
記住我
Previous studies elucidated the physiological functions of isthmin-1 (Ism-1) on glucose and lipid metabolism.
Adipokines were closely correlated with albuminuria in patients with diabetes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYHigh serum Ism-1 might be involved in the presentation of albuminuria.
The association between Ism-1 and albuminuria needs to be further investigated in prospective studies to find out, whether Ism-1 is a risk marker of diabetic kidney disease.
IntroductionType 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by hyperglycemia.1 Long-term hyperglycemia can lead to the development of microvascular complications, including diabetic nephropathy (DN), diabetic retinopathy, and peripheral sensory and autonomic neuropathy.2
DN is the most common cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD) in China and worldwide.3 4 DN generally begins with microalbuminuria, followed by macroalbuminuria, along with a progressive decrease in glomerular filtration rate.5 The most recognizable outcome of DN is ESRD, which requests renal replacement therapy in the form of dialysis or transplantation. This undoubtedly poses a substantial social and economic burden. Microalbuminuria is an indicator of early renal injury in patients with diabetes and associated with the risk of cardiovascular disease and CKD progression.6 Therefore, early detection is essential in preventing the development of DN.
Diabetes is a chronic disease characterized by insulin resistance and pancreatic islet failure. Growing evidence has proved that adipokines play important roles in the pathogenesis of diabetes and its complications, including DN. For instance, serum neuregulin-4 levels were positively related to fasting glucose and microvascular complications,7 8 and serum omentin levels were negatively associated with insulin resistance.9 Urinary kidney injury molecule-1 (uKIM-1) levels were significantly higher in patients with albuminuria or declined estimated glomerular filtration rate (eGFR) compared with patients with diabets with no evidence of DN.10 uKIM-1 reached its highest level in CKD stage 2 and showed a gradual decrease in patients with CKD stages 3 and 4.10 On the one hand, adipokines can keep glucose homeostasis through regulating glucose uptake and glucose production; on the other hand, adipokines play an important role in the prevalence and development of diabetes complications through inducing or inhibiting inflammation, oxidative stress, apoptosis and other mechanisms. For example, adiponectin, as the most abundant adipokine, extenuates insulin resistance and inflammation in diabetes. In patients with DN, elevated serum adiponectin concentration was observed.11 Moreover, in cultured podocytes, adiponectin reduced podocyte permeability to albumin, likely acting through the AMPK (AMP-activated protein kinase) pathway.12
Isthmin-1 (Ism-1) is a novel identified adipokine which exists in brain, lung, immune cells, and adipocytes of adult mice.13 14 Previous studies backed up its critical role in embryo development, organ morphogenesis, angiogenesis, and aging process.15–18 Recent studies indicated that Ism-1 had manifold beneficial metabolic effects, including promoting glucose uptake, improving insulin resistance, and inhibiting hepatic steatosis.14 Overexpression of Ism-1 by transducing viral vectors in diet-induced obese (DIO) mice could increase insulin sensitivity, inhibit endogenous hepatic glucose production, and reduce liver fat. In addition, injection with recombinant Ism-1 (5 mg/kg for 21 days) showed a significant lower fasting blood glucose (FBG) and improved glucose tolerance in this study. However, the relationships between Ism-1 with DN and insulin resistance were still unclear in patients with T2DM. Therefore, the present study aimed to investigate the association of serum Ism-1 levels with insulin resistance and early stage of DN (defined by the presence of albuminuria with preserved renal function) in patients with T2DM.
MethodsSubjectsA total of 150 patients with T2DM were recruited from Qilu Hospital of Shandong University from October 2020 to December 2021. Diabetes was diagnosed based on the 2006 WHO criteria.19 To explore the association of Ism-1 with albuminuria and avoid the effect of decreased renal function, we excluded patients with an eGFR of <60 mL/min/1.73 m2. Besides, as we did not measure islet autoantibodies, to ensure the diagnosis of T2DM, we excluded patients with age less than 40 years and fasting C-peptide of <0.3 ng/mL. We also excluded patients with FBG of ≥8.0 mmol/L to ensure the accuracy of insulin resistance measures in the 75 g oral glucose tolerance test (OGTT). Other exclusion criteria and research flowchart are shown in online supplemental file 1.
Clinical data collectionDemographics, clinical parameters, and medical history were collected through the electronic medical record of Qilu Hospital, including age, gender, diabetes duration, weight, height, waist circumference, blood pressure (BP), hypertension, history of smoking, history of alcohol consumption, hemoglobin A1c (HbA1c), serum albumin, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), triglyceride (TG), creatinine, and urinary albumin:creatinine ratio (UACR). UACR were tested by first morning urine sample. The amount of alcoholic beverage consumed was converted to the average grams of ethanol intake per day. History of alcohol consumption was defined as having drunk more than 28.0 g/day ethanol for men (14.0 g/day for women) at least 1 year, current or former.20 History of smoking was defined as having smoked more than one cigarette every day for a year, current or former. Hypertension refers to present hypertension with or without medical treatment before enrollment. Body mass index (BMI) (kg/m2) was calculated as weight (kg) divided by height squared (m2). eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation.21 All patients underwent 75 g OGTT. After at least a 10-hour fast, serum glucose and C-peptide concentrations were obtained at 0, 60,120, and 180 min during OGTT. At the start of OGTT, fasting blood sera were collected in duplicate. One aliquot was stored frozen at −80°C until analysis of Ism-1. Another aliquot was used for the test of glucose and C-peptide. To exclude the confusion of exogenous of insulin, insulin resistance (HOMA2-IR, the update Homeostasis Model Assessment of insulin resistance), and insulin sensitive (HOMA2-%S, homeostasis Model Assessment insulin sensitivity) were estimated by the computerized homeostasis model assessment of C-peptide downloaded online (https://www.dtu.ox.ac.uk/homacalculator/download.php) to objectively reflect insulin resistance and insulin sensitivity.22 23 Serum Ism-1 levels were quantified using ELISA kits (MBS2707255; MyBiosource, Southern California, San Diego, USA).
Definition and groupingAlbuminuria was defined as UACR of ≥30 mg/g in the present study. Microalbuminuria was defined as UACR ranging from 30 mg/g to 300 mg/g, and macroalbuminuria was defined as UACR of ≥300 mg/g. All participants were stratified into the normal-albuminuria group, the microalbuminuria group and the macroalbuminuria group.
Statistical analysisAll analyses were performed with SPSS V.25.0 software. The data were graphed using GraphPad Prism V.8.3. Kolmogorov-Smirnow test was used for normality analysis. Homogeneity of variance was estimated with the F test. Continuous variables are expressed as mean±SD or median (IQR). The categorical variables are presented as percentages. The statistical significance of differences between groups was evaluated by one-way analysis of variance and LSD (least significant difference) post hoc test for continuous variables with normal distribution, Kruskal-Wallis Test for continuous data with skewed distribution and Pearson χ2 test for categorical variables. Binary logistic regression and multivariable linear regression analyses were used to assess the association of serum Ism-1 levels with UACR in different models. In the multivariable linear regression analyses, UACRs were transformed to log10 expression data for reducing skewness. Multivariable linear regression analyses were performed to explore the correlation of serum Ism-1 levels with IR. Only p<0.05 were considered as significant.
ResultsSerum Ism-1 levels were different in patients with or without macroalbuminuriaBased on UACR, all participants were divided into the normal-albuminuria group (n=90), the microalbuminuria group (n=42), and the macroalbuminuria group (n=18, table 1). Compared with the normal-albuminuria group, the microalbuminuria and macroalbuminuria groups had a greater incidence of hypertension and higher usage of ACE inhibitor (ACEI) or angiotensin II antagonist (ARB) treatment. In addition, the macroalbuminuria group had a lower eGFR and serum albumin than the normal albuminuria or the microalbuminuria group. HbA1c is higher in the microalbuminuria group compared with the normal albuminuria group but not significantly different in the macroalbuminuria group. The macroalbuminuria group had the highest serum Ism-1 levels (figure 1), but no difference was observed between the normal-albuminuria group and the microalbuminuria group (p>0.05).
Table 1Demographic and biochemical parameters of the study population in different albuminuria groups
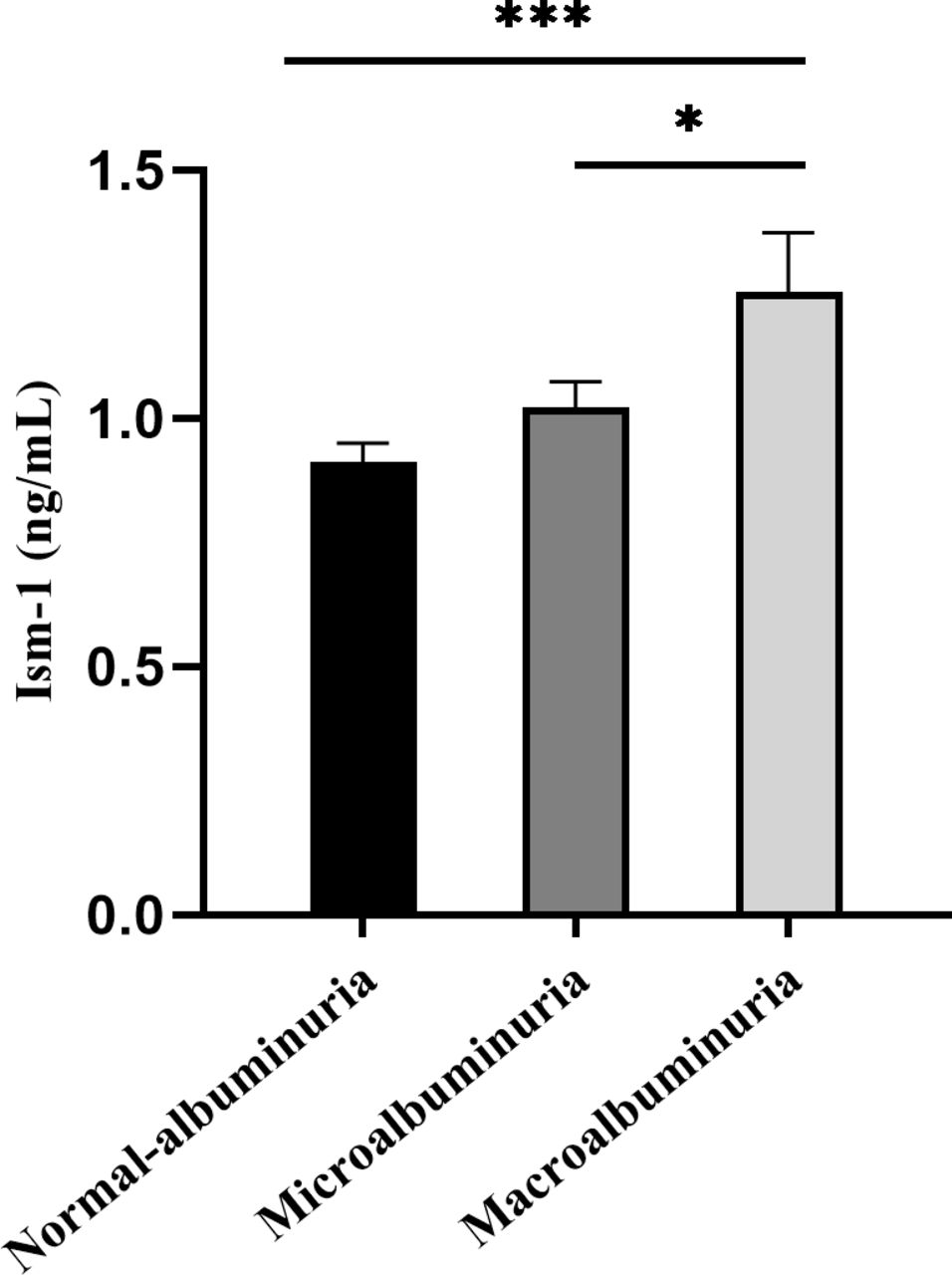 Figure 1
Figure 1 Comparison of the levels of serum Ism-1 in different albuminuria groups. Data are represented as mean±SEM. *P<0.05, **P<0.01, ***P<0.001. Ism-1, isthmin-1.
Association of serum Ism-1 levels with albuminuria in patients with T2DMTo investigate whether serum Ism-1 levels were independently associated with the prevalence of albuminuria, we performed a series of binary logistic regression analyses (table 2) and multivariable linear regression analyses (table 3 and figure 2). BMI, LDL-C, TG, and serum albumin were included into the models because Ism-1 has been proved to suppress lipogenesis and increase protein synthesis and was positively related to BMI.14 Considering hypertension is a known risk factor of albuminuria,24 25 SBP was included in model 3. To minimize the influence of eGFR on the elimination of Ism-1, we excluded patients with eGFR less than 60 mL/min/1.73 m2 and included eGFR in models. The results of binary logistic regression analyses and multivariable linear regression analyses showed that serum Ism-1 levels were positively associated with the severity of albuminuria in patients with T2DM. After adjusting for age, gender, BMI, duration of T2DM, HbA1c, fasting C-peptide, hypertension, LDL-C, TG, albumin, eGFR, and ACEI or ARB treatment, increased serum Ism-1 levels were still significantly associated with the severity of albuminuria.
Table 2Binary logistic regression analyses of the relationship between Ism-1 and albuminuria
Table 3Multivariable linear regression analyses of the relationship between isthmin-1 and log10-transformed urinary albumin:creatinine ratio
 Figure 2
Figure 2 Simple linear regression of serum Ism-1 levels and log10-transformed UACR. Ism-1, isthmin-1; UACR, urinary albumin:creatinine ratio.
Association of serum Ism-1 levels with insulin resistance in patients with T2DMRecent research indicated that Ism-1 might promote glucose uptake and improve insulin resistance in vitro.14 However, the relationships of Ism-1 with insulin resistance in patients with T2DM were still unclear. We conducted a series of multivariable linear analyses to explore the relationship between Ism-1 and insulin resistance. The analysis was adjusted for several covariates, including age, gender, diabetes duration, BMI, hypertension, LDL-C, TG, serum albumin, eGFR, and ACEI or ARB treatment. Results were presented in online supplemental file 2. Unfortunately, no correlations were observed between serum Ism-1 levels and insulin resistance, including fasting C-peptide (p=0.841), HOMA2-IR (p=0.663), and HOMA2-%S (p=0.481).
DiscussionThe results of the current study showed that serum Ism-1 levels were correlated with albuminuria in patients with T2DM, even after adjusting for various risk factors. However, no relationships were observed between serum Ism-1 levels and insulin resistance, which were assessed by 75 g OGTT.
T2DM is a multisystem disease that has reached epidemic proportions, and chronic hyperglycemia eventually leads to the occurrence and progression of DN. There is strong evidence to suggest that adipokines are involved in the onset and development of DN. Adiponectin and leptin are two of the most abundant adipokines. In recent years, many studies highlight the effect of adiponectin on diabetic kidney injury. Serum adiponectin concentrations had a significant positive correlation with UACR.26 Saraheimo et al have identified that serum adiponectin levels, as a risk factor, were associated with progression from macroalbuminuria to ESRD by Cox regression analysis.27 In animal experiments, increased albuminuria was observed in adiponectin–knockout miceHowever, after treatment with adiponectin, normalization of albuminuria was observed.28 Later studies proved that adiponectin receptor agonists could reduce lipotoxicity and oxidative stress through AMPK/PPARa pathway in human glomerular endothelial cells and murine podocytes.12 29 Both low and high serum leptin levels were risk factors for kidney function decline. Meanwhile, lower serum leptin levels were associated with progression of albuminuria in patients with T2DM.30 In summary, previous studies indicate that adipokines are involved in the development of DN and could be a means of therapeutic intervention.
Ism-1 is a 60 kDa secreted adipokine, characterized by a ‘thrombospondin type 1 repeat’ domain and an ‘adhesion-associated domain in MUC4 and other proteins’ domain. The relationship between Ism-1 and albuminuria in patients with T2DM has not been reported. In the present study, all participants were defined by evidence of albuminuria with eGFR of ≥60 mL/min/1.73 m2 (CKD stages 1 and 2). Therefore, we focused on the changes of serum Ism-1 levels in patients with albuminuria and refrained the effect of decreased renal excretion on the levels of circulating Ism-1. Our findings showed that Ism-1 was positively associated with the severity of albuminuria, even after adjusting several risk factors. Patients with higher serum Ism-1 levels were prone to have more severe albuminuria. More in-depth studies are urgently needed to validate the role of Ism-1 on the pathogenesis of albuminuria.
Ism-1, as an angiogenesis inhibitor, induced vascular permeability through the low- affinity receptor avβ5 integrin and high-affinity glucose-regulated protein 78 kDa (GRP78).31 32 To note, Venugopal et al found that mice under different dose injections of Ism-1 showed significantly increased lung vascular permeability in a dose-dependent manner, while no significance increase was observed in the kidney.33 Therefore, we can only assume that Ism-1 has a negative or compensatory role in the progression of albuminuria through a currently unknown mechanism rather than increasing vascular permeability in kidney. Inflammatory burden has been recognized as the main player in the prevalence and progression of DN, which is activated by the metabolic, biochemical, and hemodynamic disorders existing in diabetes.34 Many serum inflammatory markers are elevated in patients with DN, such as C reactive protein:serum albumin ratio,35 mean platelet volume:lymphocyte ratio,36 and monocyte:lymphocyte ratio37 in hemogram. Adipose tissue and adipokines were no longer considered to only devote to energy storage but a regulator of immunity, inflammation, glucose homeostasis, and lipid metabolism.38 We can only propose a hypothesis that Ism-1 may be involved in the progression of albuminuria through inflammation, apoptosis, or lipotoxicity.
Recent research demonstrated that Ism-1 could increase glucose uptake by inducing GLUT4 translocation to the plasma membrane in human and mouse adipocytes. Ism1-KO mice presented impaired glucose uptake and impaired insulin sensitivity, especially in brown adipose tissue and skeletal muscle. Moreover, recombinant Ism-1 has a preventive and therapeutic effect on improving insulin resistance and hepatic steatosis in DIO mice.14 In summary, previous studies suggested that Ism-1 was correlated with insulin resistance.
In the present study, all subjects underwent 75 g OGTT. To avoid the basal high-glucose interfering with the β-cell response, patients with FBG of ≥8.0 mmol/L were excluded. To avoid the disturbance of insulin medication, insulin resistance was estimated by the computerized homeostasis model depending on C-peptide kinetics. Nevertheless, our study showed that no relationship was observed between Ism-1 and insulin resistance in patients with T2DM. Large-sample studies need to further verify our findings.
Strengths of our study are the fact that we identified that serum Ism-1 levels were positively associated with the severity of albuminuria in patients with T2DM for the first time. However, there were several limitations of our study: first, as a cross-sectional study without follow-up, whether serum Ism-1 level changes as the aggravation of DN remains unclear. Second, the relationship of Ism-1 with DN in patients with T2DM needs further study, including patients with impaired renal function. Third, we only tested fasting serum Ism-1 levels rather than repeated simultaneous Ism-1 during OGTT. The conclusion that Ism-1 has no relation with insulin resistance needs more validation.
In conclusion, the results of our study showed that serum Ism-1 levels were significantly higher in patients with T2DM with albuminuria and associated with the value of UACR in patients with T2DM and preserved renal function. However, whether and how Ism-1 participates in the pathogenesis of albuminuria needs more in-depth studies.
Data availability statementData are available upon reasonable request. All free text entered below will be published.
Ethics statementsPatient consent for publicationEthics approvalThis study involves human participants and was approved by the ethics committee of Qilu Hospital of Shandong University (ethics name ID 2021-289). The participants gave informed consent to participate in the study before taking part.
AcknowledgmentsWe thank all participants in this study.
留言 (0)