
記住我
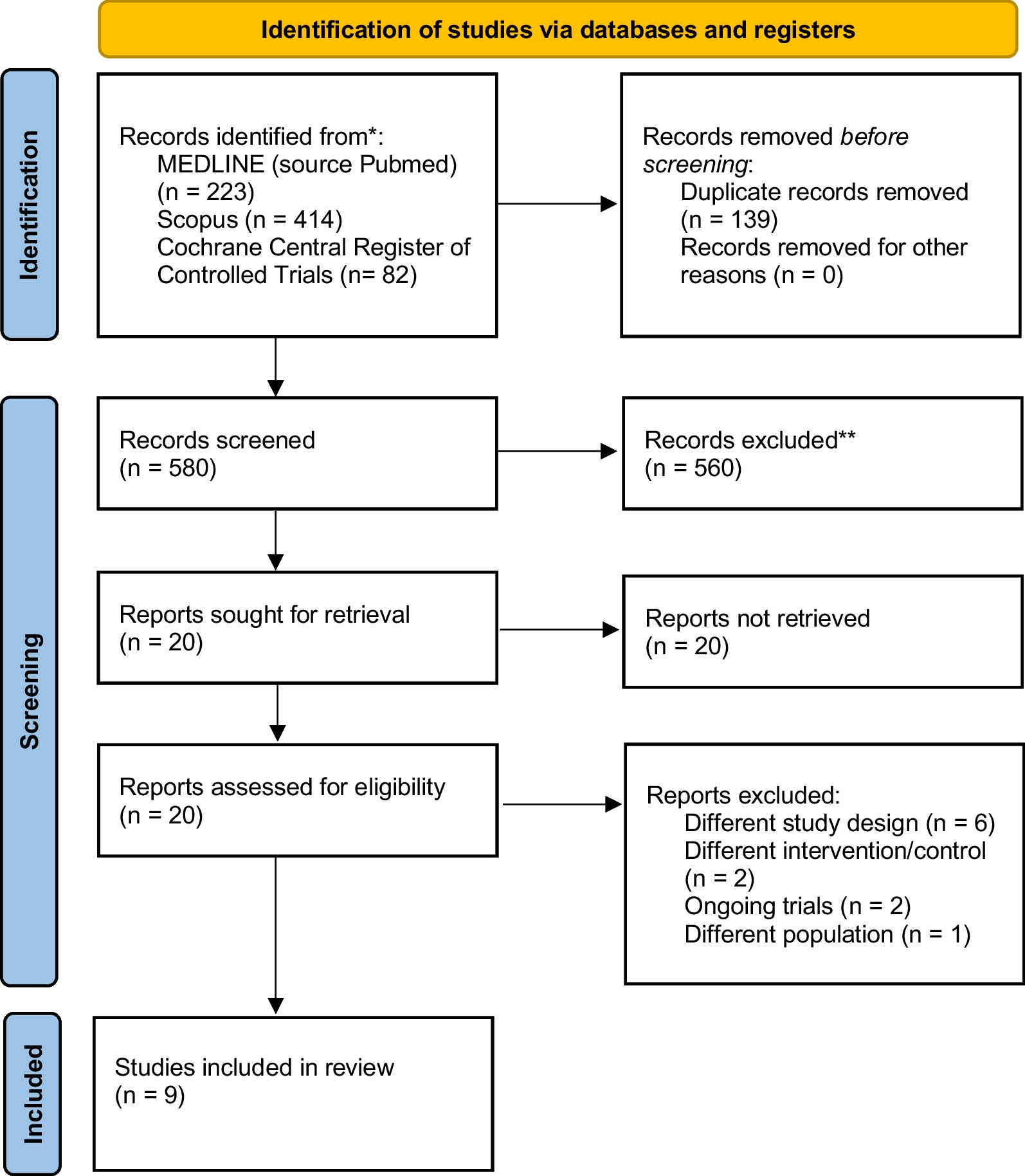


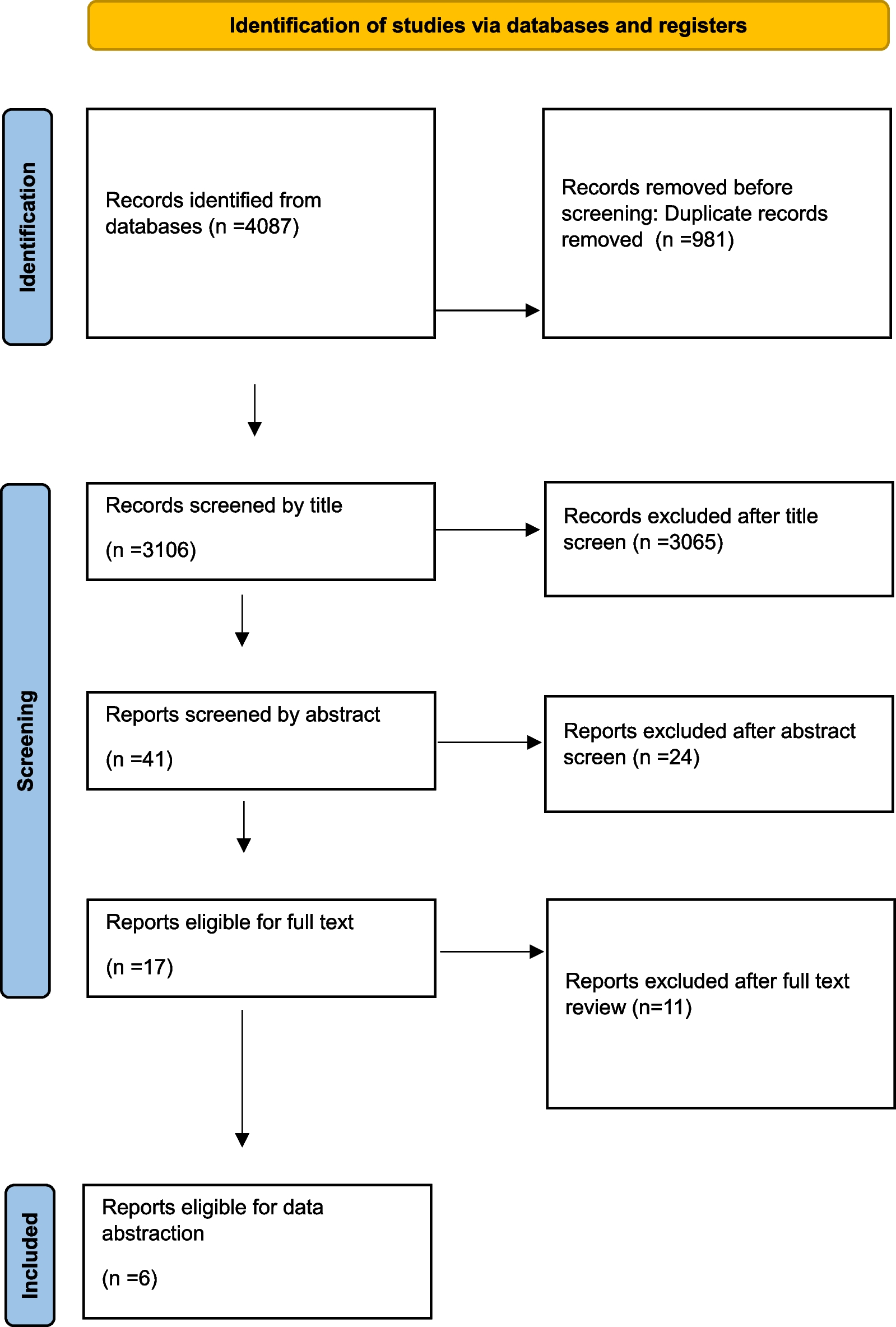
Of the 7743 records screened, ten studies, including two RCTs [28, 29] and eight observational studies [20,21,22,23,24,25,26,27], were included in this systematic review (Fig. 2). Among the eight observational studies, seven were before-after comparisons [20,21,22, 24,25,26,27], and one was a retrospective analysis [23]. The participants in these studies were all civilian trauma patients. One study incorporated ROTEM into DCR to resuscitate combat causalities; however, it was excluded as it did not have a definite transfusion strategy [30]. Of the ten included studies, only one was a multi-center trial [29], and the remaining were single-center studies [20,21,22,23,24,25,26,27,28]. Most of the studies were performed in the USA [22,23,24, 26,27,28], and the others were conducted in Europe [20, 29], Australia [21], and China [25]. One center, Denver Health Medical Center, published two studies: one was a before-after observational study [27], and the other was an RCT [28]. TEG was the most frequently used VHA device in the included studies (eight studies) [20, 22,23,24,25,26,27,28]; ROTEM [21], and TEG or ROTEM [29] were conducted in the other two studies. Regarding the transfusion strategy, two RCTs compared TEG or ROTEM-guided strategy to CCT-guided strategy [28, 29]; eight observational studies compared TEG or ROTEM-guided strategy to non-TEG or non-ROTEM-guided strategy [20,21,22,23,24,25,26,27], two of them were CCT-based [20, 22], one was an MTP protocol [26], and the others did not mention (Table 1). The detailed transfusion strategies and relevant VHA tests are shown in Additional file 1: Table S2 and Additional file 1: Table S3. The risk of bias in RCTs is shown in Additional file 1: Figure S1; one study [28] may had more risk of bias than another [29]. The overall risk of bias assessment of observational studies was moderate or severe (Additional file 1: Table S4), and their NOS scores ranged from 6 to 7 (Additional file 1: Table S5).
Fig. 2
Flow diagram of study selection
Table 1 Characteristics of included studiesEffect of the VHA-guided strategy on blood transfusion in trauma patientsEight studies gave detailed RBCs, plasma, platelet, and cryoprecipitate/fibrinogen amounts for the included patients [20,21,22,23,24,25, 28, 29]. One study grouped the patients according to RBCs transfusion amounts (≥ 6 U or ≥ 10 U) and mechanism of injury (MOI) (blunt or penetrating) and performed a stratified analysis [26]. In the last study, the blood products were illustrated in a figure, and the data could not be extracted; it concluded that there was a trend of fewer products in the post-TEG group but did not reach a significant difference [27] (Table 2).
Table 2 Effect of VHA-guided strategy on blood transfusionIn the included studies, most of them did not find significant differences between the VHA-guided strategy and control strategy on the amount of RBCs transfusion (seven studies) [20, 21, 25,26,27,28,29], plasma transfusion (five studies) [20, 22, 25, 27, 28], platelet transfusion (seven studies) [20,21,22, 25,26,27,28], and cryoprecipitate/fibrinogen transfusion (seven studies) [20, 22,23,24,25, 27, 29].
In addition, three studies supported that the VHA-guided strategy could reduce the use of RBCs in trauma patients [22,23,24]. As for plasma transfusion, four studies indicated that the VHA-guided strategy reduced plasma transfusion amounts [
留言 (0)