Bladder cancer is the 9th leading cause of cancer-related deaths worldwide, causing nearly 210.000 deaths each year [1]. Among possible risk factors for bladder cancer, infectious pathogens are of particular interest for their carcinogenesis properties. Since infectious agent-related cancers can be predictable and preventable by screening and vaccination programs [16]. However, to achieve this goal, the role of infectious pathogens in the development of specific cancers should be confirmed. Therefore, this study was performed to detect BKPyV and JCPyV in bladder cancer tissues and to screening for the presence of these viral pathogens among patients with bladder cancer. In this study, BKPyV and JCPyV were detected in 1.7% and 6.1% of the bladder cancer biopsy specimens, respectively.
The association between human polyomaviruses and bladder carcinoma continues to be controversial. While some studies suggested an association between BKPyV and JCPyV infections and bladder carcinoma [17,18,19], the other studies denied this association [3, 20,21,22]. These studies have been performed in different populations with different environmental risk factors and genetic backgrounds and have failed to reach a consensus. A recent study proposed the role of BKPyV in the development of bladder cancer via the anti-viral apolipoprotein B mRNA editing enzyme catalytic polypeptide (APOBEC)-mediated damage of the urothelial genome. In this hit-and-run mode of carcinogenesis, despite inducing APOBEC3B expression by LTAg of BKPyV, the causative viral agent is absent in the tumoral tissue probably due to immune clearance of BKPyV [23]. The present study, despite identifying BKPyV and JCPyV in a number of bladder cancer biopsy specimens in the South of Iran, suggests that these viruses are unlikely to be effective causative factors in bladder cancer in this region. Nevertheless, prospective cohort studies are needed to reach a more definite conclusion and to achieve further understanding of the association between BKPyV and JCPyV infections and the development of bladder cancer in an Iranian population.
The prevalence of 1.7% for BKPyV observed in this study is higher than that reported among patients with bladder cancer in Hungary (0.0%) [22] but lower than those reported in the United Kingdom (3.33%) [3], the United States (5.5%) [21], Mashhad (North-East of Iran) (13.7%) [24] and Italy (55%) [17]. Moreover, the prevalence of 6.1% for JCPyV observed in this study is higher than that reported among patients with bladder cancer in the United Kingdom (0.87%) [3] but lower than that reported in Italy (25%) [17]. These variations in the prevalence of human polyomaviruses in these studies could be due to differences in the type of specimen, processing methods, the sensitivity of the detection assays, and sociodemographic characteristics of the study population.
In this study, multiple samples from different parts of the tumoral tissue were tested for each patient. Since BKPyV and JCPyV may not infect all cancerous parts equally, testing the samples outside the infected site can lead to false-negative results. In addition, a nested PCR method was used to detect BKPyV and JCPyV in bladder tissue specimens. Due to the low number of copies of viral DNA in tissue specimens, a nested PCR assay is more useful for the detection of BKPyV and JCPyV than conventional PCR assays. So that all positive samples were identified in the second round of PCR. However, the risk of contamination, which leads to false-positive results, is higher in nested PCR assay than in one-step PCR assay [25]. In this study, to avoid contamination during PCR procedures, strict quality controls were applied. Moreover, positive and negative controls were used to ensure the accuracy of the results. Accidental contamination at the time of sample processing, which can lead to false-positive results, is another issue. During sectioning each sample, the necessary precautions were taken to avoid cross-contamination with the next sample.
In this study, the prevalence of BKPyV and JCPyV among patients with bladder cancer was not statistically associated with age, gender, place of residency, and the stage and grade of bladder cancer, although the majority of infected patients were in the age group 70–79 years, male, residents in Tangestan, stage Ta-T1, and low-grade and high-grade papillary urothelial carcinoma. Similarly, a study from the United Kingdom reported no association between the prevalence of BKPyV and JCPyV and stage and grade of the tumor [3]. Bladder cancer commonly affects older ages, with a peak incidence in the 7th and 8th decades of life, and is more common in men [17]. In this study, the mean age of patients increased with increasing the stage and grade of bladder cancer. So that patients in stage T2–T3 had a higher mean age compared to patients in stage Ta–T1. Moreover, patients with high-grade papillary urothelial carcinoma had a higher mean age compared to patients with urothelial papilloma.
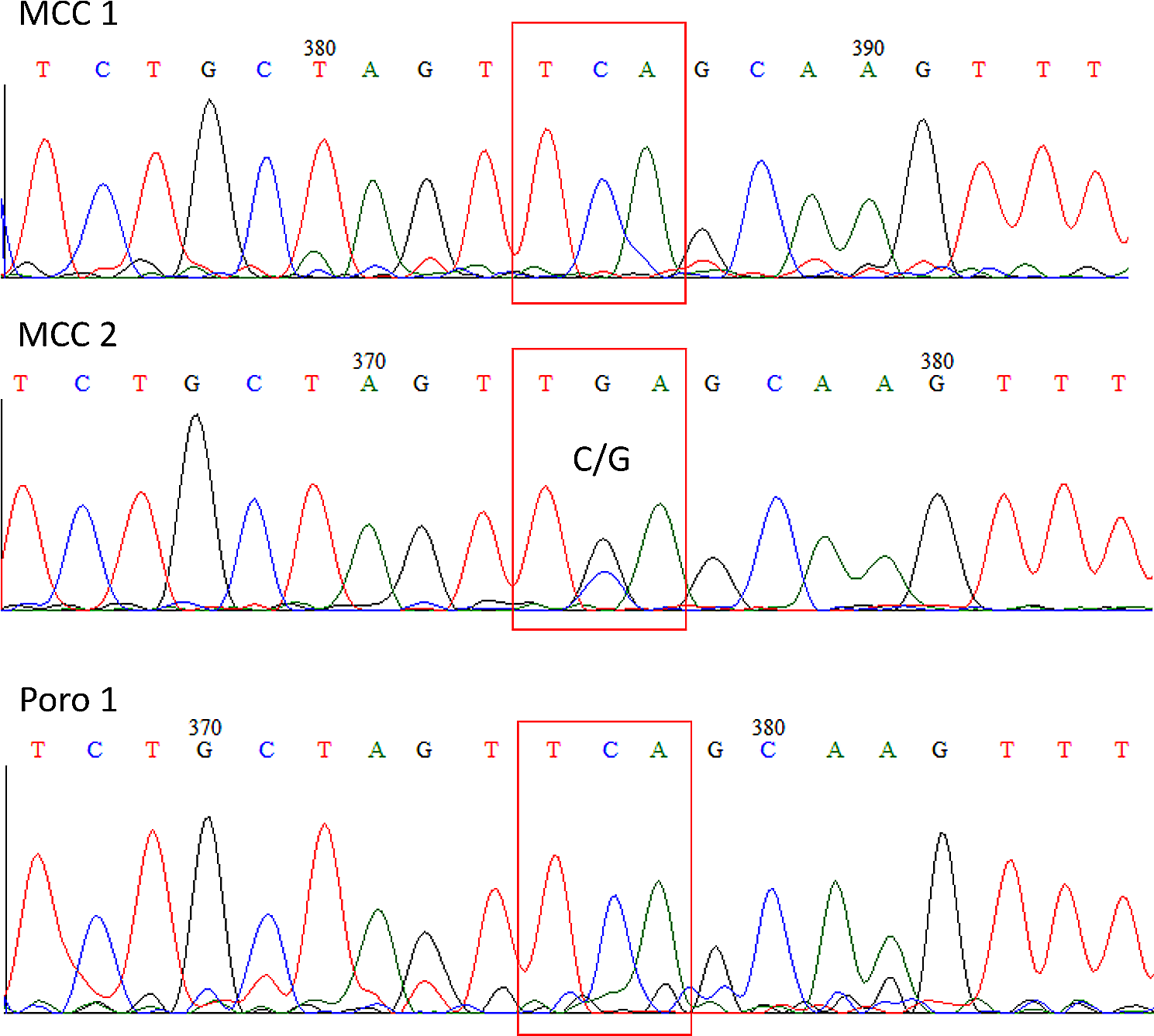
Based on the nucleotide sequence analysis of the VP1 region, the BKPyV genotypes I and IV and the JCPyV genotypes 2, 3 and 6 were found among patients with bladder cancer in this study. Currently, 4 BKPyV genotypes (I, II, III, and IV) with 4 subtypes related to genotype I (Ia, Ib-1, Ib-2 and Ic) and six subtypes related to genotype IV (IVa-1, IVa-2, IVb-1, IVb-2, IVc-1 and IVc-2), and 8 JCPyV genotypes (1–8) with 5 subtypes related to genotype 2 (2a, 2b, 2c, 2d and 2e) have been identified depending on the geographical distribution [7, 26]. The BKPyV genotype I shows a widespread distribution and is prevalent in different parts of the world. The BKPyV genotype IV is predominant in Asia. The BKPyV genotypes II and III are less prevalent and are almost rare [27, 28]. The JCV genotypes 1 and 4 are predominant in the United States and Europe. The JCV genotypes 2 and 7 are prevalent in Asia. The JCV genotypes 3 and 6 are the main genotype in Africa. The JCV genotype 5 is a recombination of genotypes 2b and 6. The JCV genotype 8 has been isolated from Papua New Guinea and Western Pacific populations [26].
We have carried out the largest screening of BKPyV and JCPyV to date in an Iranian population with bladder cancer, finding that these viruses are unlikely to be effective causative factors in bladder carcinogenesis among patients with bladder cancer resident in the northern shores of the Persian Gulf. In addition, data on BKPyV and JCPyV infections in bladder cancer, including distribution by age, gender, place of residency, tumor grade and tumor stage, were analyzed. Besides, the high number of screened samples increases the generalizability of the results to the population resident in this region. In addition, this study highlighted the importance of testing multiple samples from different parts of the tumoral tissue for each patient. In this study, due to the limited number of non-cancerous bladder samples in the archives of the pathology department of the hospitals and difficulties in acquiring healthy bladder samples, only 30 non-cancerous samples were screened for detection of BKPyV and JCPyV. The low number of control patients is one of the limitations of this study. As another limitation, paraffin-embedded tissue samples were used to detect BKPyV and JCPyV. The detection rate of viral DNA might be slightly higher in fresh frozen tissue samples compared to paraffin-embedded tissue samples.





留言 (0)