
記住我
As the UK enters lockdown for the third time in the space of 9 months, it seems timely for ophthalmologists and more specifically glaucoma specialists to examine the effect that the COVID-19 pandemic is having on local surgical practice.
We are faced with the challenge of attempting to minimise irreversible sight loss due to treatment delays while being mindful that the process of attending a healthcare facility increases the risk of COVID-19 infection for the patient, their family members and other close contacts.1
The first UK lockdown was announced on 16 March 2020. Initially all face-to-face clinic appointments and elective ophthalmology surgeries were cancelled by some units. National lockdowns have subsequently been announced in November 2020 and January 2021.
Many glaucoma laser and surgical procedures have been suspended in cases where there is no urgent threat of vision loss; however, reduced numbers of urgent procedures have been necessary.1
Current guidelines from the Royal College of Ophthalmologists (RCOphth) provide general guidance regarding consideration of surgery only in patients at risk of vision loss due to delays. These guidelines also give recommendations on the process of preparing patients for theatre (such as preoperative testing and isolation periods), as well as day of surgery protocols such as face masks for patients, personal protective equipment (PPE) for staff, reduction of staff in theatre, minimisation of general anaesthesia and air exchange periods for cases requiring the latter.1 Tejwani et al 2 have published guidelines to assist glaucoma doctors in India in continuing to practise and treat patients with glaucoma responsibly and safely. Recommendations were made to avoid general anaesthesia if possible and for procedures requiring less postoperative care to be favoured at the discretion of the surgeon; however, there was little specific guidance for glaucoma surgery.2
The choice of surgical procedure and of anaesthetic is still largely the domain of the operating surgeon, and the impetus for the current survey was to achieve some insight into the changes in surgical practice adopted by glaucoma specialists in the UK as a result of the COVID-19 pandemic. Such information provides valuable insights into the current state of practice among specialists in the field as well as forms a basis for examining the extent to which the pandemic may result in permanent changes to practice. This report may also help clinical leads, consultants, directors and managers of hospital ophthalmic services to plan patient care during the recovery phase and provide an insight into what the ‘new normal’ may look like. It will also assist national and regional National Health Service bodies to provide guidance regarding service delivery.
AimThe aim of the study was to quantify, describe and evaluate primary glaucoma surgical practices in the UK both before and after the COVID-19 pandemic. In particular, information regarding preferences in established/traditional glaucoma surgery, adoption of minimally invasive glaucoma surgery (MIGS) procedures and choice of anaesthesia was sought, as well as changes to such practices subsequent to the pandemic.
ResultsRespondents‘ demographicsA total of 70 UKEGS glaucoma specialists completed the survey. Consultants’ years of experience are presented in table 1. Forty-one (59%) respondents had 10 years or less of consultant experience and 21 (30%) respondents had been practising at a consultant level for 5 years or less. A total of 65 (93%) respondents had undergone formal glaucoma fellowship training. Collectively, respondents were representative of the whole of the UK. Areas of greatest representation included consultants who identified as practising in the South East (23%), North West (21%) and South West (17%) of the UK. Each of the Scottish and Northern Irish categories contributed 6% of overall responses.
Table 1Years practising as a consultant ophthalmologist
Glaucoma surgery practices (pre-COVID-19)Participants were asked to report their preferred ‘established’ (non-MIGS) glaucoma procedure for primary open angle glaucoma (POAG) before COVID-19. The results are presented in figure 1. Trabeculectomy was the procedure of choice for 61 (87%) glaucoma specialists.
 Figure 1
Figure 1 Preferred ‘established’ (non-MIGS) glaucoma procedure for primary open angle glaucoma ‘pre-COVID-19’. GDD, glaucoma drainage device; MIGS, minimally invasive glaucoma surgery.
A total of 51 (73%) respondents reported performing MIGS procedures before COVID-19. The types of MIGS procedures performed by respondents in the 12 months before COVID-19 are presented in figure 2. The most commonly performed MIGS procedure was the iStent inject (51%), followed by XEN 45 (36%) and Preserflo (17%). The adoption of MIGS prior to COVID-19 was also analysed according to years of consultant-level experience, and the results are displayed in table 2.
Table 2Adoption of MIGS prior to COVID-19 according to experience
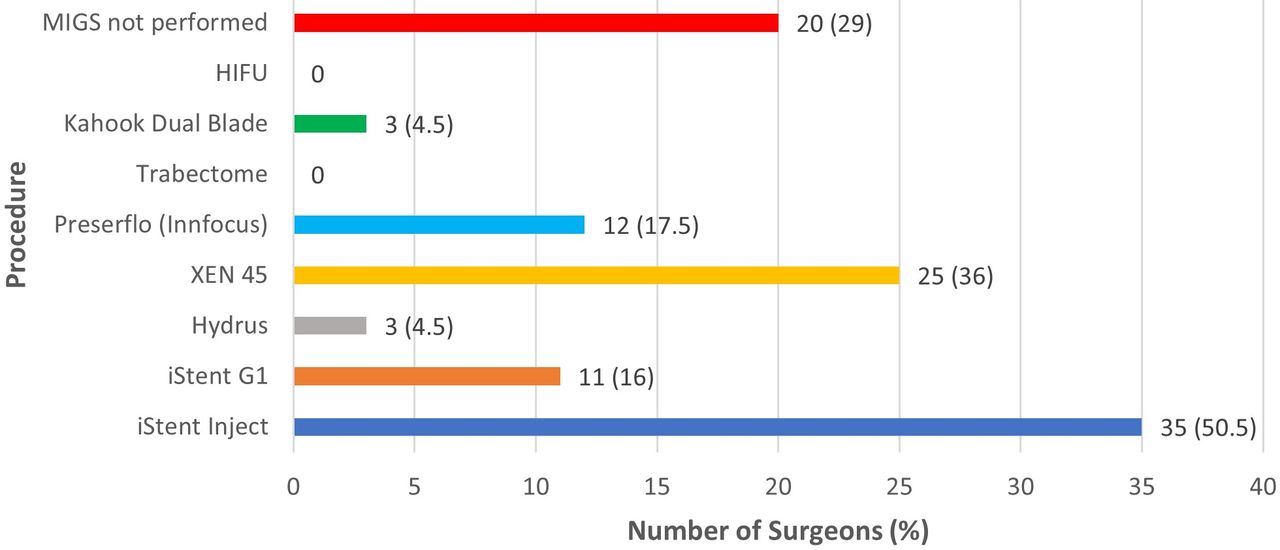 Figure 2
Figure 2 MIGS procedures performed in the 12 months preceding COVID-19. HIFU, high-intensity focused ultrasound cyclophotocoagulation; MIGS, minimally invasive glaucoma surgery.
Choice of anaesthesia (pre-COVID-19 and post-COVID-19)The most common choice of anaesthesia for respondents’ established glaucoma surgery of choice before COVID-19 was a sub-Tenon’s block without sedation, identified by 33 (47%) respondents. General anaesthesia was preferred by six (8%) respondents. When questioned regarding COVID-19-related changes to their preferred type of anaesthesia, 49 (72%) respondents reported no change, whereas 15 (22%) respondents reported changing to predominantly using local anaesthetic without sedation.
Opinion regarding glaucoma surgery as an aerosol-generating procedureStand-alone glaucoma surgery was considered an aerosol-generating procedure (AGP) by only five (7%) respondents. When asked to nominate which procedures were considered aerosol-generating, four respondents identified trabeculectomy and one respondent identified glaucoma drainage devices (GDDs).
Glaucoma surgery practices (post-COVID-19)Forty-three (61%) respondents reported modifying their glaucoma surgery practice subsequent to the onset of the COVID-19 pandemic. Of the glaucoma specialists who modified their surgical practices, 21 (43%) specifically reduced the number of trabeculectomies performed; GDD (n=5, 11%) and MIGS (n=3, 7%) were also reduced by a smaller number of surgeons.
Respondents who reported changing their glaucoma surgery practice were asked if alternative procedures were selected, and the results are fully displayed in table 3. In combination, diode laser (both micropulse and conventional trans-scleral cyclodiode) was the most common alternative procedure and was chosen by nine (21%) respondents.
Table 3Changes in surgical procedure post-COVID-19
Patterns of change in glaucoma practice were analysed according to years of consultant experience. The results are demonstrated in table 4.
Table 4Patterns of change in glaucoma surgery practice according to consultant experience
Reasoning behind change in type of procedureRespondents were asked to indicate their reasoning for changing the type of glaucoma procedure performed, and the results are detailed in table 5. Less postoperative follow-up was the reason given for change by 26 (90%) respondents. Less postoperative interventions (n=18, 62%), shorter surgical time (n=14, 48%), improved safety (n=10, 35%) and anaesthetic concerns (9=31%) were also commonly reported reasons for change. Respondents were questioned regarding the anticipated impact of any surgical choice changes on future practice patterns. The type of surgical procedure offered as first line for POAG had not changed for 32 (46%) respondents, and 15 (22%) respondents did not anticipate any future long-term change to practice despite changing during the COVID-19 pandemic. Some adoption of changes in practice in the post-COVID-19 period was anticipated by 22 (32%) respondents, with 2 (3%) respondents anticipating a complete adoption of COVID-19 influenced surgical choices.
Table 5Reasoning behind change in type of procedure
DiscussionThe primary aim of this survey was to obtain an insight into the choice of glaucoma surgical procedures and anaesthesia during the COVID-19 pandemic and how this may have modified the way we view these options, both now and beyond into the future. The RCOphth has provided guidance for surgical decision-making throughout this pandemic. These guidelines, however, are not prescriptive in recommending particular surgical procedures over others and nor would one expect them to do so. We therefore felt it was both interesting and important to determine the real-world influence that the pandemic has had on national surgical decision-making.
Seventy UK-based glaucoma subspecialist consultants participated in the survey. This represents a large number of glaucoma surgeons across the UK, with a widespread and proportionate distribution across all the home countries. There was also a relatively even spread of experience related to time in a consultant post, which was important in teasing out experience-related differences in choices.
The majority of respondents (87%) identified trabeculectomy as their preferred ‘established’ glaucoma procedure for POAG before COVID-19. This is not surprising and reflects current evidence of glaucoma surgical preferences in the literature.3 The smaller number of surgeons identifying non-penetrating glaucoma surgery (NPGS) is likely to represent the fact that less UK glaucoma specialists are trained in this surgical approach, with the larger North West proportion of NPGS respondents reflecting this. A large proportion of respondents (73%) also reported performing MIGS procedures as part of their glaucoma armamentarium (although not as the ‘primary established’ procedure) in the pre-COVID-19 period, with the iStent inject (51%), XEN 45 (36%), Preserflo (17%) and iStent G1 (16%) being the most adopted procedures. Duration of availability, surgical learning curve and the ease with which a particular MIGS procedure can be combined with phacoemulsification surgery are likely to have influenced the trend in MIGS surgery. This in itself is an interesting snapshot of how glaucoma surgery has evolved over the last decade, with a propensity to add a myriad of newer surgical options which are many times grouped together under the generalised heading ‘minimally invasive glaucoma surgery (MIGS)’. Specialists with 0–5 years of consultant experience had a very high (95%) adoption rate of MIGS, while the adoption of MIGS by specialists with more years of consultant experience, 16–20 years or >20 years, was lower (50% and 42%, respectively). This demonstrates a greater likelihood for consultants with fewer years of experience to include MIGS in their surgical algorithms. One possible reason for this is the comfort with which an experienced surgeon may be able to reproduce a traditional glaucoma operation without early postoperative complications. There are, however, several potential reasons for this observation which are beyond the scope of this study to discuss.
Type of anaesthesia was cited as one reason for changing the type of surgery performed post-COVID-19. The increased risk of COVID-19 transmission during administration of general anaesthesia has been well documented.4 Glaucoma procedures are often performed under local anaesthesia; therefore, 72% of respondents reported no change in choice of anaesthesia and 22% of respondents reported changing to predominantly local anaesthesia without sedation. Both the desire to reduce the number of cases performed under general anaesthesia and the reduced availability of anaesthetists are likely to have explained this observation.
The extent to which any particular glaucoma surgery may be aerosol-generating is still a point of contention. Only 7% of our respondents considered stand-alone glaucoma surgeries as aerosol-generating procedures. The concern seemed to be during the washout of mitomycin C during trabeculectomy or GDD surgery. Experimental intraocular models have been used to investigate aerosol generation by intraocular procedures such as phacoemulsification and vitrectomy but not for glaucoma procedures, and there is still no current consensus about any ocular surgery and potentially infective aerosol generation.4 5 Although adnexal and lacrimal procedures can generate infective aerosols, the risks involved with intraocular surgery are less clear. Instruments with fast-moving parts such as phacoemulsification probes and vitrectors generate aerosols, and the RCOphth has recommended full PPE where possible. It has not been established however that such aerosols are actually infective. Similarly, viral loads are known to be low in tears and conjunctiva, even in infected patients, and hence sprays generated from the ocular surface are considered by some as a possible risk, although this has not been proven.6
Forty-three (61%) respondents reported modifying their glaucoma surgery practices following the onset of the COVID-19 pandemic, with 21 (43%) of these having stopped altogether or reduced the number of trabeculectomies. The frequency of GDDs and MIGS was also decreased to a lesser degree by 11% and 7% of respondents, respectively. In cases where procedures were changed, the alternative was most likely to be trans-scleral micropulse diode (14%), GDDs (12%), cyclodiode (7%), deep sclerectomy (7%) and/or Preserflo (7%). Reasons for choosing one substitute over another varied on a case-by-case basis, but the proportion of specialists changing surgical choices was quite similar between the groups with different levels of consultant experience. This was also the case for decisions to reduce or restrict the number of trabeculectomies performed. The overarching reason given by our respondents for changing the type of glaucoma surgery was the desire for less overall patient contact in order to reduce the risk of COVID-19 transmission. A push for less postoperative follow-up (90% of respondents) and less postsurgical interventions (62% of respondents) was the main drive for shifting away from trabeculectomy. It is possible that less MIGS procedures were being performed by some surgeons due to suspension of less urgent surgical interventions and a reduction in cataract operations with which MIGS procedures are often combined. A shift towards conventional trans-scleral and micropulse diode procedures is understandable given the reduced levels of postprocedural care required; however, it would be interesting to see if these procedures, particularly micropulse diode, have produced a sustained intraocular pressure-lowering effect beyond 6 months or whether they have instead acted more as a temporising measure.7 Also of interest will be the long-term efficacy of devices such as the Preserflo, for which there is emerging encouraging data but of which the longer-term efficacy and potential adverse effects remain unknown.8 Based on the latter point, one can argue whether consideration should be given to increased training and adoption of NPGS, which has a proven track record along with the advantage of reduced postoperative reviews and manipulation compared with trabeculectomy.9–11 NPGS does have a steeper learning curve when compared with MIGS however and would be understandably difficult to adopt in a short time frame, such as that induced by the COVID-19 pandemic.
From late February 2020, Italy (particularly Lombardy) was severely affected by COVID-19.12 Quaranta et al 12 have since published their protocols and surgical experience during this period. Acting as a tertiary referral centre they found that the number of glaucoma procedures performed was actually higher than for the same period the previous year due to service closures in suburban hospitals.12 The prevailing restriction measures on the hospital and the desire to simplify postoperative care had a significant impact on the type of surgery offered. Similar to our findings, trabeculectomies were undertaken less often in favour of Preserflo, XEN and NPGS.12 It was interesting that only one tube shunt (Ahmed valve) was performed during the lockdown, which was equal to the same period in the preceding year, suggesting that tubes were not a common surgical choice in this centre. In our survey GDDs were a common substitute for trabeculectomy, mainly as an attempt by several respondents to reduce postoperative visits and interventions. Two respondents also reported reducing the number of Baerveldt tube surgeries with a preference for the newer Paul tube, which drains from postoperative day 1 and possibly carries a lower risk of early postoperative complications.13
All challenges represent an opportunity for change. As suggested by Liebmann,14 COVID-19 has necessitated a change in our models of care. There was a predicted shift in surgical choice in the direction of cyclodiode, GDD and minimally invasive procedures rather than trabeculectomy due to the intensive postoperative care with the latter.14 Although 46% of our respondents did not change their choice of preferred glaucoma procedure during the COVID-19 pandemic and a further 22% did not anticipate such changes would be adopted in the long term, around a third of respondents predicted a permanent change in surgical options and decision-making as a result of the pandemic, which is considerable.
It will be interesting to see if some of the practice changes in general can result in more effective and efficient delivery of glaucoma care. Prior to COVID-19 ophthalmology services were under considerable pressure with clinical and surgical backlogs increasing. Ironically, changes to delivery of care could become easier to implement now that COVID-19 has necessitated change. Virtual clinics, phone consultations, telemedicine and better utilisation of primary care optometrists are assuming greater roles and this will likely be maintained.
Considerations of changing the surgical procedure itself is only one adaptation that forms part of a much larger response. Nonetheless, if such times do result in changes to the surgical procedures offered, it is of great interest to first assess the nature of these changes and then possibly, at a later time, assess outcomes in circumstances where the surgery offered would have been different. An obvious immediate benefit on changes to surgical procedure is the reduced footfall through glaucoma clinics, resulting in less service demands on glaucoma departments as well as less risk of COVID-19 transmission until vaccination rates in the broader public are sufficiently high.
LimitationsThe target group for our survey were ophthalmologists within the UK who identified themselves as glaucoma specialists. For this reason, the number of respondents was, by nature of the design of the survey, relatively small. The confidence intervals of the averages are therefore wide, and this is amplified by the inherent inaccuracies of research based on surveys. There are also some inconsistencies regarding which surgical procedures should be categorised as MIGS procedures, such as Preserflo not being considered as ‘minimally invasive’ by all respondents. With respect to the design of the survey itself, the available options for answers at times allowed for inconsistent responses, such as choosing general anaesthesia ‘with sedation’ as an anaesthetic option. There were also instances where respondents were able to choose multiple answers when only asked for one. In all above circumstances individual complete responses were analysed and data interpreted in a manner to be consistent with the entire submitted response. One methodological omission was the noticeable absence of cataract surgery as an option for glaucoma surgery, which it may well be in some cases. As a consequence, our survey does not provide an insight into the extent that glaucoma-related cataract surgery was performed or restricted as a result of the pandemic. It is also important to acknowledge other factors influencing surgical decision-making other than COVID-19. Promotion of MIGS devices by their manufacturers and a recognition even before COVID-19 that Paul tubes may offer improved predictability and efficacy when compared with Baerveldt tubes and Ahmed valves, respectively, limit the ability to conclude that such changes in practice were a product of the advent of COVID-19 alone.
留言 (0)