Summary
Electrotherapy neuromodulation (referred to as “neuromodulation” henceforth) has been used for pain management since ancient times. Scrobonus Largus, court physician to emperor Claudius, reported treatment of headaches with electric eels (4–100 V, 100 Hz) in 46–47 AD [13]. The era of modern neuromodulation is thought to have started in the 1960s with deep brain stimulation, followed by spinal cord stimulation, for intractable pain. Over the next 50 years, technological advances have significantly broadened the field of neuromodulation and impact on patient outcomes [6].
Current neuromodulation techniques for CPP target the sacral roots, pudendal nerve, mid-thoracic spinal cord, conus medullaris, and dorsal root ganglion (DRG) [6, 14, 15]. Unfortunately, given the complex nature of diagnosing CPP, it is increasingly common that patients are not evaluated by pain management specialists until unsuccessful treatment by two or more specialists from other fields (e.g., gynecology). By this point, CPP has often evolved into a chronic phase, rendering techniques including physical therapy, nerve blocks, radiofrequency lesions, and pharmacologic options increasingly ineffective. In such patients, neuromodulation may be the last bastion of potentially effective therapy. While the efficacy of neuromodulation for CPP often depends on adequate lead positioning, a lack of consensus exists with respect to the optimal target and location of leads [6].
Sacral Neuromodulation
Sacral neuromodulation (SNM) is an emerging minimally invasive treatment option for refractory CPP. SNM was first described by Tanagho and Schmidt in 1982 [16] and applied to human patients in 1988 [17]. Originally approved in 1997 by the US Food and Drug Administration (FDA) for urinary urge incontinence, urinary urgency-frequency, and non-obstructive urinary retention, SNM was eventually adopted for off-label usage in recalcitrant CPP [18]. SNM is an attractive treatment target in CPP given the role of the sacral nerve roots in relaying sensory information from the pelvic floor [19,20,21]. These sensory fibers may theoretically be subject to neuromodulation at any portion of the anatomical trajectory. In reality, caudal neuroanatomy is less mobile, less packed, and has a thinner insulating dorsal cerebrospinal fluid (CSF) layer relative to the conus medullaris and cauda equina. In addition, spatial representation of the distal sacral fibers diminishes in the cephalad direction; a stimulus may therefore preferentially recruit cephalad fibers. At the level of the thoracic spinal cord, sacral fibers are also smaller than lumbar fibers entering the dorsal column. The size discrepancy necessitates more energy to stimulate sacral fibers at the cost of indiscriminately stimulating thoracic fibers and inducing extraneous paresthesias. Thus, sacral nerve root stimulation may provide more selective pain modulation and stable delivery of electric pulses relative to cephalad structures [6, 19].
In 1997, a staged protocol involving a peripheral nerve evaluation (PNE) trial prior to permanent device placement was developed to identify favorable responders [22, 23]. Leads are typically inserted with local anesthesia and connected to an external temporary stimulator to allow for patient sensory responses. Trial duration generally lasts between 1 and 4 weeks and necessitates at least 50% symptomatic improvement to justify permanent SNM implant; a minimum 2-week trial period is recommended [22, 24, 25]. Success rates of PNE trials are typically around 50% with a reported range of 40–100% [24, 26]. Our review suggests a PNE success rate of 41–100% (Table 1). In studies that described lead arrangements, quadripolar leads were more utilized than octopolar leads and unilateral nerve roots were targeted more than bilateral nerve roots. Any roots from S1 to S4 were subject to neuromodulation with the most common target being unilateral S3 (Table 1).
Table 1 Summary of non-case reports for sacral neuromodulation in CPPOf the multitude of etiologies that underlie CPP, interstitial cystitis/bladder pain syndrome (IC/BPS) is the most well-documented indication for SNM (Table 1). In sum, 15 of 35 studies exclusively treated for this indication [21, 24,25,26,27,28,29,30,31,32,33,34,35,36,37]. Several studies did not characterize CPP by diagnosed etiology [13, 38,39,40,41,42]. Perineal or anorectal pain was reported in four studies [43,44,45,46].
Martellucci et al. reported pain outcomes in a population of patients with CPP and prior pelvic surgeries [13]. Falletto et al. documented outcomes of SNM in patients with chronic anal and perianal pain [46] Sokal et al. applied SNM to patients with idiopathic CRPS and failed-back surgery syndrome [47]. Less common indications included vulvodynia [20, 48], coccydynia [48], severe endometriosis [49], postsurgical neuropathic pain [48], actinic proctitis [48], sacroiliac joint dysfunction [50], dyspareunia [50, 51], clitoral pain after abdominal surgery [52], and cauda equina syndrome [51] (Table 1).
Lead placement strategies are broadly stratified into percutaneous (retrograde, anterograde, and transforaminal) and open approaches. The retrograde, also known as cephalocaudal, approach has been described as the standard technique for SNM implantation [6, 19] and entails lumbar epidural puncture with caudal advancement of electrodes. Unfortunately, this approach has a relatively high technical failure rate as advancement in the sacral promontory is frequently impossible [48]. Additionally, the retrograde approach lends itself to an increased risk of dural puncture, intrathecal lead placement, and cerebrospinal fluid leak. Reported stimulation parameter ranges include amplitude of 0.8–1.6 V, frequency of 30–50 Hz, and pulse width of 350–450 μs [53]. In our review, five studies described the retrograde approach [13, 20, 21, 27, 51]. Stimulation parameters were described in three of these studies and were variable (Table 1) [13, 20, 51].
In contrast, the anterograde, also known as the caudal or trans-hiatal, approach is technically easier and entails needle advancement under fluoroscopic guidance through the sacral hiatus. The risk of dural puncture is decreased compared to the retrograde approach. Leads emerging from the needle often need to be advanced a short distance to the nerve roots. However, the thin subcutaneous layer overlying the sacral hiatus often makes lead anchoring difficult and increases the risk of skin erosion. The anterograde approach has raised concerns regarding implant sterility and risk of infection [6, 48, 53]. In total, six studies described the anterograde approach [20, 38, 45, 47, 48, 50]. Stimulation parameters were described in two cases reports, of which only one mentioned voltage (Table 2). Parameters included amplitude of 1–10.5 V, frequency of 60–1200 Hz, and pulse width of 20–300 μs [20, 50].
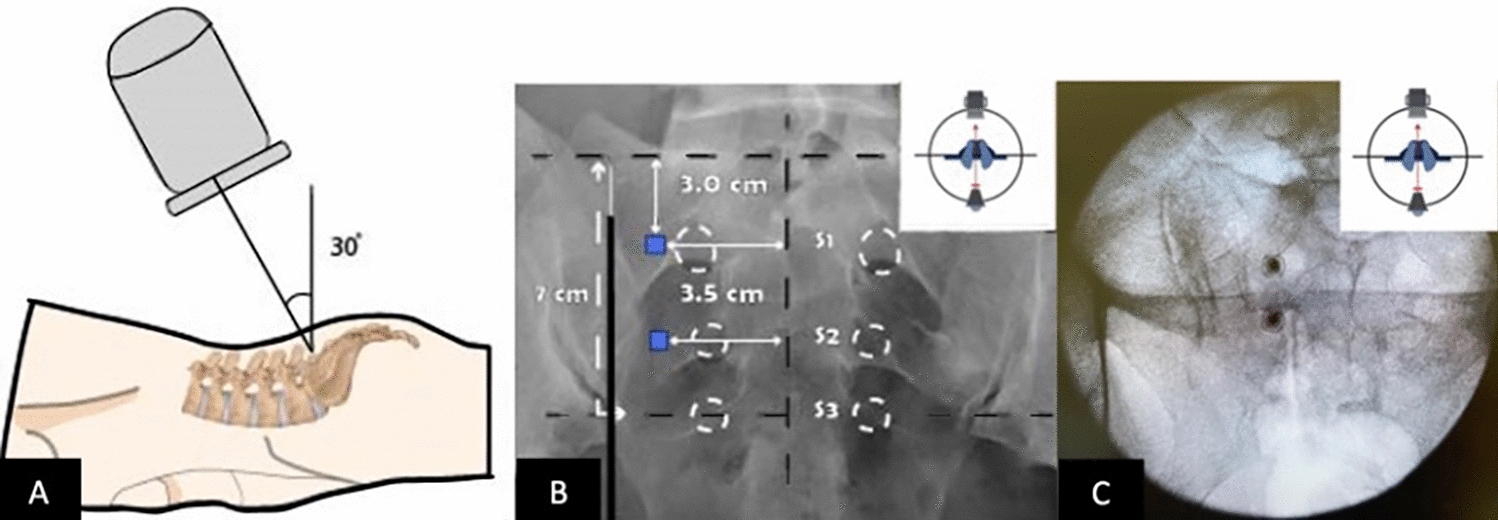
Table 2 Characteristics of selected case reports on sacral neuromodulationThe third method is the transforaminal approach, usually targeting the S3 nerve root, which is technically easier and has been widely adopted in staged SNM. The approach has a reduced risk of dural puncture and skin erosion but at the cost of a higher incidence of reprogramming and lead migration due to challenges with anchoring. Anterior lead positions also tend to stimulate motor fibers and may generate uncomfortable paresthesias. Tined leads have improved fixation success [54, 55]. Previously reported stimulation parameters include amplitudes of 0.8–1.0 V, frequencies of 25–30 Hz, and pulse width of 180–210 μs [53, p. 200]. In total, 17 studies employed the transforaminal approach [24, p. 2; 25, 28,29,30,31,32,33,34,35, 40, 41, 46, 49, 51, 53, 56]. Stimulation parameters were described in eight studies (Table 1) with amplitude of 1–9 V, frequency of 14–54 Hz, and pulse width of 200–300 μs. Notably, Marinkovic et al. compared long-term pain outcomes in patients who underwent neuromodulation with low voltage (less than or equal to 3 V) to high voltage (at least 4 V) [35].
The final approach is open surgery, which is often a last resort and has been largely replaced by the aforementioned minimally invasive alternatives. Open surgery has previously been described as placing paddle leads unilaterally or bilaterally following a partial L5–S1 laminectomy. Leads are advanced caudally beneath the dorsal sacrum to overlay the S2–S4 roots. Paddle leads may provide broader paresthesia coverage. Stimulation parameters are typically set to lower amplitudes and higher frequencies [










留言 (0)