
記住我
In this study on extended electrocardiographic monitoring in PPCM, we showed a high prevalence of arrhythmic events. In this regard, ILR in addition to 24 h-Holter monitoring had a significantly higher arrhythmic yield than 24 h-Holter monitoring alone. All major brady- and tachyarrhythmias occurred in the early phase of the disease (i.e., within the first 4 months after diagnosis). Neither 24 h-Holter or ILR monitoring detected any episodes of AF.
The most commonly detected VA in this cohort was NSVT, which occurred in four patients (16%), all of which had a severely impaired LVEF. Our reported prevalence of VAs is comparable to studies on the use of the WCD in patients with newly diagnosed PPCM, which also showed a high burden of VAs (12%) [9]. Previous studies have shown that a prolonged corrected QT (QTc) interval by Bazett’s formula (QTcB) is associated with adverse outcome in PPCM [6]. Indeed, it is well established that a prolonged QTc predisposes to VAs and is associated with SCD [10]. Three out of four patients with NSVT had a prolonged QTcB at presentation. However, our study was underpowered to show a conclusive relationship between QT prolongation and occurrence of VAs.
In a recent systematic review and meta-analysis, Sammani et al. [11] evaluated the burden of VAs in patients with non-ischaemic DCM. They reported an annual event rate of 4.5% for sustained VAs in DCM. In their study, younger age, hypertension, prior (non-)sustained VA, decreased LVEF, LV dilatation, late gadolinium enhancement (LGE) and genetic mutations (Phospholamban (PLN), Lamin A/C (LMNA), and Filamin-C (FLNC)) were significant predictors of arrhythmic events. [11]
One patient with severe heart failure developed third degree AV block 1 week after PPCM diagnosis. The ventricular escape rhythm eventually failed, and the patient demised from asystole before she could reach the hospital. Complete heart block (CHB) at the time of PPCM diagnosis has previously only been described in case reports [12, 13]. In both case reports, an underlying myocarditis with focal inflammation was suggested as a possible mechanism of the CHB. However, this was not confirmed by cardiac magnetic resonance (CMR) in either of the cases [12, 13]. In a cohort of patients with advanced heart failure, severe bradycardia or electromechanical dissociation (EMD) was described as the rhythm at the time of arrest in 62% of patients [14]. Severe bradyarrhythmia or EMD, in particular, precedes cardiac arrest in patients with idiopathic DCM, and is believed to account for about one-third SCD in these patients. [15, 16]
24 h-Holter ECG monitoring is an inexpensive and non-invasive diagnostic modality, but is confined to monitoring during the usual 24–48 h weartime [17]. However, newer devices (i.e., adhesive patches attached to a small device recorder) allow for continuous rhythm monitoring over several days [18]. The benefit of ILRs is that they allow for much longer periods of rhythm monitoring (i.e., up to 3 years). The device records patient- or event-activated (auto-triggered) ECG tracings. ILRs are usually indicated, if the suspected arrhythmia occurs infrequently. Disadvantages are the invasive insertion with the risk of postoperative wound infection, and higher costs compared to Holter ECG monitoring or patches [19]. Furthermore, ILRs do not typically record short runs of NSVT. The REVEAL XT© device that we used in this study, only detected NSVT when more than 16 consecutive beats of NSVT was detected by the device. The prevalence of NSVT might, therefore, be higher than what we report.
In this study, we could show that ILR in addition to Holter monitoring had a higher yield of arrhythmic events than 24 h-Holter monitoring alone. We also found that patients with severely impaired LV systolic function were at highest risk of arrhythmias, particularly shortly after index diagnosis. We, therefore, recommend that ILR should be considered in the early post-partum period in patients with severe heart failure and/or severe LV dysfunction, especially in patients with symptoms suggestive of an arrhythmia, and particularly when the 24 h-Holter did not detect any arrhythmia. However, larger prospective studies are required to support our recommendations.
Our study also highlights the importance of event adjudication of the REVEAL XT© device. In our study, the minority of detected arrhythmias were true arrhythmic events. As our study population consisted of pregnant and postpartum women, some false events may be related to enlarged breasts leading to artefacts. However, regular device interrogations and expert adjudications of all stored events are crucial to detect arrhythmic events. Newer generation ILR devices can be connected telemonitoring platforms and allow for a more timely response to a serious arrhythmic event and give the opportunity for pre-emptive interventions [19].
Previous prospective studies on the prevalence of major arrhythmic events in PPCM investigated the use of a WCD [8, 9]. Similar to our study, Duncker et al. demonstrated that arrhythmic events occurred in the early phase after PPCM diagnosis (40–165 days). In their study, the WCD detected VAs in 12% of patients and all episodes of VF could be successfully terminated by a device shock [9]. These data highlight that WCD has important therapeutic benefit in terminating ventricular tachyarrhythmias in patients with severely reduced LVEF. Indeed, WCD can, therefore, be used as “bridging” therapy, allowing for medical therapy to be initiated and protecting against SCD from VAs. This strategy would prevent unnecessary implantation of ICDs in young women with a disease with potential for LV recovery [20]. However, due to the high cost of the device, patient selection and risk stratification is of great importance [21].
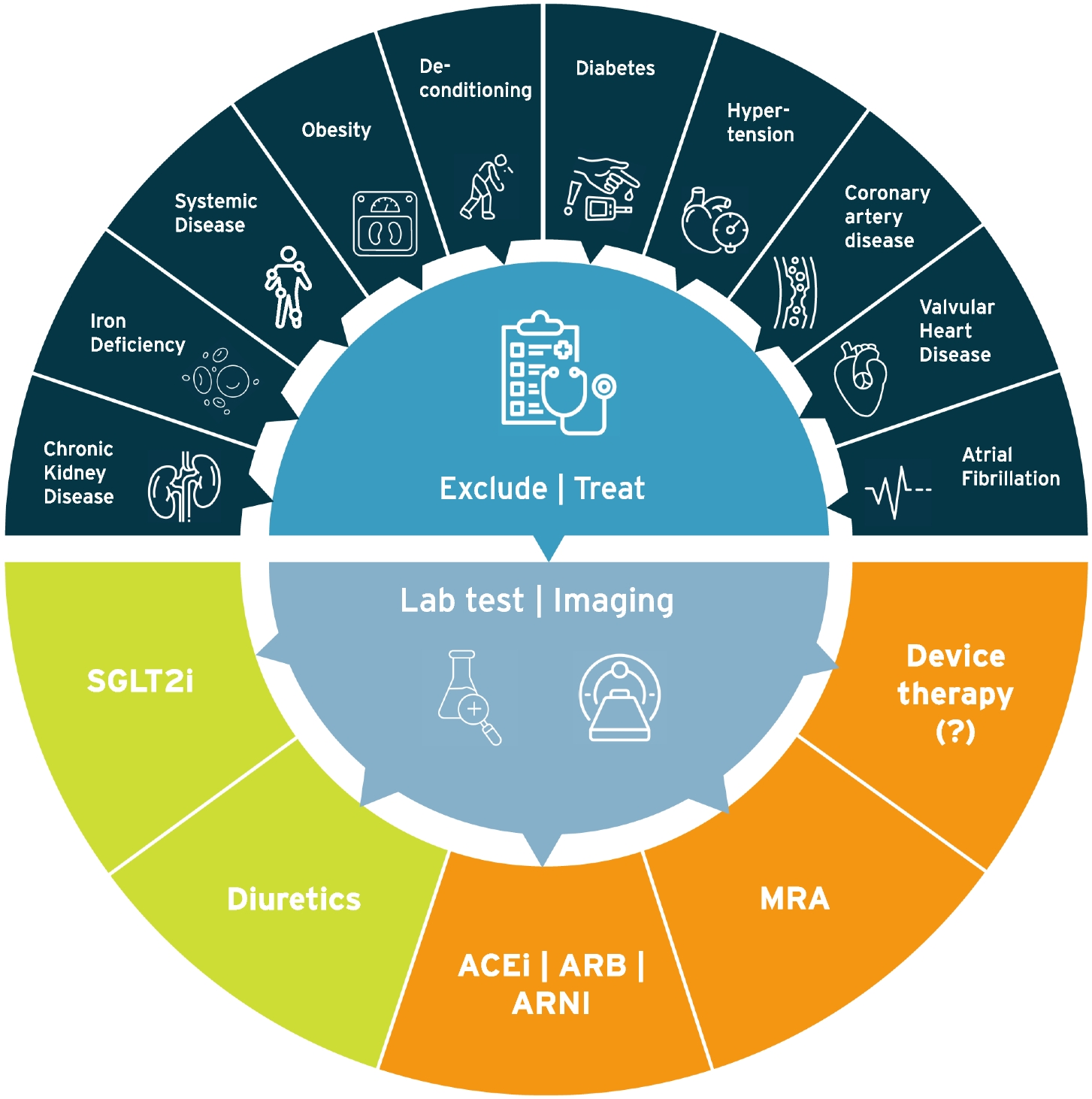
It should be highlighted that WCDs are not available in large parts of the world. As illustrated in the proposed algorithm for the detection and management of arrhythmias (Fig. 4), we recommend extended electrocardiographic monitoring in PPCM if WCDs are not available. This would include Holter monitoring on all patients with severely impaired LV systolic function in the acute phase of the disease, and ILRs when 24 h-Holter monitoring was inconclusive, or if symptoms suggestive of arrhythmias occur infrequently.
Fig. 4
Proposed algorithm for the diagnosis and management of arrhythmias in PPCM. ECG electrocardiogram, HF heart failure, ICD implantable cardioverter defibrillator, ILR implantable loop recorder, LVEF left ventricular ejection fraction, WCD wearable cardioverter defibrillator
LimitationsWe acknowledge that the patient cohort included in this study is small, and do not allow for definitive recommendations. However, PPCM is a relatively rare disease. The sample size might have affected the estimate of the true prevalence of arrhythmias in patients with newly diagnosed PPCM. As only ten patients received an ILR (which allows for continuous rhythm monitoring), we cannot comment on subsequent arrhythmias in patients who only received 24 h-Holter ECG monitoring.
Our study is also not adequately powered to answer the question about which patients are most likely to benefit from ILR, but patients with severely reduced LV function or severe symptoms of heart failure appeared to be at higher risk for ventricular arrhythmias. Therefore, as recommended by the latest ESC position statement on PPCM [2], WCDs should be considered for patients with a LVEF ≤ 35% in the early stage of disease, i.e., when arrhythmias are more prevalent. However, these devices are not readily available in large parts of the world. In settings where WCDs are unavailable for patients with a LVEF ≤ 35%, extended monitoring with an ILR may, therefore, be useful for the detection of atrial and ventricular arrhythmias. If ventricular arrhythmias are detected, an ICD should be considered for secondary prevention.
Our sample size is also too small to answer the question whether patients with short runs of NSVT have a higher risk of SCD. However, it may be a surrogate marker of a more severely diseased ventricle. The detection of NSVT is important, because it has previously been reported to be a marker of increased risk of SCD in patients with non-ischaemic cardiomyopathy [22]. Late gadolinium enhancement (LGE) on cardiovascular magnetic resonance (CMR) has been established as a strong predictor of VAs and SCD in a wide spectrum of non-ischaemic cardiomyopathies [23]. We acknowledge the lack of CMR scans in this cohort, which could have been important to answer the question if PPCM patients with arrhythmic events show signs of structural abnormalities such as LGE on CMR.
In this study, we used the out of the box settings for the detection of VAs by ILR, as most physicians would do in clinical practice. It is possible this underestimated the frequency of shorter NSVT episodes. However, considering only NSVT of more than 16 consecutive beats on Holter, would have decreased the detection rate by Holter monitoring.
A further limitation to this study is that Holter monitoring was only performed at the time of index diagnosis, and not at follow-up. This might have underestimated the true prevalence of arrhythmias in this cohort.
We encourage validation of our findings in a larger, multi-centred cohort. However, to the best of our knowledge, this is the largest prospective study on extended electrocardiographic monitoring on consecutive women with PPCM regardless of their initial LVEF.
留言 (0)