
記住我
Venous ulcers are the most common type of leg ulcers,1 and the incidence of venous insufficiency and ulcers increases with age.1 Between 1% and 22% of the population older than 60 years experiences venous ulceration.2 It is common for a person with a venous ulcer to be admitted to an acute care setting. However, this many interrupt the plan of care if the patient is receiving care for the venous ulcer from another provider. Standard care for venous ulcers is multicomponent compression wraps.3 Below is a case with answers to the dilemmas of care during hospitalization.
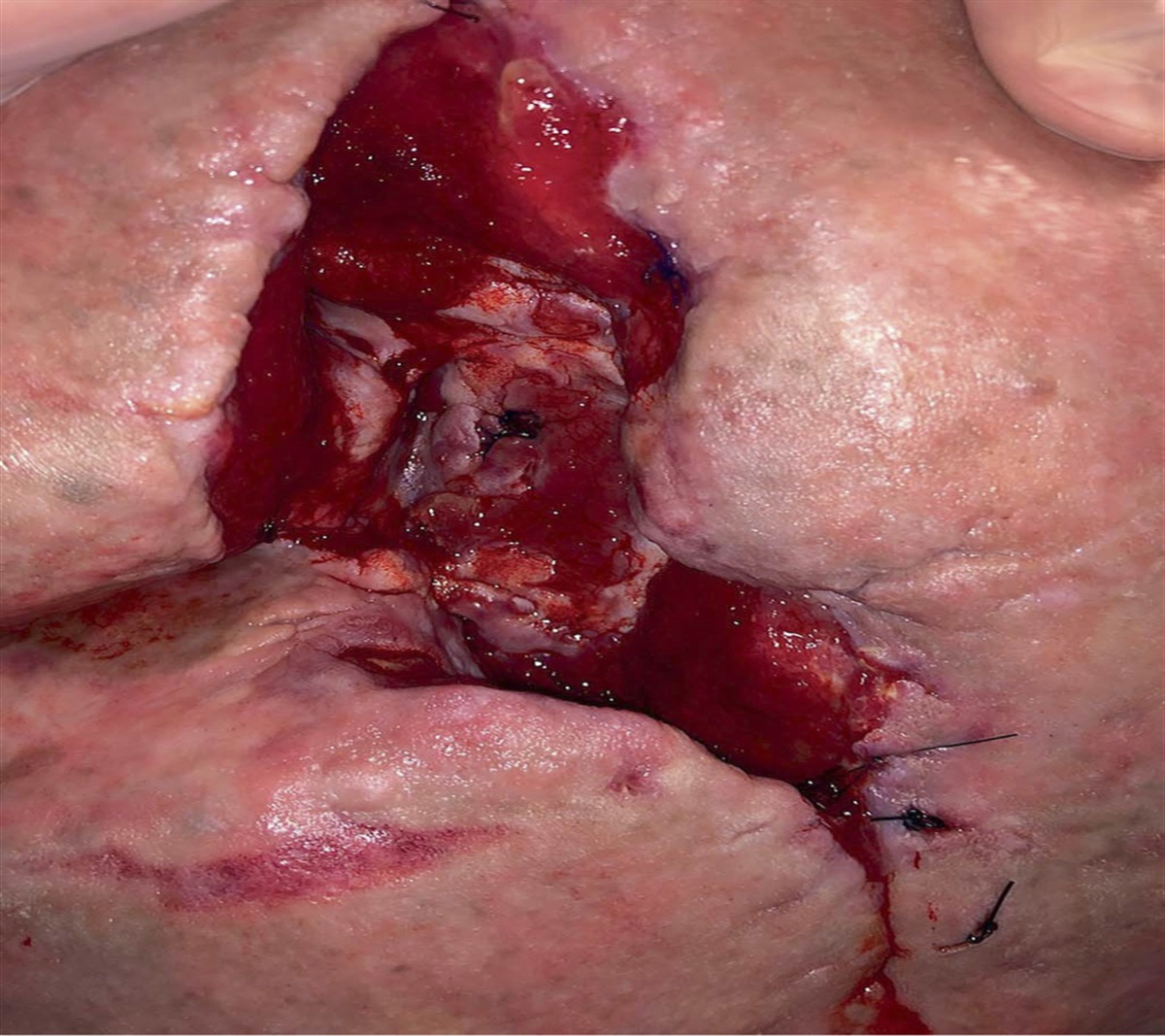
CASE STUDYA 70-year-old man with shortness of breath is hospitalized for uncompensated heart failure. The patient had a job for 40 years that required standing; he retired 2 years ago and falls asleep in a chair with his legs dependent while watching TV. His history includes hypertension and obesity (280 lb). He quit smoking cigarettes 10 years ago, drinks a 12-oz beer daily, and has not used injected drugs. While doing the intake assessment, the nurse notes a thick compression dressing on his left lower extremity. The patient explains, “I hit my leg on the corner of the bed 3 months ago and attend a wound clinic by my house.” He states he was told it is a venous ulcer, and he goes weekly to get the dressing changed. The current dressing was applied 3 days ago (Figure).
 Figure:
Figure: THE PATIENT’S DRESSINGEdwards H, Courtney M, Chang AM, Finlayson K, Gibb M, Parker C. Promoting healthy skin: a self-directed learning resource for residential aged care workers. Web-based interactive DVD. Brisbane, Australia: Queensland University of Technology; 2010.
Dilemma: Should the Dressing Be Removed?There may be hesitancy on the part of the patient or the nurse to remove a compression wrap, particularly because the dressing is complex and may require a specialist for reapplication. But the dressing must be removed for thorough wound assessment upon admission. The venous ulcer is often not the primary concern for practitioners managing the patient during hospitalization but must be assessed and managed.
CASE STUDY, CONTINUEDThe nurse removes the dressing. The ulcer is on the medial malleolus and 3.0 × 3.0 × 0.2 cm in size with a clean, pink base. It has marked serous drainage, no odor, and no surrounding warmth or erythema; the patient reports slight pain. Bilateral lower extremities are edematous and discolored. The patient reports that the edema decreases at night and increases during the day. Dorsalis pedis and posterior tibial pulses are strong. Lower extremities are warm to palpation.
Dilemma: How Should This Wound Be Redressed?Venous ulcer guidelines can help with care decisions.3 Because the wound base is clean (ie, free of necrotic tissue or debris) and without indication of infection (eg, foul odor, surrounding warmth, or erythema) but with drainage, a nonstick, absorptive dressing such as alginate should be applied. Silver is not beneficial for venous ulcers without indications of infection.1–3 Use of honey has not resulted in significant improvement in venous ulcers.1,2 The provider should treat the surrounding skin of the lower extremities with emollients, but avoid open wounds and the areas between toes.1
Dilemma: Should Compression Wraps Be Applied?Before applying any type of compression to the lower extremities, the clinician should consider comorbidities including arterial disease, diabetes, and congestive heart failure. External compression when arterial insufficiency is present (ankle brachial index [ABI] <0.8) can further impair circulation to the extremity.1,4 Diabetes can affect arterial studies because of arterial calcification, resulting in falsely elevated, less reliable ABI values. Further evaluation is indicated in the case of ABI >1.30 or <0.90.5 The provider should consider the patient’s tolerance of the extra fluid load from heart failure that can result from the fluid shift if compression is applied. The type of compression dressing used would depend on the products available in the agency and the level of compression prescribed.
CASE STUDY, CONTINUEDThe nurse finds in the electronic medical record that the patient’s most recent ABI from Doppler studies 2 months prior was 1.0, and the patient’s medical history does not include diabetes mellitus. However, because the patient is undergoing workup for uncompensated congestive heart failure, his providers decide not to apply compression to the lower legs. Once his heart failure is controlled, compression therapy prior to discharge is reevaluated. Individualized compression therapy will be continued on an outpatient basis.
Dilemma: Whom Should the Nurse Contact About This Wound?The attending physician needs to be notified of the wound. A wound care specialist can be consulted to make recommendations for wound management while the patient is hospitalized.4
Dilemma: Should the Patient Be Allowed to Sit in a Chair?Hospitalization can provide an opportunity for interventions that may markedly improve the wound. Improvement in venous ulcers is often noted as related to the lower extremity elevation that comes with time spent in bed during hospitalization. While at rest, the patient’s lower extremities should be elevated.2
When the patient sits in a chair, he should have a stool and pillow so that his lower legs are elevated and not dependent. Safety must always be considered: the person positioned with both legs elevated needs to be able to easily call for help, so the call device should be located within reach.
Dilemma: What Else Should the Nurse Consider Related to the Patient’s Venous Ulcer?Because obesity is a contributing factor to venous insufficiency and ulceration,3,4 the dietitian should be consulted for a nutrition assessment to optimize nutrition for wound healing and, ultimately, for weight-loss planning. Physical and occupational therapists should be consulted to teach calf muscle pump exercises and provide mobility aids. Patients and families should be educated as to what chronic venous insufficiency and venous ulcers are, the lifelong need of care to prevent recurrence, the importance of compression, the need for lower extremity elevation, the need to sleep in bed versus a recliner, importance of leg exercises, and so on.1,2,4,5 Needless to say, the patient’s learning and involvement in care may be affected by his/her interest and motivation, family involvement, home setting, and finances, to name just a few additional factors. A home care nurse referral can ensure continuation of the assessments and education that began during hospitalization.
IMPLEMENTATION OUTCOMESCompression and lower extremity elevation are mainstays of venous ulcer therapy that should be considered in the acute care setting. Compression wraps should be removed for assessment and management while a patient is in acute care despite the special training that is required for application. Comorbidities, including arterial disease, diabetes, and congestive heart failure, should be considered before resuming compression therapy. REFERENCES 1. SIGN Network. SIGN guideline 120: management of chronic venous leg ulcers. https://www.nhstaysideadtc.scot.nhs.uk/wound%20Formulary/Pdf%20docs/sign120%202010.pdf. Last accessed August 3, 2022. 2. Sieggreen MY, Niezgoda JA, Smart H, Siddique A. Venous disease and ulcers. In Baranoski S, Ayello EA, eds. Wound Care Essentials—Practice Principles. 5th ed. Philadelphia, PA: Wolters Kluwer; 2020. 3. Tang JC, Marston WA, Kirsner RS. Wound Healing Society (WHS) venous ulcer treatment guidelines: what’s new in five years?Wound Repair Regen 2012;20:619–37. 4. American Academy of Wound Care (AAWC). International Consolidated Venous Ulcer Guideline (ICVUG) updated 2015. https://aawconline.memberclicks.net/assets/appendix%20c%20guideline%20icvug-textformatrecommendations-final%20v42%20changessaved18aug17.pdf. Last accessed August 3, 2022. 5. British Columbia Provincial Nursing Skin and Wound Committee. Guideline: application of compression therapy to manage venous insufficiency & mixed venous/arterial insufficiency. 2016. https://www.clwk.ca/buddydrive/file/guideline-compression-therapy-final-2016-may/. Last accessed August 3, 2022.
留言 (0)