
記住我










COVID-19 often causes hypoxemic respiratory failure and ARDS.1 As severe respiratory failure subsequently causes physical impairment, including ICU-acquired weakness,2 early mobility therapy is believed to improve clinical outcomes.3 On the other hand, severe hypoxemia and respiratory distress, which are hallmarks of the acute phase of COVID-19,4 may cause difficulties and barriers to implementing early rehabilitation. However, despite several recommendations for early mobility therapy management and strategy procedures for COVID-19-related acute respiratory failure,5,6 studies on the effectiveness and safety of early mobility therapy in ICUs are rare in these patients. In this report, we aimed to evaluate the incidence of adverse events during early mobility therapy in the ICU as well as the correlation of early mobility therapy with the prognosis of patients with COVID-19-related acute respiratory failure.
MethodsThis single-center prospective study enrolled consecutive patients who were admitted in the ICU of Kitasato University Hospital for COVID-19-related acute respiratory failure treatment from October 1, 2020–September 30, 2021. Subject characteristics, including biomarkers and severity scores, were collected on admission, whereas information regarding respiratory therapy and rehabilitation sessions was obtained during intensive care and clinical course. This study was performed in accordance with the Declaration of Helsinki and was approved by the ethics committee of Kitasato University (KMEO B20-360). Since all outcome measures are collected as a part of routine care, we obtained verbal informed consent from all participants or their surrogates and made the information on the research public by opt-out.7
Subjects were assessed by an ICU team consisting of physicians, nurses, and physiotherapists within 24 h of being admitted to the ICU to determine whether rehabilitation could be initiated. Early mobility therapy, particularly out-of-bed mobilization, was carried out based on specific medical recommendations.5,6 Early mobility therapy protocol consisted of monitoring of clinical conditions, evaluation of muscle strength by the Medical Research Council (MRC) scale, and prevention of disability by active limb exercises and out-of-bed exercise.6 The level of out-of-bed exercise was assessed with the ICU mobility scale and determined based on the subjects’ MRC scale.8 Each early mobility therapy session was implemented by ICU nurses and one of 4 physiotherapists with specialized knowledge about intensive care. During all early mobility therapy sessions, the following adverse events stated in the global consensus were recorded: worsening dyspnea, breathing frequency > 30 breaths/min, percutaneous oxygen saturation SpO2 < 93% on oxygen therapy, requirement of an FIO2 > 0.50 or PEEP > 10 cm H2O, respiratory distress, arterial hypertension or hypotension, bradycardia or tachycardia, intercurrent arrhythmia, or shock.6
The end points of the study were the 7-category ordinal scale one month after the ICU admission and the in-hospital all-cause death. The 7-category ordinal scale consisted of the following categories: (1) not hospitalized and with resumption of normal activities; (2) not hospitalized but was unable to resume normal activities; (3) hospitalized but did not require supplemental oxygen; (4) hospitalized and required supplemental oxygen; (5) hospitalized and required nasal high-flow oxygen therapy, noninvasive ventilation, or both; (6) hospitalized and required extracorporeal membrane oxygenation, invasive mechanical ventilation, or both; and (7) death.9 The time period for in-hospital death was calculated as the number of days from the ICU admission to the date of death.
Statistical AnalysisThe clinical characteristics of subjects who had adverse events during early mobility therapy, subjects without adverse events, and subjects who did not receive early mobility therapy were compared using Mann-Whitney U test for continuous variables and chi-square or Fisher exact test for categorical variables as appropriate. The correlation of early mobility therapy implementation and adverse events with the end points was also assessed using Jonckheere-Terpstra test and multiple regression analysis for the 7-category ordinal scale and Kaplan-Meier survival curve with log-rank test and multivariate Cox proportional hazard model for in-hospital death. Based on the sample size of end points in the analyses, age, sex, body mass index (BMI), history of diabetes, episode of sepsis, use of mechanical ventilation in the ICU, C-reactive protein, lactate dehydrogenase, ferritin, and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were used as covariates for multiple regression analysis, whereas APACHE II score was used as a covariate for the Cox hazard model.
ResultsAmong 782 hospitalized patients with COVID-19, 105 subjects with COVID-19-related acute respiratory failure were admitted to the ICU. Rehabilitation was initiated for all subjects in the ICU, and 90 subjects (85.7%) underwent early mobility therapy.
In a total of 315 early mobility therapy sessions, adverse events during mobilization were documented in 142 sessions (451 times/1,000 sessions) of 67 subjects (74.4%). The following events were more frequently noted: 98 sessions with SpO2 < 93%, 73 with worsening dyspnea, 56 with breathing frequency > 30 breaths/min, and 25 with hypotension, whereas no serious events were documented. Two or more types of adverse events simultaneously occurred in 86 early mobility therapy sessions. No significant differences in clinical features were observed between with or without adverse events during early mobility therapy (Table 1). Conversely, subjects without early mobility therapy were significantly older and had lower BMI, higher prevalence of sepsis in the ICU, higher use of noradrenaline agent and mechanical ventilation, and higher APACHE II and Sequential Organ Failure Assessment scores as compared to subjects who underwent early mobility therapy with adverse events during mobilization (Table 1). Based on the mobility levels of 90 subjects with early mobility therapy upon discharge from the ICU, 24 subjects could sit on chairs, 30 could stand or march in place, and 36 could walk, without statistical differences in the ICU mobility scale between those with or without adverse events (P = .83).
Table 1.Characteristics of Subjects Who Underwent Early Mobility Therapy With and Without Adverse Events and No Early Mobility Therapy Subjects
The presence of adverse events during mobilization was not associated with poor clinical outcomes in the 7-category ordinal scale, whereas subjects who could not perform early mobility therapy had poor outcomes (Fig. 1). The adjusted coefficients for the 7-category ordinal scale against early mobility therapy with adverse events were −0.29 (95% CI3,6 −1.10 to 0.52, P = .48) for early mobility therapy without adverse events and 1.32 (95% CI 0.25–2.37, P = .02) for non–early mobility therapy. During the median follow-up period of 18 d, 19 in-hospital deaths (18.3%) occurred. Figure 1 shows the association between early mobility therapy implementation with or without adverse events and in-hospital mortality. No association between adverse events during mobilization and in-hospital death was consistently observed (log-rank: P = .24); however, non–early mobility therapy was associated with lower survival rates as compared with early mobility therapy with adverse events (log-rank: P < .001). Based on the presence of adverse events during early mobility therapy, the adjusted hazard ratios were 0.30 (95% CI 0.04–2.41, P = .26) for early mobility therapy without adverse events and 5.34 (95% CI 2.08–13.66, P < .001) for non–early mobility therapy.
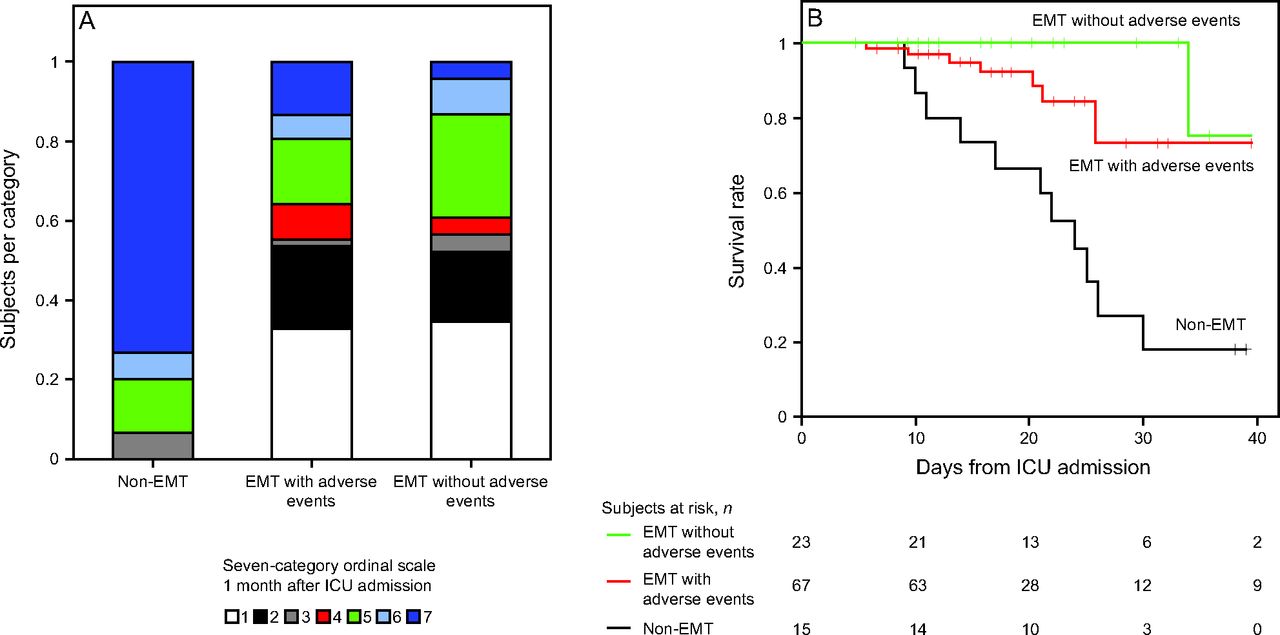 Fig. 1.
Fig. 1. Correlations between the implementation of early mobility therapy with or without adverse events and the clinical outcomes. A: Seven-category ordinal scale one month after ICU admission. : (1) not hospitalized and with resumption of normal activities; (2) not hospitalized but was unable to resume normal activities; (3) hospitalized but did not require supplemental oxygen; (4) hospitalized and required supplemental oxygen; (5) hospitalized and required nasal high-flow oxygen therapy, noninvasive ventilation, or both; (6) hospitalized and required extracorporeal membrane oxygenation, invasive ventilation, or both; and (7) death. B: Kaplan-Meier survival curves of the 3 groups based on the implementation of early mobility therapy with or without adverse events for in-hospital mortality. Early mobility therapy with adverse events (green line) was not associated with higher in-hospital mortality compared to early mobility therapy without adverse events (red line).
DiscussionTo our knowledge, this study is the first to reveal that subjects with COVID-19-related acute respiratory failure during early mobility therapy in an ICU present a relatively high rate of non–serious adverse events despite the delayed initiation of mobilization in accordance with a recent study.10 Nevertheless, in these subjects, adverse events during early mobility therapy were not associated with poor clinical outcomes and higher in-hospital deaths. Therefore, the implementation of early mobility therapy may be a beneficial treatment for patients with COVID-19-related acute respiratory failure considering the potential risk of adverse events during mobilization.
The rate of adverse events during early mobility therapy in an ICU was reported to be < 10% in critically ill subjects with acute respiratory failure.11 The results confirmed that patients with COVID-19-related acute respiratory failure would likely develop oxygen desaturation and tachypnea during early mobility therapy, although exercise-induced oxygen desaturation has been documented in survivors of COVID-19 after recovery from pneumonia.12 A recent study, implementing a similar early mobility therapy procedure to our study, reported that deterioration during mobility therapy was associated with an increased hospital length of stay in subjects with community-acquired pneumonia.13 However, this association was not observed in our results with subjects with COVID-19. The delayed initiation of early mobility therapy due to subject instability with or without adverse events may be a cause of the differences in findings between the studies.
Several statements support the effectiveness of early mobility therapy for patients with COVID-19 to prevent physical dysfunction.3,6 On the other hand, since the general conditions are unstable due to severe oxygenation disorders and inflammatory storm in the acute phase of COVID-19-related acute respiratory failure, a review mentions the doubts about the suitability of early mobility therapy.14 In this study, we confirmed that although minor events during early mobility therapy were observed in high rates of participants there were no serious complications. However, the subjects who were not able to engage early mobility therapy had a higher illness acuity. A recent study reported the safety and usefulness of neuromuscular electrical stimulation in subjects with severe COVID-19 who had difficulty with early mobility therapy due to unstable clinical conditions and ICU-acquired weakness.15 Thus, it is considered to need the trial on optimal rehabilitation intervention for the patients with severe acute chronic respiratory failure who have unstable breathing during early mobility therapy.
As this was an observational study, it is unclear whether early mobility therapy itself improved patient outcomes. The worse clinical condition of subjects with non–early mobility therapy should also be considered in the interpretation of the results. The small sample size of the included subjects should also be acknowledged as a limitation. Therefore, further interventional evaluation using additional samples to assess the effects of early mobility therapy on the clinical outcomes of patients with COVID-19-related acute respiratory failure is required.
Adverse events during the early mobility therapy are frequently observed without serious events in patients with COVID-19-related acute respiratory failure. We found that the adverse events during early mobility therapy implementation were not associated with poor outcomes in subjects with COVID-19-related acute respiratory failure. These findings may be valuable in understanding and validating the early mobility therapy for patients with COVID-19-related acute respiratory failure to increase its risk management level and effectiveness.
AcknowledgmentsThe authors would like to thank the medical and nursing staff of the ICU in Kitasato University Hospital for their valuable contribution to clinical practice.
Copyright © 2022 by Daedalus Enterprises
留言 (0)