
記住我
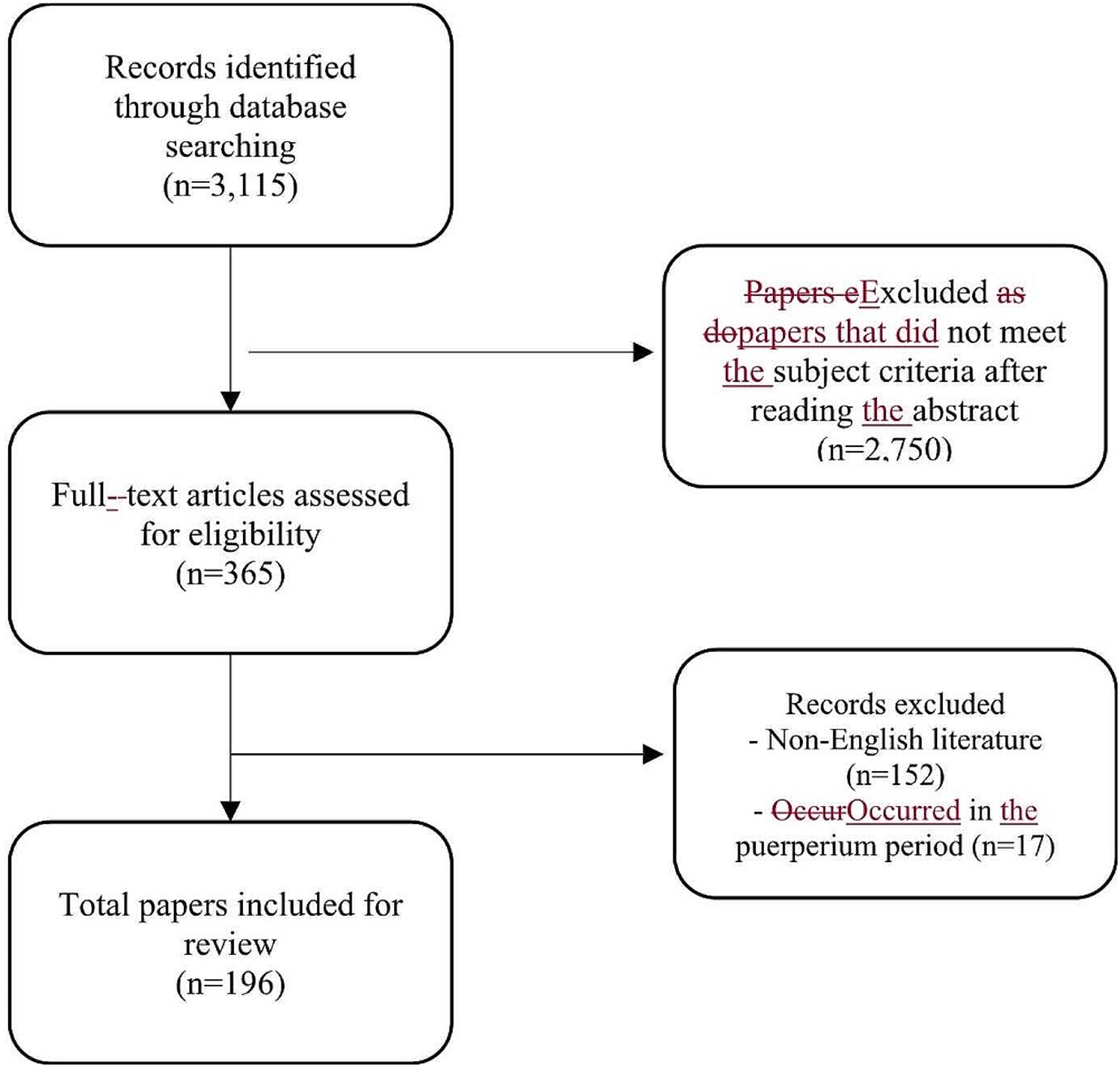


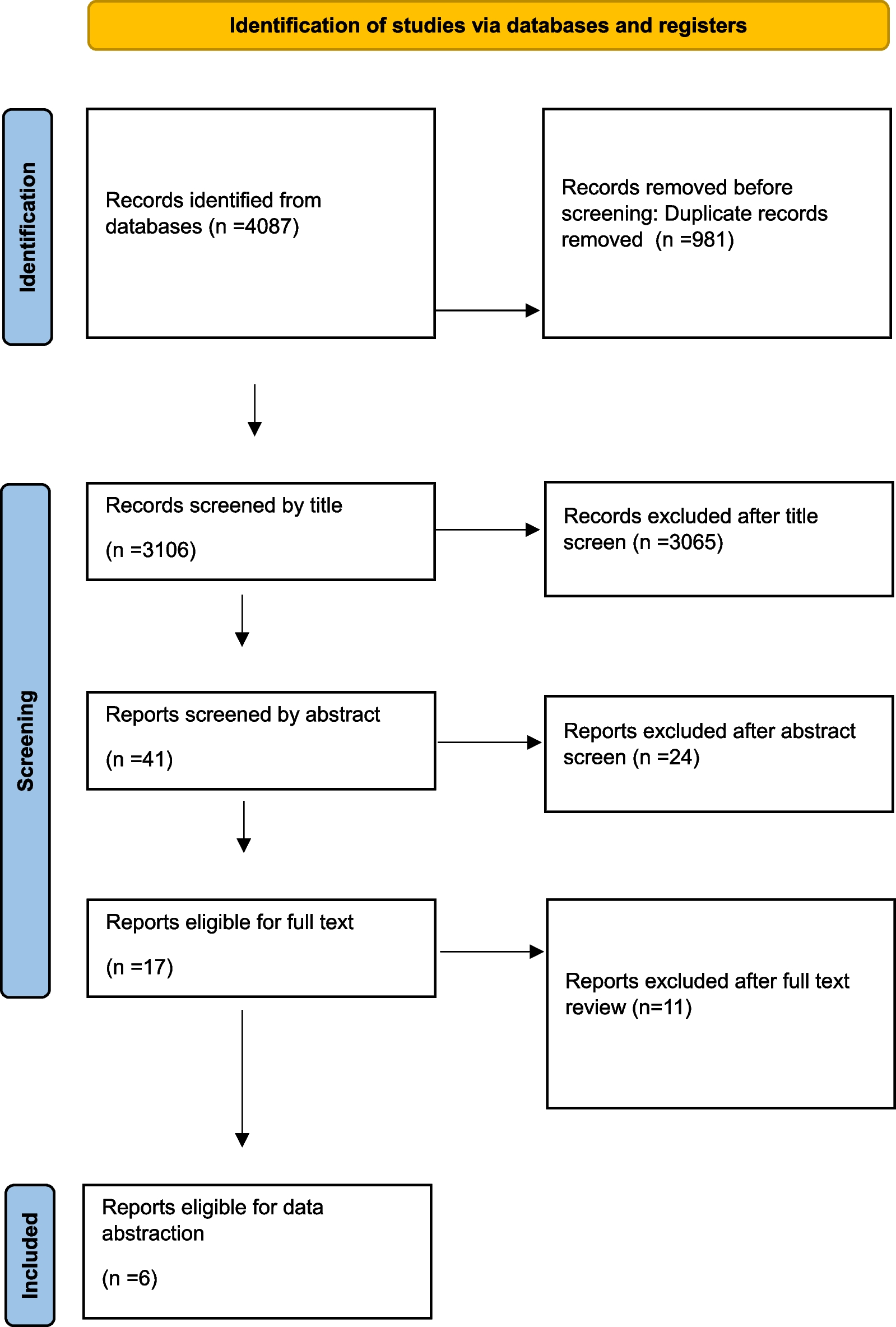
The bibliographer conducted a computerized search in different databases (MEDLINE, PubMed, Scopus, Web of Science, Embase). Citations were included up to June 2021 using the primary search strategy: acute postoperative pain, emergency surgery, pain assessment, acetaminophen, NSAIDs, ketamine, opioids, epidural anesthesia, peripheral nerve blocks, continuous wound infusion, local infiltration combined with AND/OR with synonyms and MeSH terms. We considered acute pain management after major abdominal pathology requiring urgent emergency laparotomy or laparoscopy, including reoperations after elective gastrointestinal surgery and reoperations after previous abdominal surgery. No language restriction was imposed. Duplicates and animal studies were removed. The dates were selected to allow comprehensive published abstracts of clinical trials, consensus conferences, comparative studies, congresses, guidelines, government publication, multicenter studies, systematic reviews, meta-analysis, large case series, original articles, and randomized controlled trials. Narrative review articles were also analyzed to identify other studies. Abstracts were screened, and irrelevant studies were removed; then, a full-text assessment of the articles was performed. Case reports were excluded. In case of disagreement between the two reviewers (FC and FCo), the consensus was reached by discussion. If there was no consensus, another two reviewers were sought (FCa and FFo). PRISMA guidelines flowchart [12] is reported in Fig. 1. Level of evidence (LoE) was graded in high, moderate, low, and very low. The grade of recommendation (GoR) graded as strong, moderate, and weak was calculated, keeping into consideration the GRADE model [13]. An international expert panel discussed the different issues in subsequent rounds. At each round, the manuscript was revised and improved. The final version about which agreement was reached resulted in the present manuscript.
Fig. 1 Notes on the use of the guideline
Notes on the use of the guidelineThese guidelines present evidence-based methods for optimal management of acute postoperative pain management in emergency general surgery patients. The practice indications which were promulgated in this work do not represent a standard of practice. These are suggested plans of care based on the best available evidence and experts’ consensus, but they do not exclude other approaches as being within the standard of practice. For example, they should not be used to compel adherence to a given medical management method, which method should be finally determined by the treating health care provider after considering the conditions at the relevant medical institution (staff levels, experience, equipment, etc.) and the characteristics of the individual patient. However, the treatment results’ responsibility rests with those directly engaged and not with the consensus group.
Pain assessment and managementStatementsPostoperative pain must be recognized and treated as soon as possible and as best as possible in all patients (high recommendation, intermediate quality evidence).
Emergency general surgery may be associated with more severe postoperative pain; specific attention should be given to this patient group (GoR 2, LoE B) (moderate recommendation, intermediate quality evidence).
Postoperative pain assessment, at rest and—if possible—on movement, is strongly recommended, to improve patient management after emergency surgery (moderate recommendation, intermediate quality evidence).
Preemptive analgesia is a viable option in reducing postoperative opioid consumption (GoR 2, LoE B) (moderate recommendation, intermediate quality evidence).
Adequate education for the patient and, if possible, of the family about the surgical and anesthesiologic treatment, options, plan, and aims of pain management should be performed whenever it is possible (GoR 1, LoE B) (high recommendation, intermediate quality evidence).
Perioperative pain management should be implemented considering patient history, comorbidities, ongoing chronic therapy, and potential risk for substance abuse (GoR 1, LoE B) (high recommendation, intermediate quality evidence).
Validated pain scales should be included into treatment planning, ongoing evaluation, and adjusting process (GoR 1, LoE B) (high recommendation, intermediate quality evidence).
Pain management should be adjusted to ensure the greatest effect and the lowest side effects possible (GoR 1, LoE B) (high recommendation, intermediate quality evidence).
Emergency general surgery (EGS) is related to a worse acute postoperative pain compared to elective surgery [14,15,16,17,18]. Patient- and family-centered education is regarded as very important during the preoperative and postoperative periods [14, 15, 17, 19,20,21,22]. Telling patients how a drug is chosen, its properties and effects, understanding its side effects, and shared in the decisions helps reduce APP. A recent study proved that a lower educational level worsens pain [23].
An accurate evaluation including psychiatric comorbidities, namely dementia and delirium, may facilitate APP management since pain assessment techniques in these conditions may be much more time-consuming [19, 21, 24]. Assessment tools that incorporate a behavioral component for pain scoring have demonstrated validity in patients with dementia [25]. Special attention should be paid to the treatment of anxiety [26], evaluation of depression [26], and catastrophizing [15, 17]. Uncontrolled pain syndrome is manifested by tachycardia, arterial hypertension, increased rigidity of the muscles of the anterior abdominal wall and chest muscles, which leads to alteration of the ventilation and hypoxemia, difficulties in coughing and definitively to an increased risk of respiratory infectious complications. Enhanced sympathetic stimulation inhibits peristalsis and at the same time increases the tone of the smooth muscles of the intestine, which is fraught with the development of postoperative paresis. In addition, postoperative pain syndrome prevents early mobilization of patients and also contributes to their emotional and physical suffering, sleep disturbances. A sudden increase in pain, especially associated with the appearance of tachycardia, hypotension, hyperthermia, requires an urgent comprehensive assessment of the patient’s condition, since this may be a harbinger of postoperative complications (bleeding, anastomotic leaks, deep vein thrombosis, etc.).
All these conditions may contribute to worsening APP outcome. Coping strategies could be used specially to contrast catastrophizing thoughts.
The assessment of preoperative chronic pain is necessary because it is demonstrated that previous chronic pain history since may be associated to a worse APP [22]. Moreover, high APP pain level may lead to persistent postoperative pain [16, 17, 19, 20, 22, 27].
Accurate APP’s assessment, which is essential, is usually underestimated, underevaluated, and underperformed [14,15,16, 18, 20, 21, 23, 24, 28,29,30,31,32]. Some tools such as visual analog scale (VAS) score for some aspects seem to be inappropriate in measuring APP since it does not give a multidimensional pain evaluation. Hence, predictor index or questionnaire should be adopted to give the best APP evaluation.
Consideration should be given to APP follow-up evaluation and adequate therapy during the postoperative period. In fact, pain drugs are often administered not at regular intervals [18, 33] nor according to pain scales [15, 18, 33]. Local policy must include standard interval at which a patient is assessed and reassessed for pain. After a pain intervention is completed, reassess patients for both pain control and adverse reactions to the intervention at an appropriate interval based on the anticipated effect. When a significant change in worsening pain level is reported, reevaluate the patient for possible postoperative complications. A combined nurse service with clinician supervision seems to provide better outcomes in APP management [14, 15, 18, 20, 21, 23, 24, 34, 35]. It is proven that 24 h/day monitoring with a regular assessment/documentation guarantees a better pain treatment [14, 20].
In addition to psychiatric comorbidities, chronic pain, and patient dealing with substances of abuse, special attention should be paid to OSAS patients, since a correlation with APP is not fully understood [36, 37]. In this category of patients, antalgic therapy recommendation aims to reduce as much as possible the use of opioids to prevent possible cardiopulmonary complications. Furthermore, literature advises to be aware of age, body mass index (BMI) and gender: Younger age [16, 18, 23] and female gender [16, 18, 33] could be risk factors for APP. Some studies show that low BMI is associated with better pain outcomes [37]. Also knowing about the patient’s smoking habits could improve APP [23].
Preemptive and preventive NSAIDs seem to reduce both pain and morphine use. Clinically significant adverse events from nonsteroidal anti-inflammatory drugs (NSAIDs) administered before surgery are possibly under-reported; for this reason, it is impossible to define with high level of evidence the safety of either preemptive or preventive NSAIDs [38].
Non-opioids drugsStatementsOpiates usage should be reduced as much as possible in postoperative pain management strategies (strong recommendation, intermediate quality evidence).
Multimodal pain management should always be considered to improve analgesia while reducing individual class-related side effects; a pharmacological step-up approach including major opiates when necessary should be adopted (strong recommendation, intermediate quality evidence).
Whenever contraindications are absent, acetaminophen, NSAIDs (strong recommendation, high-quality evidence), and gabapentinoids administration (moderate recommendation, moderate quality evidence) are recommended in multimodal analgesia.
Acetaminophen administered at the beginning of postoperative analgesia may be better and safer than other drugs (strong recommendation, intermediate quality evidence).
Acetaminophen used in multimodal and preemptive therapy is associated with a reduction of opiates side effects and improved postoperative outcomes (strong recommendation, intermediate quality evidence).
Coxib administration may be considered if there are no contraindications (strong recommendation, moderate quality evidence).
Multimodal analgesia involves the use of different classes of analgesic medications (NSAIDs, COX2 inhibitors, gabapentinoids, or acetaminophen in combination with morphine IV-PCA) with different mechanisms of action on the peripheral and/or central nervous system.
The different combinations of these drugs lead to additive or synergistic effects on pain relief and can potentially reduce the side effects of mono-modal interventions. The drugs used for this purpose include:
Acetaminophen (paracetamol): it is effective as an analgesic mainly if used in combination with NSAIDs or morphine. Its use reduces opioids use [39,40,41]
NSAIDs: are indicated for the treatment of moderate pain when used alone. Their use in multimodal analgesia reduces morphine consumption and related side effects [40]
Opiates: are the first-line therapy to treat pain in these patients. They also reduce anxiety and dyspnea [42, 43]. PCA is recommended when iv route is needed in patients with adequate cognitive functions, starting with bolus injection in opioid naïve patients [7].
Gabapentinoids such as gabapentin and pregabalin can be considered as a component in multimodal analgesia. They act by decreasing the release of neurotransmitters in the synapse, thus providing a nociceptive blocking activity.
Alpha-2-agonists: in addition to their anti-hypertensive effect, they have been shown to have a sympatholytic effect by inhibiting norepinephrine release, thus reducing the opiates requirements.
Acetaminophen in a multimodal regimen is a valid and effective option. A study conducted in nearly 800,000 patients undergoing common major surgical elective and emergency procedures showed that this drug in a multimodal therapy regimen provides a cost-effective strategy to improve outcomes and patient satisfaction with a side-effect profile that is superior to opioids alone in moderate–severe APP [44]. The use of acetaminophen is associated with shorter length of stay, decrease in opioid-related complication rates, and lower costs in a heterogeneous population of patient who underwent to elective and emergency cardiovascular, colorectal, general, obstetrics and gynecology, orthopedics, or spine surgery [45]. A case–control cohort study of 1231 patients undergoing gynecologic and abdominal surgery showed that ibuprofen and acetaminophen (600 mg every 6 h and 500 mg every 6 h) could offer an adequate postoperative pain control with a supply of opioids (hydrocodone or oxycodone) if needed [46]. A single study suggests the use of IV acetaminophen in the beginning of postoperative analgesia since its antalgic properties are better and safer than IV tramadol in patients undergoing laparoscopic cholecystectomy [47].
Different efficacy can be assessed according to the timing in the administration of acetaminophen, in the context of multimodal analgesia, as a preemptive analgesia. Acetaminophen used in multimodal and preemptive therapy (1 g before laparotomy with naproxen 250 mg and pregabalin 150 mg) was associated with a reduction of opiate side effects as well as a fewer length of stay, lower opioid-related complication rates, and lower costs compared to patients who had not received this treatment [48].
Intravenous acetaminophen (i.v. acetaminophen every 6 h from 6 h after surgery up to 72 h) can be associated with thoracic epidural anesthesia (TEA); a study has been shown to provide a superior postoperative pain management compared to TEA alone in a randomized controlled trial with 120 patients who underwent distal gastrectomy [49].
Caution is needed in the frail patient, especially in the context of coexisting liver disease. For an amount of acetaminophen infusion sufficient to ensure a significant reduction in postoperative pain compared with groups without treatment (P = 0.008), an increase in alanine aminotransferase has been observed (P = 0.043) [50].
Perioperative NSAIDs utilization results regarding the reduction of hospital stay and lowering morbidity have been demonstrated in elective surgery [51]. The literature suggests a potential correlation with dehiscence, technical failures, and wound healing inhibition in emergency general surgery patients with colon or rectal anastomoses [52]. There is not enough evidence to establish the effectiveness of NSAIDs beyond their safety profile.
In terms of efficacy for the individual NSAID drugs, no direct comparisons trial is available. Effectiveness analysis was conducted on the single NSAID once at a time. In the case of abdominal emergency surgery, it was found that perioperative administration of Ibuprofen IV 800 mg every 6 h decreased morphine requirements and pain score and it has been found safe and well tolerated [53]. The literature might suggest also considering the use of HPβCD-diclofenac in a multimodal approach to analgesia. HPβCD-diclofenac in postoperative setting reduces postoperative opioid requirements during the whole postoperative course (all P < 0.005 vs placebo) [54]. The combination of NSAIDs with acetaminophen improves the quality of pain relief compared to the appointment of each of the drugs separately [55]..
The use of coxib is effectiveness in a major surgery context [56, 57] since it provides analgesia and opioid-sparing effects in the 2–3 days immediately following major gastrointestinal surgeries employing laparotomy and reduces the VAS scores both at rest and with movement, reducing also opioids adverse effects in patients following liver resection. A word of caution must be spent regarding the associated use of coxib and NSAIDs as their combination seems to increase the incidence of myocardial infarction and to affect kidney function [58, 59].
Results about the use of gabapentinoids in postoperative management in EGS are heterogeneous and conflicting [60].
Preemptive anesthesia with other medications such as gabapentinoids to treat postoperative pain could lower opioid consumption and pain scores.
Due to the paucity of the literature, it is not possible to provide specific indications for the use of ketamine in emergency abdominal surgery. According to the literature, a single dose or infusion of ketamine appears to reduce pain score, and opioid consumption in the 48 h following surgery, especially in patients who have undergone major chest, abdominal, and orthopedic surgery [61,
留言 (0)