
記住我
In total 42 patients underwent IPAA during the study period, 4 of whom were excluded because of redo IPAA (n = 1), non FA-guided IPAA (n = 2) or another FA imaging platform (n = 1). Thus, 38 patients were included, [55.3% male, median age 45 years (IQR 24–51 years)] (Table 1). The majority of patients (89.5%) underwent IPAA for ulcerative colitis (UC). Other diagnosis included Crohn’s disease (n = 1), familial adenomatous polyposis (n = 1), Lynch syndrome (n = 1), and Lynch syndrome in combination with MUTYH-associated polyposis (n = 1). Comorbidities are shown in Table 1. The majority of patients (89.5%) underwent a modified-2-stage (Table 1). Surgical details are shown in Table 1.
Table 1 Baseline characteristics and operative detailsPrimary outcomeDuring IPAA, vascular ligation was performed in 15 of 38 patients (39.5%). In 3 of these cases, the ileocolic arcade was ligated, in 10 interconnecting branches, and in 2 a combination. FA was performed before and after ileoanal anastomosis in 29 patients (76.3%), in 6 patients (15.8%) only before anastomosis and in 3 patients (7.9%) only after. Time values for the entire cohort and comparison for vascular ligation are shown in Table 2. Time values before anastomosis with ICGi as t = 0 were prolonged, although not significantly, in patients with vascular ligation. No differences were observed for time values once ICG was observed in the pouch (times with inlet or anvil as t = 0). After anastomosis, no time differences were observed, except for a longer (non-significant) time interval between ICG injection and first signal.
Table 2 Time to fluorescent enhancement: time values for patients with or without vascular ligationSecondary outcomesFA findings led to change in management in 7 patients (18.4%) (Table 3), due to absence of ICG fluorescence in parts of the pouch in 6 cases and to delayed ICG fluorescence in one. Absence of ICG fluorescence was noticed in a small area of the pouch (< 1 cm of bowel) in 4 patients. In 2 patients, the non-fluorescent part was at the blind loop after pouch construction and was additionally resected. In the 2 other patients, the non-fluorescent area was in close proximity to the anvil or at the longitudinal stapler line, and was reinforced by sutures. In 2 patients, absence of fluorescence in a segment of terminal ileum (10 cm and 25 cm) led to selection of a more proximal loop for pouch creation. Intact but delayed ICG fluorescence was noticed in 1 patient between anvil and blind loop (33 s) and an ileostomy was created.
Table 3 Change in management due to fluorescence angiography in patients with or without vascular ligationChange in management occurred more often after vascular ligation (6/15 (40.0%) vs 1/23 (4.3%); p = 0.010) (Table 3). In case of ligation of the ileocolic arcade, change in management occurred in one out of three cases in which additional resection of the blind loop was performed. In case of ligation of interconnecting branches, change in management occurred in four out of ten cases and included suture reinforcement (2/4), additional resection of the blind loop (1/4) or ileostomy creation (1/4). When ligation of both ileocolic arcade and interconnecting branches was performed, 1 out of 2 patients required pouch reconstruction using a more proximal loop. In the latter case, a new pouch was reconstructed after absence of fluorescence in the entire pouch subsequently to ligation of the ileocolic arcade. For adequate length of the new pouch, interconnecting branches were additionally ligated. However, in this case, no intact arcade was present and only segmental branches, leading to an additional resection of 25 cm of small bowel. The pouch was created with ICG-perfused small bowel and anastomosed under acceptable tension. No significant differences were found for time values between patients with or without change of management (data not shown).
Median additional operative time owing to FA was 3 min (IQR 2–3 min). Time values were not correlated to haemodynamic parameters (p > 0.05), except for heart rate that was inversely correlated to time value ICGi-inlet (p = 0.024).
Median postoperative hospital stay was 6 days (IQR 6–14 days). Anastomotic leakage was observed in 6 patients (15.8%). All anastomotic defects were located on the circular anastomosis without signs of ischaemia or retraction. In 5 of 6 cases of leakage, reoperation was required to create an ileostomy making it a Grade C leak. For management of anastomotic leakage, 4 patients underwent EVAC and 2 had immediate transanal closure of the anastomotic defect. Of the 5 patients that received a secondary ileostomy, 4 had stoma closure after a median of 177 days (total range 131–323 days) after IPAA, and 1 patient is still undergoing EVAC therapy.
With regard to the long -term results, 83% of patients with an anastomotic leakage (5/6) had a functional anastomosis after a median follow up of 28 months (IQR 24–33 months). The only patient with a stoma still in situ is a patient with UC and dysplasia, who had already undergone neoadjuvant chemoradiation and a low anterior resection complicated by a chronic leak, for which the patient underwent a resection of the leaking anastomosis with IPAA.
There was no mortality in this cohort. Occurrence of anastomotic leakage did not significantly differ between patients with or without vascular ligation (2/15 (13.3%) vs 4/23 (17.4%), respectively; p = 1.000). Two anastomotic leaks in patients with vascular ligation occurred after ligation of interconnecting branches, one of which was combined with ligation of the ileocolic arcade. Anastomotic leakage was observed in 2 of 7 patients with a change in management (28.6%), compared to 4 of 31 (12.9%) when the procedure remained unchanged (p = 0.302).
Comparison of time values in patients with or without anastomotic leakage are shown in Table 4. Time values including transit time through the pouch were non-significantly prolonged in patients with anastomotic leakage (anvil-blind loop, time values to pouch-anal anastomosis). Time from ICGi to pouch-anal anastomosis was predictive for anastomotic leakage (p = 0.135, AUC = 0.734). A cut-off value of 53 s was derived to predict anastomotic leakage (specificity 100%, sensitivity 50%, positive predictive value 100%, and negative predictive value 89%).
Table 4 Time to fluorescent enhancement: times values for patients with or without anastomotic leakageIn 1 case, mucosal ischaemia of the blind loop was observed by endoscopy, after ligation of interconnecting branches without stoma creation (Fig. 3). Time values were 92 s for ICGi-blind loop and 64 s for anvil-blind loop. No anastomotic leakage occurred, the mucosa seemed to re-epithelialize over time and the pouch was preserved. In the case of intact but delayed ICG fluorescence between anvil and blind loop (33 s) after ligation of interconnecting branches leading to primary ileostomy, no anastomotic leakage occurred.
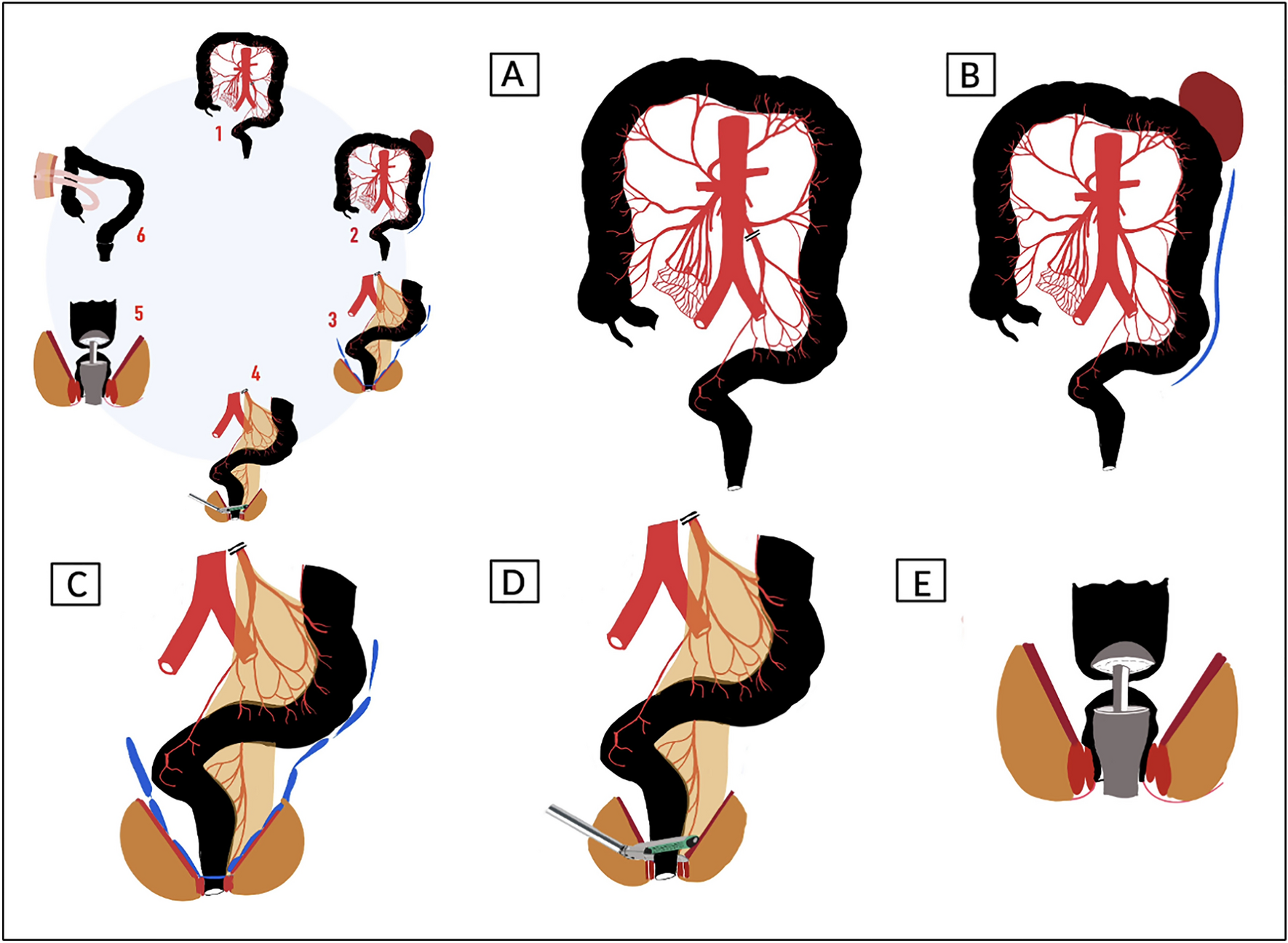
Fig. 3
A case with intact but delayed fluorescence and mucosal ischaemia of the blind loop
留言 (0)