
記住我
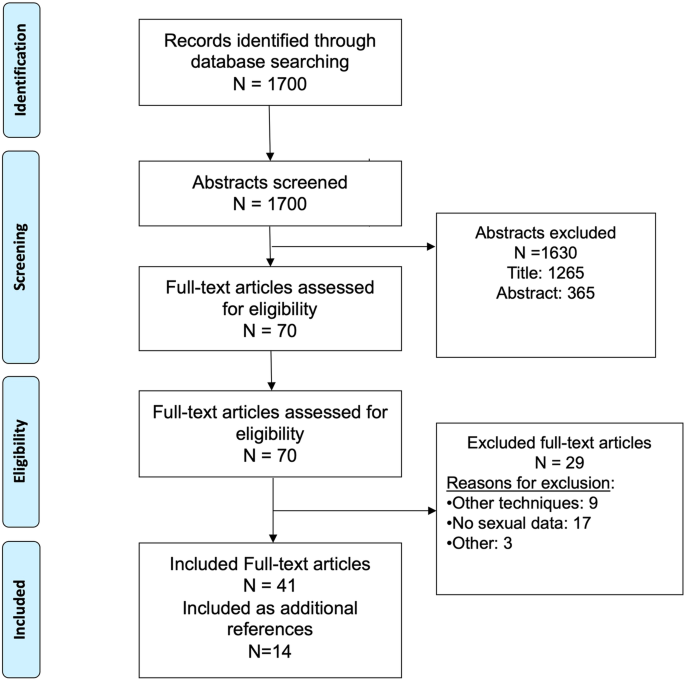
The source population for our study cohort consists of 80,458 men, originally enrolled in the Finnish Randomized Study of Screening for Prostate Cancer (FinRSPC) in 1996–1999 [22]. Age at baseline was 55–67 years, and the population of Finland in this age group is predominantly White European. In Finland, two drugs were in clinical use for hyperuricemia management during the study period: allopurinol (931 users in our cohort) and probenecid (9 in our cohort). There were too few probenecid users to allow statistical analysis, thus they were excluded. After linkage to Finnish national registries, men who were diagnosed with PCa before baseline, had used probenecid, or had deficient medication purchase information were excluded. The study cohort consists of 9252 men with prostate cancer (Fig. 1).
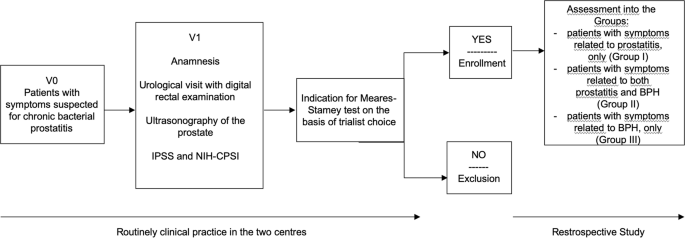
Fig. 1
A CONSORT-style flow chart of study cohort formation.
Prostate cancer clinical characteristicsPCa cases diagnosed during the follow-up were identified through the Finnish Cancer Registry, the national registry that comprehensively registers cancers diagnosed in Finland [23]. Latest PSA measurements before PCa diagnoses were obtained from Fimlab and Huslab laboratory databases. Fimlab and Huslab are the leading providers of diagnostic laboratory services in the Helsinki and Pirkanmaa areas. We obtained Gleason -scores in prostate biopsy from patient records. The cases were grouped into three PCa risk categories according to the EAU (European Association of Urology) prostate cancer guidelines: low-risk = Gleason 6, cT1/2a or PSA < 10; intermediate-risk = Gleason 7, cT2b or PSA 10–20; high-risk = Gleason 8–10, cT3–T4, metastatic or PSA > 20 [24]. Information on primary PCa treatment (surgery, radiation therapy, ADT, active surveillance/watchful waiting, others) was available from patient records.
Information on use of allopurinol and other medicationsAs a part of the tax-funded national health insurance organized by the Social Insurance Institution of Finland (SII), all Finnish citizens are entitled to reimbursement of the price of physician-prescribed drug purchases. Compensation ranges 40–100% (with €4.5 co-payment) depending on medical indication of drug use. When allopurinol is used for gout, reimbursement is 65% of the price [25]. It is typically received as price compensation at the time of purchase. SII records all reimbursed drug purchases. In Finland, allopurinol is reimbursed and available only through a physician’s prescription and thus systematically recorded by the SII. Nevertheless, SII does not record drug use during hospital inpatient periods or over-the-counter medication purchases. Additionally, we obtained information on purchases of antihypertensive drugs, antidiabetic drugs, statins and aspirin use from SII.
Information in the SII prescription registry includes each purchase (date, dose, package size and number of packages). The Anatomical Therapeutic Chemical (ATC) codes were used for drug identification (M04AA51 and M04AA01 for allopurinol). We linked medication data to the study cohort by using personal identification numbers, issued to all Finnish residents at birth or immigration.
Information on comorbiditiesWe collected information on BMI from a survey sent along with invitations to the third FinRSPC screening round [26]. We had BMI information for 985 men out of 9252 men (11%).
Information on the Charlson comorbidity index was calculated based on diagnoses registered by the national hospital discharge registry (HILMO) during 1996–2000 [27]. HILMO is a nationwide healthcare registry, maintained by the government of Finland. It records all diagnoses and procedures during in- and outpatient hospital visits to health care units. Primary health care diagnoses are not included in this registry.
Information on deathsWe received information on dates and causes of deaths from the death certificate registry of Statistics Finland. The registry records primary, immediate, and contributory causes of death using ICD-10 coding. Deaths with ICD-10 codes 61 (PCa) registered as the primary cause of death were PCa-specific deaths.
MethodsStatistical analysesExtended Cox regression was used to estimate hazard ratios (HRs) and 95% confidence intervals (95% CI). Follow-up started at PCa diagnosis and continued until death, the end of 2015, or emigration (analyses on risk of death). The time metric was years and months as a decimal of years since PCa diagnosis. Analysis was performed separately for two endpoints: PCa death and overall death. The proportional hazard assumption was not evaluated, as the exposure of interest was time-dependent and allowed to change during the follow-up.
Allopurinol use after PCa diagnosis was analysed as a time-dependent variable, i.e., user status was updated for each follow-up year based on medication purchases. For eliminating effect of bias caused by selective discontinuation of drugs in patients with terminal phase cancer, we kept the subjects as users after the first purchase [28]. For example, a man who purchased allopurinol every second year was categorized as an allopurinol user at every follow-up year following his first purchase. Cumulative years of use and average intensity of use were updated for each follow-up year.
Allopurinol use before PCa diagnosis was analysed as a time-fixed variable including all usage that occurred between 1995 and the year of diagnosis.
Our hypothesis is that the potential effect of allopurinol on CSS would require long-term, rather than acute, use. A total amount of allopurinol (g) purchases was calculated for each calendar year. Yearly allopurinol amount (g) was divided by the dose corresponding to the drug-specific defined daily dose (DDD). The WHO-recommended DDD for allopurinol is 0.4 g [29]. Cumulative DDDs (total amount of drug used), duration (number of years with any allopurinol purchases), and intensity (DDD/years of use) were calculated for allopurinol use.
We used two different extended Cox regression model adjustments to estimate risk of PCa death by allopurinol use: an age-adjusted (age at diagnosis) and multivariable-adjusted model with further adjustment for FinRSPC screening arm, use of antihypertensive drugs, antidiabetic drugs, statins, aspirin, EAU PCa risk group and Charlson comorbidity index. Age is connected to lower CSS and OS. FinRSPC screening might have effect for CSS and OS due to more frequent physician visits. Antihypertensive drugs are associated with slightly higher PCa-specific mortality in our study cohort [30]. Statins are associated with lower PCa-specific mortality [31]. Charlson comorbidity index is a potential confounding factor because it predicts risk of death and presumably associates with allopurinol use. In Finland, physician-prescribed aspirin (ASA) is used mostly for preventing cardiovascular events, while NSAIDs are used for analgesia. ASA use was associated with modest reduction in PCa-specific mortality in meta-analysis, therefore ASA was included in the model adjustments [32]. We did not adjust the model with NSAID use, because NSAIDs are commonly used analgesics in acute gout.
Kaplan-Meier curves were used to illustrate CSS and OS by prediagnostic allopurinol use.
Subgroup analysisPossible effect modification by selected background variables was estimated in stratified subgroup analyses. Effect modification was evaluated by statistical significance of the interaction terms by the stratified variable and allopurinol use in an extended Cox regression model with PCa death as the endpoint. Effect modification was tested for statin and diabetes medication use, FinRSPC trial arm and sociodemographic group (marital status, pensioner vs non-retired). FinRSPC screening arm is an interesting factor for subgroup analysis, as chronic inflammation affects PSA and with this analysis, we could evaluate how systematic PSA testing may modify allopurinol association with CSS. Sociodemographic group is an interesting subgroup analysis, as lifestyle factors and health care use likely differ by sociodemographic group. If we think that allopurinol could have some biological effect on CSS, it must be the same in all sociodemographic groups. We also did stratification by statin use because we have shown before that statin use after PCa diagnosis may delay prostate cancer progression [33].
Lag time analysisTo minimize and evaluate protopathic bias, we performed lag-time analyses to estimate association between allopurinol use and each of our end points allowing one- to three-year latency.
Supplementary analysesFor a supplementary analysis, we excluded all allopurinol non-users. Then we divided our study population to three groups with similar sizes by cumulative duration and intensity of allopurinol use. The lowest tertile was used as the reference group, to assess whether CSS or OS is associated with longer duration or higher intensity of use (after adjustment for age or age and other prognostic factors).
We used IBM SPSS statistics software version 27 for all data analyses.
留言 (0)