
記住我
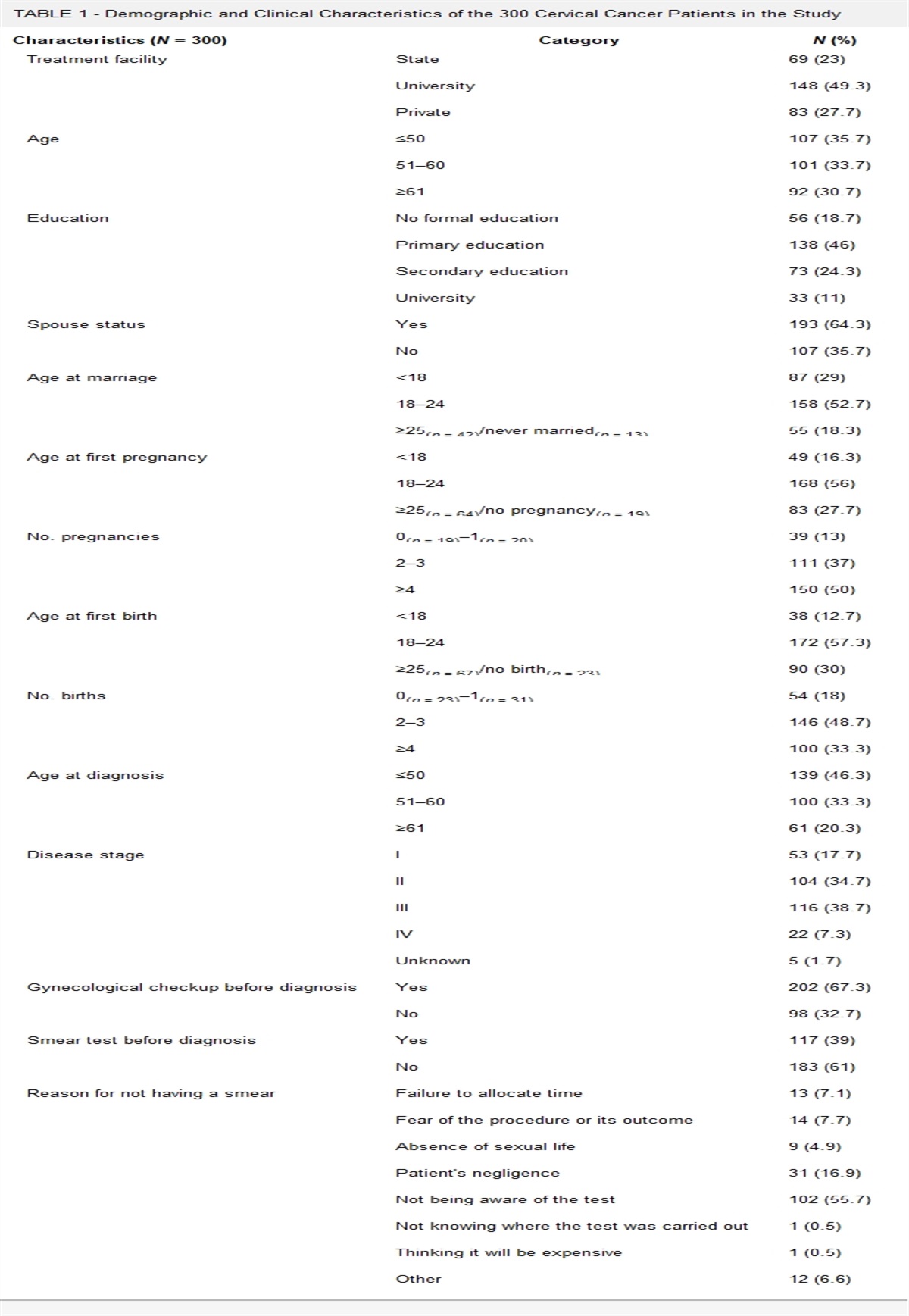
Women living with HIV (WLWH) have an increased risk of infection with the human papilloma virus (HPV).1 Furthermore, their immunocompromised state increases the risk of HPV persistence and progression to cervical intraepithelial neoplasia II-III (CIN II-III) and cancer.2 Combination antiretroviral therapy (cART) has decreased the incidence of opportunistic infections among WLWH;3 however, it has not been shown to reduce the rate of HPV infections among this population.4 Guidelines for management of women with cervical cytological abnormalities were first introduced in 2001 by the American Society for Colposcopy and Cervical Pathology (ASCCP). The 2001 Bethesda System for cytological classification introduced the terms LGSIL and HGSIL to refer to low-grade and high-grade cervical cancer precursors, respectively.5 The latest guidelines for cervical cancer screening for WLWH stratify screening based on age: in WLWH younger than 30 years, screening is done annually and deferred for 3 years after 3 consecutive negative results. For WLWH 30 years and older, HPV testing is recommended, and a colposcopy is indicated if there are 2 repeated results of atypical cells of undetermined significance (ASCUS). An initial ASCUS result alone can be followed up either with a colposcopy or with a 6-month repeat cytology.6,7
The evolution of current guidelines has shown that screening in WLWH has become similar to screening in HIV-negative women8,9 (Table 1). Although cART has improved outcomes for WLWH, the increased likelihood of progression of cervical dysplasia and decreased ability to clear HPV remains.10–12 Despite this faster progression, there is still no consensus as to how frequently WLWH should be screened for cervical cancer. Limited access to health care and cultural barriers have been reported as factors contributing to poor control of the disease in WLWH.13–15
TABLE 1 - Guidelines for Management of Women With Cervical Cytological Abnormalities for Women With HIV: Comparison of 2001 With 2016 (CDC & ASCCP) 2001 guidelines (8) 2016 guidelines (6) Frequency of screening • Screening should be obtained twice during the first year after diagnosis of HIV infection and, if the results are normal, annually thereafter, but no later than 21 y. • Screening should be done at least once per yearASC-H indicates atypical squamous cells, cannot exclude a high-grade lesion.
Among this cohort of minority WLWH who presented with negative baseline cytology, our primary objective was to determine the proportion of women who progress to LGSIL/HGSIL across 5 years, and our secondary objective was to identify associated factors of cytologic progression in this same 5-year period.
MATERIAL AND METHODS Protection of Human SubjectsThe institutional review board approved this study for human subjects' research, and the requirement for written informed consent was waived. After data were extracted from the clinic database and the medical records, they were deidentified before analyses.
Data CollectionWe identified eligible patients using the Gynecologic HIV clinic database in a tertiary care center in Miami, serving a large minority population. We extracted information for each clinic visit for a period of 5 years after the date the patient was eligible. Subsequently, we conducted a retrospective chart review to complement extracted information. Women with a previous diagnosis of HIV, a negative baseline cytology screening between 2009 and 2012, and at least 2 visits within a year period were considered eligible. Visits took place at the Gynecologic HIV Clinic between 2010 and 2013 (n = 162). This clinic serves a large minority population in South Florida including African Americans, Caribbean immigrants, and Latina women. It provides gynecologic and primary care via free or subsidized HIV medical care and social support services. A subanalysis included women with a baseline of 2 consecutive annual cytology screenings who were selected to be reviewed for follow-up cytology screening at 3 years (5 years after baseline). Cervical cytological findings were interpreted using the 1991 Bethesda System criteria.5 Before 2016, the HIV clinic screened WLWH with cytology and colposcopy with cervical biopsy every 6 months until a negative cytologic and colposcopic examination was obtained for at least 1 year. This routine was also continued until surgical treatment for high-grade lesions was performed. In 2016, current guidelines were incorporated in all clinics, and women were screened once per year until 3 serial negative samples were found. In women with negative cytology, follow-up was scheduled at 3-year intervals. If there was more than 1 cytology per calendar year, only the first one was included in the study. All women with abnormal cytological findings underwent control cytology, colposcopy, biopsy, and treatment according to the current guidelines at the time of diagnosis.8,9,16
The following information was collected from the patient's electronic medical record: age at baseline cytology, race/ethnicity, CD4 count, HIV viral load (VL) at baseline, route of HIV transmission, Centers for Disease Control and Prevention (CDC) HIV-defined AIDs, history of sexual transmitted infections (STI), social history, history of smoking cigarettes, cytology results, and HPV test results. Race/ethnicity was collected based on self-identified race, ethnicity, and place of birth. We classified race/ethnicity in the cohort as African Americans (AA) if born in the United States and self-identified Black non-Hispanic, Afro-Caribbean (AC) if born in any country of the Caribbean and self-identified Black non-Hispanic, and Hispanic if self-identified as Hispanic, regardless of country of birth. A detectable VL was defined as more than 200 copies/mL. For each cytology, the date and the result were registered according to Bethesda classification, and only the most severe cytology in a calendar year was included in the analysis. Cytology progression was defined as a change in cytologic severity from a negative result to LGSIL or HGSIL; from LGSIL to HGSIL; and from ASCUS to LGSIL/HGSIL. The change of a negative result to ASCUS alone, regardless of HPV infection, was not considered progression. A comparison between women with cytologic progression and women who did not progress was performed. For the HPV result, up to 2015, our institution performed detection of high-grade HPV subtypes by the hybrid capture II method, with results reported as high-risk HPV detected or not detected. Starting in 2016, the HPV test was performed using real-time polymerase chain reaction methodology (Roche, Cobas HPV test), with results reported as detection of HPV16, HPV18, or “Other High-Risk HPV”.
High-risk HPV detection by the hybrid capture II method or detection of either HPV16, HPV18, or “Other High-Risk HPV” in the polymerase chain reaction were considered a positive HPV test at all available timepoints during the study period. Because the HPV test was performed only in a subset of patients, HPV status was recorded as a separate variable and recorded throughout the entire follow-up period. A categorical variable representing the HPV status change throughout the study period was created for analyses. When HPV was reported at baseline, it was classified as “detected”. If it was reported at least once during the entire follow-up period excluding baseline, it was classified as “acquired”. When HPV was reported positive at baseline and negative during the follow-up period, it was classified as “regressed”. Finally, if HPV was negative at both baseline and during the entire follow-up period, it was classified as “not detected”. Only women with the HPV status categories “detected”, “not detected”, and “acquired” were included in the logistic regression model.
Statistical AnalysisStatistical analysis was conducted using SAS Studio Software version 9.4 (SAS Institute, Cary, NC). Mean and standard deviations were calculated for continuous variables such as age and years living with HIV. Frequencies were determined for categorical variables: race/ethnicity, HIV VL, AIDS status, history of smoking, history of STI, drug use, HPV infection status, and cytology progression. Overall results were reported as percentages of the total sample size. Variables were analyzed between cytology progression groups using the chi-square, Fisher exact test, or independent t test. Multivariate logistic regression modeling was performed to calculate adjusted odds ratios (aOR) and corresponding 95% confidence interval (CI) for progression to LGSIL/HGSIL. The multivariate model was adjusted for age, race/ethnicity, VL, HIV status, years living with HIV, history of smoking, drug use, and HPV status. All tests were 2-sided, and an α level of 0.05 was used for all statistical tests.
RESULTSA total of 162 medical records with a baseline cytology result from January 2010 to December 2012 were reviewed. These included all WLWH who had 1 initial negative cytology result (baseline) and 2 consecutive serial results. The mean age of the cohort was 44.8 years (±11 years). Forty-two percent were AA (n = 68), 30% were AC (n = 48), and 26% were Hispanics (n = 42). Centers for Disease Control and Prevention–defined AIDS status was reported in 75% of the women (n = 121). Most women in our cohort were receiving cART therapy (n = 157, 97%) (Table 2), and 21% presented a detectable HIV VL (n = 32). Comparison between ethnic groups at baseline showed that AA had the highest rate of AIDS (78%) and were significantly more likely to report the use of tobacco products (28%, p < .01) and substance use (24%, p < .01).
TABLE 2 - Patient Cohort Demographic and Clinical Characteristics (n = 162) Variable Total (N = 162) Age, years Mean ± SD 44.8 ± 11 Range 24–74 Race/ethnicity AA 68 (42) ACa 48 (30) Hispanic 42 (26) Other 4 (2) Receiving cART Yes 157 (97) No 5 (3) Detectable HIV VL (n = 156) VL ≤ 200 cp/mL 124 (79) VL > 200 cp/mL 32 (21) HIV status HIV-positive (not AIDS) 41 (25) CDC-defined AIDS 121 (75) Years living with HIV (n = 159) Mean ± SD 9.82 ± 6.82 Range 0.06–32.34 History of smoking Negative 136 (84) Positive 26 (16) Drug use Negative 144 (89) Positive 18 (11) History of STI Negative 158 (98) Positive 4 (2) HPV statusb (n = 138) Not detected 94 (68) Detected 16 (12) Acquired 20 (15) Regressed 8 (6) Cytology progressionb No progression 131 (81) Progression 31 (19)aAC includes 40 Haitians, 3 Bahamians, 3 Jamaicans, 1 St. Martiner, and 1 St. Lucian.
bAcross 5 y follow-up.
During the initial 2-year follow-up, 102 (63%) women remained negative in the cytology result, 47 (29%) had a result of ASCUS, and 13 (8%) had a result of LGSIL; we did not find any HGSIL results (Table 3). In addition, of the 138 women who underwent HPV testing, 36 (22%) had a positive result.
TABLE 3 - Cervical Cytology and HPV Diagnosis at Baseline and at 2-y Follow-Up Most severe cervical cytology (N = 162) N (%) Negative 102 (63) ASCUS 47 (29) LGSIL 13 (8) High-risk HPV status (N = 36) N (%) HPV positives at baseline 14 (39) HPV diagnosed at 1st year follow-up 17 (47) HPV diagnosed at 2nd year follow-up 5 (14)From the women who presented a cytology indicating ASCUS (n = 47, 29%) after a negative cytology in the first 2 years of follow-up, we report an ASCUS result in 60% (28/47) of women during the first year and 40% (19/47) in the second year. During the first year, other elements that were reported in the pathology result included excess bacteria in 14% (4/28); evidence of fungal infection in 11% (3/28); cellular evidence of inflammation in 11% (3/28); and evidence of cellular atrophy in 4% (1/28). During the second year, these other elements included excess bacteria in 21% (4/19), cellular evidence of atrophy in 11% (2/19), and fungal infection in 5% (1/19).
We compared the cohort by cytology progression (Table 4). A total of 31 (19%) women progressed to LGSIL/HGSIL across 5 years. In addition, 22% of AA (15/68) and 21% of AC (7/48) compared with 15% of Hispanics (9/42) progressed, showing that both AA and AC were found to have the highest rate of cytologic progression. This difference in proportion, however, was not statistically significant (p = .57). Human papillomavirus infection was detected in 30% (8/27) of women who showed cytologic progression compared with 7% (8/111) who did not progress, and HPV regression was found in 0% of women who progressed compared with 7% (8/111) who did not progress (p < .0001). Multivariate logistic regression showed that the probability of progression to LGSIL/HGSIL among women with a history of detected HPV across 5 years was greater than women with an undetected HPV (aOR = 5.11; 95% CI = 1.31–19.93; p < .02). Centers for Disease Control and Prevention–defined AIDS status was also associated with higher probability of cytologic progression compared with women without AIDS status (aOR = 4.28; 95% CI = 1.04–17.63; p = .04) (Figure 1). Other variables evaluated in the multivariate model such as age, race/ethnicity, VL, years living with HIV, history of smoking, and drug use were not associated with progression.
TABLE 4 - Patient Cohort Characteristics (n = 162) by Cytology Progression Across 5 y Variable Cytology progression p a Progression (N = 31) No progression (N = 131) Age, y .65 Mean ± SD 45.65 44.64 Range (25–70) (24–74) Race/ethnicity .57 AAb 15 (48) 53 (41) ACb 7 (23) 41 (31) Hispanicb 9 (29) 33 (25) Other — 4 (3) HIV VL (N = 30) (N = 126) .35 VL ≤ 200 cp/mL 22 (73) 102 (81) VL > 200 cp/mL 8 (27) 24 (19) HIV status .08 HIV-positive (not AIDS) 4 (13) 37 (28) CDC-defined AIDS 27 (87) 94 (71) Years living with HIV (N = 30) (N = 129) .98 Mean ± SD 9.79 ± 7.74 9.83 ± 6.61 Range (0.89–31.78) (0.06–32.34) History of smoking .28 Negative 24 (77) 112 (85) Positive 7 (23) 19 (15) Drug use .34 Negative 26 (84) 118 (90) Positive 5 (16) 13 (10) History of STI .58 Negative 30 (97) 128 (98) Positive 1 (3) 3 (2) HPV status (N = 27) (N = 111) <.0001 Not detected 14 (52) 80 (72) Detected 8 (30) 8 (7) Acquired 5 (18) 15 (14) Regressed — 8 (7)aChi-square, Fisher exact test, or independent t test.
bOnly these categories were included in the analysis.
 FIGURE 1:
FIGURE 1: Adjusted OR of cytology progression by patient baseline characteristics. AA indicates African American; AC, Afro-Caribbean.
Of the 102 women who remained negative at baseline and 2 years afterwards, 9 women (9%) progressed to LGSIL and 1 (1%) progressed to HGSIL before the recommended 3-year follow-up.
DISCUSSIONThe primary goal of our study was to determine the proportion of WLWH with cytologic progression to LGSIL/HGSIL in the 5-year follow-up period after a negative cytology. Other possible factors including race/ethnicity were also examined. To our knowledge, this is the first study using race/ethnicity as explanatory variable among a cohort of minority groups.
Since its inception, cervical cancer screening has evolved with an increased understanding of the natural history of HPV infection and its causal role in the development of cervical disease. Cytology, which was previously the hallmark of screening, has been highly effective in reducing the rates of cervical cancer in developed countries. However, HPV testing has consistently been shown to be highly sensitive in detecting CIN2+ lesions, and persistent HPV leads to virtually all cervical cancer.17 Furthermore, in women aged 25 to 65 years, primary HPV screening led to statistically significant increased rate of detection of CIN3+ lesions in the first round of screening in comparison cytology alone.18 Women living with HIV are reportedly 1.5 to 2.5 times more likely to be infected with HPV compared with HIV-negative women.11 Higher HPV acquisition, lower HPV clearance, and higher incidence of LGSIL and HGSIL leaves this group at heightened risk for HPV-related cancers.1 The Multicenter AIDS Cohort Study (MACS), one of the largest HIV cohorts in the United States, revealed significantly lower CD4 counts in HPV-related clinical conditions compared with those without HPV.19 At our institution, HPV positivity was an important risk factor that was associated significantly to progression to LGSIL/HGSIL. Alade et al.12 report similar results in a cohort of 325 WLWH aged 30 years as well as older WLWH with normal index cervical cytology and subsequent cytology results. Women living with HIV who tested positive for HPV were found to have higher likelihood of receiving a diagnosis of CIN2+ or higher within the next 4 years when compared with HPV-negative WLWH after adjusting for age, ethnicity, and CD4 levels (HR = 6.3; 95% CI = 1.7–23.2; p = .006).12 In addition, CDC-defined AIDS also predicted higher likelihood of cervical cytology progression. Because cervical cancer is considered an AIDS-defining disease, it is not surprising that more women with AIDS will progress to a higher severity in the cervical cytology.
A recent metanalysis reports that a higher nadir of CD4 counts in WLWH were associated with a 36% to 70% reduced risk of high-risk HPV and 36% to 80% reduced risk of CIN2+; cART was associated with a reduction in high-risk HPV persistence and histology-diagnosed CIN2+.20 Among WLWH who presented a cytology progression in our study, 52% did not have a positive high-risk HPV result, and only 1 progressed to HGSIL during the entire follow-up period. Furthermore, 97% of enrolled WLWH in our study were receiving cART, and 79% presented undetectable VL. Effective cART and VL suppression could have contributed to lower rates of HPV positivity among progressors seen in our cohort.
Despite the overall decrease in cervical cancer rates in the United States, racial disparities in health outcomes prevail and are well documented.14 Disaggregated data reveal that African American women have 60% higher incidence in cervical cancer compared with their Caucasian American counterparts.15 In comparison, Hispanic/Latina and non-Hispanic Black women are also reported to be diagnosed later with advanced stages of cervical cancer and have slightly higher mortality rates compared with non-Hispanic white women.21 These outcomes have been attributed to access to screening, socioeconomic, behavioral, and environmental factors. The possibility of biological factors such as molecular biological pathways distinctively driving aggressive outcomes in racially disparate populations have been described.15 The burden of HPV infection and poor cervical cancer outcomes are disproportionately affecting minority populations including those living with HIV. This study included a cohort of African American, non-Hispanic African Caribbean, and Hispanic women. The analysis of baseline characteristics among these 3 populations showed that African Americans were more likely to report a habit of smoking tobacco and drug use. It is well known that tobacco products increase the risk of developing cervical dysplasia22,23; however, there was no significant difference among these 3 populations in the rate of cytologic progression.
In 2019, 187.1/100,000 women were living with HIV in the United States.24 African Americans and Hispanics represent most of these statistics (785.4 and 202.5 women per 100,000, respectively).25 Miami-Dade County had the highest incidence rate of newly diagnosed HIV infections in the United States, with an incidence of 50.7/100,000 new cases in 2018.24 Various sociodemographic, behavioral, and social factors contribute to disparities in viral suppression among women and may also influence progression to cervical dysplasia such as early cART initiation and sustained adherence, which likely reduce incidence and progression of CIN.20 Our clinic serves a diverse minority Black population ranging from African Americans to immigrant women from Haiti, Jamaica, and other Caribbean islands. Haitians account for one of the largest foreign-born Black populations diagnosed with HIV/AIDS in the United States26 and are less likely to achieve viral suppression compared with African Americans and Hispanics after receiving cART.27 The Haitian population carries a higher burden of HPV, with a prevalence as high as 20.7%, with oncogenic strains (13.2% of the total Haitian population) accounting for most of these infections.28 As a result, the Haitian population experiences a high rate of cervical cancer, occurring in 38/100,000 women, 4 times higher than the rate in the general Florida population.29
The HIV virus is known to influence the HPV infection natural history by decreasing the host's immune response and suppression of HPV infections. Initial infection with HPV recruits dendritic cells, T cells, and macrophages while inhibiting Langerhans cells. A defect in the immune response ultimately leads to increased HPV acquisition, prevalence, persistence, and progression of disease.30 Certain HPV genotypes can potentially be less affected by the levels of immunosuppression in WLWH.31 At the moment, no recommendation exists on whether genotyping the HPV virus in these minority WLWH will positively impact diagnosis and treatment outcomes. This study establishes preliminary data supporting the usefulness of HPV testing in minority populations living with HIV.
In this cohort, a lower proportion of women were virally suppressed (21%). Moreover, during the entire follow-up period, women who progressed had a higher percentage of HIV VL (23%) compared with women who did not progress (15%); however, this difference was not significant.
LimitationsIt is necessary to highlight that this study was performed in an academic institution in the United States, where a large portion of the HIV+ population remain in sustained adherence to cART. This may contribute to low rates of detectable HIV VL and CIN overall because we found only 1 case of progression to HGSIL after 5 years follow-up. Because this study is retrospective in nature, not all clinical data and historical data were available for all women, and statistical analyses are limited to the available information in the database and the charts. In our institution, high-risk HPV testing was not commonly requested until 2012, and HPV typing was not done until 2016. High-risk HPV testing and HPV genotyping were performed based on individual provider judgment; therefore, these results are not available homogenously in all patients. Furthermore, data were not collected at the same timepoints for each participant, which limits the information available for analysis. The multivariate model focused on a subsample of patients who had HPV results available (n = 138). Given the small sample size, lack of statistical power may contribute to detect an effect for predictor variables. Comprehensive prospective studies with larger sample sizes assessing histologic changes and comparing time to progression to CIN2+ between potential predictor variables are needed to fully understand associated factors in this minority population.
ConclusionsAmong this cohort of minority women, HPV positivity was the single most significant factor predicting progression to LGSIL/HGSIL. Most of the LGSIL/HGSIL progressors in the cohort (68%) never converted to HPV positivity. Because South Florida remains the epicenter for new HIV infections, further studies are warranted to understand potential factors influencing cervical cancer incidence and outcomes in minority populations. Providers screening WLWH for CIN should carefully decide cytology screening intervals for ethnic minority populations. This study highlights the usefulness and importance of HPV testing in this population. As data supporting HPV testing in cervical cancer screening recommendations continue to evolve, HPV testing alone may be taken in consideration as a feasible screening option in WLWH.
ACKNOWLEDGMENTSA portion of this study was presented previously at the ASCCP 2017 Global Meeting, and full results presented at ASCCP 2020 Scientific Meeting on Anogenital and HPV-Related Diseases.
The authors also acknowledge partial support and assistance from Sylvester Comprehensive Cancer Center and The Miami Writing Center.
REFERENCES 1. Denny L, Boa R, Williamson AL, et al. Human papillomavirus infection and cervical disease in human immunodeficiency virus-1-infected women. Obstet Gynecol 2008;111:1380–7. 2. Firnhaber C, Van Le H, Pettifor A, et al. Association between cervical dysplasia and human papillomavirus in HIV seropositive women from Johannesburg, South Africa. Cancer Causes Control 2010;21:433–43. 3. Sezgin E, Van Natta ML, Thorne JE, et al. Secular trends in opportunistic infections, cancers and mortality in patients with AIDS during the era of modern combination antiretroviral therapy. HIV Med 2018;19:411–9. 4. De Vuyst H, Mugo NR, Chung MH, et al. Prevalence and determinants of human papillomavirus infection and cervical lesions in HIV-positive women in Kenya. Br J Cancer 2012;107:1624–30. 5. Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA 2002;287:2114–9. 6. Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. 2021 [cited 2021 Dec 15]; Available from: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/Adult_OI.pdf. 7. Rahatgaonkar VG, Deshpande AA, Oka GA. Screening for cervical cancer in HIV-infected women: a review of literature. Indian J Cancer 2021;58:317–7. 8. Wright TC Jr., Cox JT, Massad LS, et al. 2001 Consensus Guidelines for the Management of Women with Cervical Cytological Abnormalities. J Low Genit Tract Dis 2002;6:127–43. 9. Kaplan JE, Benson C, Holmes KK, et al. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recommendations and reports. Morbidity and mortality weekly report Recommendations and reports 2009;58:1–207; quiz CE1–4. 10. Blitz S, Baxter J, Raboud J, et al. Evaluation of HIV and highly active antiretroviral therapy on the natural history of human papillomavirus infection and cervical cytopathologic findings in HIV-positive and high-risk HIV-negative women. J Infect Dis 2013;208:454–62. 11. Liu G, Sharma M, Tan N, et al. HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer. AIDS 2018;32:795–808. 12. Alade RO, Vragovic O, Duffy C, et al. Human papillomavirus co-testing results effectively triage normal cervical cytology in HIV-positive women aged 30 years and older. J Low Genit Tract Dis 2017;21:125–8. 13. Nwangwu-Ike N, Frazier EL, Crepaz N, et al. Racial and ethnic differences in viral suppression among HIV-positive women in care. J Acquir Immune Defic Syndr 2018;79:e56–68. 14. Yu L, Sabatino SA, White MC. Rural-urban and racial/ethnic disparities in invasive cervical cancer incidence in the United States, 2010–2014. Prev Chronic Dis 2019;6:E70. 15. Olusola P, Banerjee HN, Philley JV, et al. Human papilloma virus-associated cervical cancer and health disparities. Cell 2019;8:622. 16. Masur H, Brooks JT, Benson CA, et al. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Updated Guidelines from the Centers for Disease Control and Prevention, National Institutes of Health, and HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis 2014;58:1308–11. 17. Dillner J, Rebolj M, Birembaut P, et al. Long term predictive values of cytology and human papillomavirus testing in cervical cancer screening: joint European cohort study. BMJ 2008;337:a1754. 18. Melnikow J, Henderson JT, Burda BU, et al. Screening for cervical cancer with high-risk human papillomavirus testing: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2018;320:687–705. 19. Ye Y, Burkholder GA, Wiener HW, et al. Comorbidities associated with HPV infection among people living with HIV-1 in the southeastern US: a retrospective clinical cohort study. BMC Infect Dis 2020;20:144. 20. Kelly H, Weiss HA, Benavente Y, et al. Association of antiretroviral therapy with high-risk human papillomavirus, cervical intraepithelial neoplasia, and invasive cervical cancer in women living with HIV: a systematic review and meta-analysis. Lancet HIV 2018;5:e45–58. 21. Moore de Peralta A, Holaday B, Hadoto IM. Cues to cervical cancer screening among U.S. Hispanic women. Hisp Health Care Int 2017;15:5–12. 22. Fonseca-Moutinho JA. Smoking and cervical cancer. ISRN Obstet Gynecol 2011;2011:847684. 23. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum 2004;83:1–1438. 24. Cent
留言 (0)