source control of associated infection.
AntisepticsAntiseptics play major roles in chronic wound care and are commonly used in wounds with colonization, critical colonization, and infection. Antiseptics differ from antibiotics primarily based on their application, which is exclusively topical. The use of antiseptics at dressing changes provides wound cleaning, irrigation, and debridement, reducing bacterial burden and suppressing biofilm formation and reformation.7 Antiseptics inhibit the growth and development of microorganisms through several mechanisms, including disruption of membrane proteins, damage to cell walls and cytoplasmic processes, and nuclear disruption. It is unlikely that antiseptics cause bacterial resistance. Common antiseptics for clinical use include dilute hypochlorite preparations and hypochlorous acid.
AntibioticsAn antibiotic is an antimicrobial substance that kills or inhibits bacterial growth and development. To reduce the risk of toxicities and development of resistance, antibiotics should be used only if clinical or laboratory evidence suggests bacterial infection; bacterial colonization should not be treated.
Antibiotics are usually administered orally, parenterally, or topically. Parenteral antibiotic therapy is warranted when there is extensive soft tissue involvement, systemic symptoms, rapid progression of clinical manifestations, and persistent or progression of symptoms after 48 to 72 hours of oral therapy. Parenteral antibiotics can be administered without difficulties in inpatient settings and can be administered at home with home healthcare or at outpatient infusion centers. Consider drug interactions, because some antibiotics can alter the levels and effects of concomitant medications.
Antibiotics are grouped into classes based on structures and mechanisms of actions. The spectrum of antibiotics commonly used in wound care is summarized in Table 3.
Table 3 - ANTIBACTERIAL SPECTRA OF ANTIBIOTICS COMMONLY USED IN WOUND CARE SETTINGSa Pathogen Amoxycillin and Clavulanate First-Generation Cephalosporin Clindamycin TMP-SMX Doxycycline Ciprofloxacin Levofloxacin Metronidazole Linezolid β-Hemolytic Streptococcus + + + +/− 0 0 +/− 0 + MSSA + + + + + 0 + 0 + MRSA 0 0 +/− + + 0 0 0 + CoNS +/− +/− +/− + + 0 +/− 0 + Enterococcus faecalis + 0 0 0 +/− 0 + 0 + Enterococcus faecium +/− 0 0 0 +/− 0 0 0 + Pseudomonas aeruginosa 0 0 0 0 0 + + 0 0 Enterobacterales +/− 0b 0 +/− +/− + + 0 0 Anaerobes + 0 + 0 +/− 0 0 + 0Abbreviations: CoNS, coagulase-negative staphylococci; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus; TMP-SMX, trimethoprim-sulfamethoxazole.
+: active most of the time; +/−: variable; 0: not recommended.
aRefer to local antibiogram because resistance can vary.
bFirst-generation cephalosporin can be used when it is shown as susceptible in culture results. However, it is not used frequently because it is not commonly included in antimicrobial susceptibility panels.
Penicillin G was one of the first antibiotics developed and is still one of the most widely used. Penicillins, cephalosporins, carbapenems, and monobactams all contain a β-lactam ring that gives these antibiotics their classification (β-lactams) and antibacterial activity. The β-lactam ring inhibits bacterial enzymes, called penicillin-binding proteins, which are responsible for synthesizing the peptidoglycan layer of bacterial cell walls, resulting in cell lysis. In addition to the naturally derived penicillin G, there are many semisynthetic derivatives of this compound that share the same penicillin core structure. These semisynthetic penicillins can be classified into antistaphylococcal penicillins, broad-spectrum penicillins, and antipseudomonal penicillins. Although penicillin G is active against most Streptococcus species, some Enterococcus species, and some anaerobes, it is not common in the wound care setting because of its narrow spectrum and need for frequent administration. Antistaphylococcal penicillins (nafcillin, oxacillin, and dicloxacillin) are active against MSSA because of decreased susceptibility to penicillinases produced by Staphylococcus. Broad-spectrum penicillins (amoxicillin, ampicillin) are distinguished by their activity against Gram-negative rods. Clavulanate potassium is frequently given with amoxicillin to inhibit enzymes, called β-lactamases, which confer resistance to amoxicillin and other β-lactam antibiotics. Amoxicillin/clavulanate is commonly prescribed in wound care settings because of its broad-spectrum coverage including Gram-positive cocci, Gram-negative rods, and anaerobes. Although up to 10% of patients report penicillin allergy, more than 90% of patients with a reported penicillin allergy do not have immunoglobulin E-mediated hypersensitivity.21 Obtaining detailed allergy history, including the timing and type of reaction against penicillin, is very important when a penicillin-class agent is ideal based on wound culture results but the patient self-reports a penicillin allergy.
CephalosporinCephalosporins are frequently used both in outpatient and inpatient settings because of their broad-spectrum coverage and few adverse effects. As with penicillins, cephalosporins share the β-lactam ring but differ in the adjacent ring structure and side chains. Cephalosporins are grouped into generations based on their spectrum of activity, and the later generations are characterized by their expanded aerobic Gram-negative bacilli coverage. The first-generation cephalosporins are effective against Gram-positive organisms except for Enterococcus species (which have intrinsic resistance to all cephalosporins) and some Gram-negative rods. Oral first-generation cephalosporins (eg, cephalexin, cefadroxil) are commonly used for uncomplicated skin and soft tissue infections typically caused by Staphylococcus and Streptococcus. Higher generations generally have expanded spectra against aerobic Gram-negative bacilli. Second-generation cephalosporins (eg, cefuroxime) have similar activity against Gram-positive cocci as the first-generation and have expanded coverage for certain Gram-negative organisms and anaerobes. Third-generation cephalosporins (eg, ceftriaxone, ceftazidime) cover additional Gram-negative rods that do not produce AmpC β-lactamase or ESBL, including E coli, K pneumoniae, and P mirabilis. Ceftazidime (third generation) and cefepime (fourth generation) provide Pseudomonas coverage. Many newer cephalosporins do not fit neatly into the generation scheme but are occasionally described as fifth-generation cephalosporins, such as ceftaroline, which exhibits activity against MRSA (which is resistant to all other cephalosporins). Siderophore cephalosporins, currently limited to cefiderocol, and those combined with β-lactamase inhibitors, namely, ceftolozane-tazobactam and ceftazidime-avibactam, are active against multidrug-resistant Gram-negative rods such as multidrug-resistant Pseudomonas species and carbapenem-resistant Enterobacterales. These higher-generation cephalosporins are administered intravenously, and infectious disease consultation is recommended for antimicrobial management of infections due to multidrug-resistant organisms. Allergic cross-reactivity between cephalosporins and penicillins is low; previous studies reported only 0% to 8.1% of patients who reported penicillin allergies reacted to cephalosporin.22,23
ClindamycinClindamycin is a lincosamide antibiotic that inhibits protein synthesis by reversibly binding to the 50S ribosomal subunit. It is well absorbed after oral administration, and it penetrates well into bone. Clindamycin is commonly used for uncomplicated skin and soft tissue infections because it is active against many Streptococcus species, including some S aureus isolates and anaerobes, but lacks activity against Enterococcus and Enterobacterales because of intrinsic resistance. Clindamycin resistance among S aureus, especially MRSA, has been increasing, and approximately 40% of S aureus isolates were resistant to clindamycin in 2017.24 Prevalence of resistance can vary locally, and susceptibility needs to be assessed for individual isolates, especially when patients are not improving with empiric clindamycin. One major disadvantage is that clindamycin is highly associated with Clostridioides (formerly Clostridium) difficile colitis.
Trimethoprim-sulfamethoxazoleTrimethoprim-sulfamethoxazole (TMP-SMX) is a combination of two antimicrobial agents that act synergistically in the bacterial synthesis of tetrahydrofolic acid, a precursor to the synthesis of DNA. Similar to clindamycin, it has good absorption and penetrates well into bone.25 In addition, TMP-SMX is active against a wide variety of aerobic Gram-positive cocci and Gram-negative rods. It can also be used for polymicrobial infections, either as monotherapy or as part of a combination therapy, depending on the susceptibilities. Because it retains activity against most MSSA and MRSA isolates, TMP-SMX is an important oral antibiotic to treat S aureus in wound care settings. However, it is not active against Streptococcus species, P aeruginosa, or anaerobes. Although TMP-SMX works against a wide variety of bacteria, resistance has developed in most bacterial species. It is generally well tolerated but rarely can cause life-threatening adverse effects including hyperkalemia (due to blockade of the collecting tubule sodium channel by trimethoprim26), Stevens-Johnson syndrome, and blood dyscrasias; TMP-SMX is contraindicated in pregnancy.
TetracyclinesTetracyclines (eg, tetracycline, doxycycline, minocycline, omadacycline) inhibit protein synthesis by binding reversibly to the 30S ribosomal subunit. These agents achieve high concentrations in the tissues, which is helpful in wound, bone, and joint infections. They are well absorbed after oral administration and penetrate well into bone.25 Doxycycline is prescribed the most frequently among the tetracyclines. Omadacycline was approved in 2018, and it exhibits expanded activity compared with older agents, including certain Streptococcus and VRE. Tetracyclines provide broad-spectrum coverage against many aerobic Gram-positive and Gram-negative bacteria in addition to many atypical pathogens, such as zoonotic pathogens. Most S aureus are susceptible to tetracyclines, including MRSA. Gram-negative rods, including ESBL-producing organisms, can also be treated with tetracyclines when cultures show they are susceptible. Tetracyclines (excluding omadacycline) do not have appreciable activity against S agalactiae, S pyogenes, or anaerobes, and all agents are inactive against P aeruginosa. Tetracyclines are generally safe, but some adverse effects such as dose-related gastrointestinal symptoms can occur. Tetracyclines are often contraindicated in pregnant individuals and children younger than 8 years because of permanent yellowing of teeth and bone growth inhibition.
FluoroquinolonesFluoroquinolones (eg, ciprofloxacin, levofloxacin, moxifloxacin, delafloxacin) directly inhibit bacterial DNA synthesis;27 they have high oral bioavailability and adequate bone penetration.25 Fluoroquinolones offer broad-spectrum Gram-negative bacilli coverage and, with the exception of moxifloxacin, are the only oral antibiotics that have antipseudomonal activity. Ciprofloxacin lacks reliable activity against Streptococcus species compared with the other agents. Delafloxacin, the newest fluoroquinolone, is active against MRSA, some strains of CoNS, and streptococci. It was approved in 2017 by the US FDA for treatment of bacterial skin and soft tissue infections.28 Moxifloxacin and delafloxacin additionally provide anaerobic coverage. The potentially severe adverse effects include C difficile colitis, tendon rupture, QT interval prolongation, altered mental status, and putative aortic dissection and rupture.29,30 Fluoroquinolones are generally contraindicated in pregnant or nursing individuals and children because of the potential for skeletal abnormalities.
MetronidazoleMetronidazole destabilizes bacterial DNA structure, ultimately inhibiting protein synthesis. It continues to be one of the mainstay drugs for treatment of infections due to anaerobes, including Bacteroides, Prevotella, Clostridium, and Peptostreptococcus species. Although susceptibility testing for anaerobic bacteria is not routinely performed, acquired resistance to metronidazole among anaerobic bacteria is very rare.31 Because of its limited coverage, it should be combined with other antibiotics that are active against aerobic bacteria when it is administered empirically. Common adverse effects include gastrointestinal symptoms, metallic taste, and peripheral neuropathy.
OxazolidinonesLinezolid and tedizolid are synthetic oxazolidinones that inhibit bacterial protein synthesis by binding to the 50S ribosomal subunit. These exhibit bacteriostatic activity exclusively against Gram-positive organisms including Streptococcus, Enterococcus (including VRE), CoNS, MSSA, and MRSA.32 Linezolid and vancomycin have equivalent clinical cure rates for MRSA infections, including skin and soft tissue infections.33,34 Tedizolid is noninferior to linezolid for the treatment of skin and soft tissue infections.32 Because both have excellent bioavailability, the oral forms can be administered for patients who did not improve with conventional oral antibiotics but are stable enough to stay as outpatients. Linezolid should be used with caution or avoided in patients who take selective serotonin reuptake inhibitors for depression because of the increased risk of serotonin syndrome. Thrombocytopenia and anemia have been reported with the use of linezolid, which typically occurs with 2 weeks or longer duration of therapy.35 Use of these antibiotics may be limited by cost.
Glycopeptides and lipoglycopeptidesVancomycin, a glycopeptide, and dalbavancin and oritavancin, both lipoglycopeptides, inhibit cell wall synthesis and disrupt cell membrane permeability.36,37 All agents are administered parenterally and active against Gram-positive organisms including MRSA. Vancomycin is the main parental agent for MRSA infection, and it is frequently administered for inpatients with skin and soft tissue infection. In outpatient settings, vancomycin can be administered through a peripherally inserted central catheter at outpatient infusion centers or at home by home health nurses. Both dalbavancin and oritavancin are noninferior to vancomycin or linezolid for the treatment of skin and soft tissue infection.38,39 They are long-acting parenteral agents: dalbavancin has a half-life of 14 days, and oritavancin has a half-life of 10 days. They can be administered as a single dose through peripheral lines in the ED, at outpatient infusion centers, or at home by home health nurses. Although they are convenient and enable patients whose infections warrant parenteral therapy but do not otherwise require inpatient management to avoid hospital admission, the medication cost and insurance preauthorization process can be challenging.
DURATION OF ANTIBIOTIC TREATMENTClinicians should optimize antibiotic usage by using agents with the narrowest spectrum of activity and for the shortest duration to prevent the development of multidrug resistance or adverse effects. Duration of antibiotic treatment mainly depends on the extent and severity of the infection, host factors, and the causative organisms. Generally, antibiotic durations of 1 to 2 weeks for mild soft tissue infections, 2 to 3 weeks for moderate to severe soft tissue infections,11 and 6 weeks for osteomyelitis are recommended.8 Suggested empiric antibiotic regimens for wound infections are summarized in Table 4.11,40 The empiric regimen should be de-escalated once culture results are obtained.
Table 4 - SUGGESTED EMPIRIC ANTIBIOTIC REGIMENS FOR WOUND INFECTIONS Type of Infection Empiric Oral Antibiotic Regimen Boils, furuncles, abscesses 1. TMP-SMXAbbreviations: MRSA, methicillin-resistant Staphylococcus aureus; TMP-SMX, trimethoprim-sulfamethoxazole.
Whereas all chronic wounds are considered to be colonized, not all are infected. Understanding wound infection stages and closely examining chronic wounds are critical to assess whether a chronic wound is colonized or infected. Once infection is suspected, collect specimens for culture using proper techniques to avoid contamination to guide antimicrobial treatment.
Going back to the case study, a tissue culture was obtained with a 7 mm dermal curette after wound debridement and cleaning with normal saline, which grew extended spectrum β-lactamase producing Klebsiella oxytoca. Based on the susceptibility, ciprofloxacin 500 mg twice a day was started. Cadexomer iodine gel was applied daily after wound cleansing. Electric wheelchair use was continued. Her wound was closed in 30 days after the first wound clinic visit.
PRACTICE PEARLSAll chronic wounds are colonized with microbes; however, it does not mean they are infected. The wound infection continuum begins with contamination, colonization, and critical colonization and can progress to infection if not treated properly. Several host resistant fa
留言 (0)